
Abstract
Study Design
Systematic review.
Objective
To compare the effectiveness and safety between iliac crest bone graft (ICBG), non-ICBG autologous bone, and allograft in cervical spine fusion. To avoid problems at the donor site, various allograft materials have been used as a substitute for autograft. However, there are still questions as to the comparative effectiveness and safety of cadaver allograft compared with autologous ICBG.
Methods
A systematic search of multiple major medical reference databases was conducted to identify studies evaluating spinal fusion in patients with cervical degenerative disk disease using ICBG compared with non-ICBG autograft or allograft or non-ICBG autograft compared with allograft in the cervical spine. Radiographic fusion, patient-reported outcomes, and functional outcomes were the primary outcomes of interest. Adverse events were evaluated for safety.
Results
The search identified 13 comparative studies that met our inclusion criteria: 2 prospective cohort studies and 11 retrospective cohort studies. Twelve cohort studies compared allograft with ICBG autograft during anterior cervical fusion and demonstrated with a low evidence level of support that there are no differences in fusion percentages, pain scores, or functional results. There was insufficient evidence comparing patients receiving allograft with non-ICBG autograft for fusion, pain, revision, and functional and safety outcomes. No publications directly comparing non-ICBG autograft with ICBG were found.
Conclusion
Although the available literature suggests ICBG and allograft may have similar effectiveness in terms of fusion rates, pain scores, and functional outcomes following anterior cervical fusion, there are too many limitations in the available literature to draw any significant conclusions. No individual study provided greater than class III evidence, and when evaluating the overall body of literature, no conclusion had better than low evidence support. A prospective randomized trial with adequate sample size to compare fusion rates, efficacy measures, costs, and safety is warranted.
Keywords
Introduction
Anterior cervical fusion is a safe and effective surgery that continues to experience a rapid increase in utilization. In the United States, cervical fusions increased by 89% from 1993 to 2003, 1 and doubled again between 1998 and 2008. 2 In these cases, surgeons and patients are faced with many decisions, including the choice of bone graft material. Several options are now available, yet autologous iliac crest bone grafting (ICBG) is still considered the gold standard.3,4 However, some morbidity is associated with ICBG harvesting that can include infection, hematoma, fracture, wound healing, and donor site pain.5–9
To avoid problems at the iliac crest donor site, other autologous bone has been advocated as a suitable graft material such as local bone and fibular bone.10–13 In addition, various allograft materials have been used as a substitute for autologous ICBG. In fact, national trends point to decreased utilization of autograft (86 to 10%) with a reciprocal increase in allograft (14 to 59%) from 1998 to 2004. 14 However, questions remain as to the comparative effectiveness and safety of other types of autograft and cadaver allograft compared with autologous ICBG. Therefore, the purpose of this review was to explore the following key questions:
Is autologous ICBG safer and more effective than fusion with other types of autograft in the cervical spine?
Is autologous ICBG safer and more effective than cadaver allograft in the cervical spine?
Is non-ICBG autograft safer and more effective than cadaver allograft in the cervical spine?
Materials and Methods
Electronic Literature Search
Medline, Embase, and the Cochrane Collaboration Library were systematically searched for literature published through December 21, 2015. The search was limited to studies published in the English language that used human subjects and had abstracts available (see
Studies were excluded if they did not report results separately by treatment group, used a mixed graft such as demineralized bone matrix, or included skeletally immature patients (<18 years of age) or patients with a history of tumor or infection in the implantation site, trauma, fracture, or adolescent scoliosis. Studies with a very small sample size (n < 10) for either comparison group were not included. Animal, cadaver, and biomechanical studies were also excluded.
Data Extraction
The following data was extracted: (1) study design, (2) patient characteristics, (3) interventions, (4) inclusion and exclusion criteria, (5) follow-up duration, (6) the rate of follow-up for each treatment group (if reported or calculable), (7) patient-reported functional and pain outcomes (Oswestry Disability Index, visual analog scale, Japanese Orthopaedic Association Score and Scale, Roland-Morris score, Modified MacNab score, or patient satisfaction), (8) various clinical outcomes defined by the investigators, (9) complications or adverse events, (10) fusion rate, (11) time to fusion, (12) definition of fusion, (13) area where bone graft was harvested, (14) type of bone used (i.e., cancellous), (15) preparation methods (i.e., morselization), and (16) preservation method (i.e., freeze-dried or frozen). In the absence of patient-reported or clinical outcomes, radiographic or clinician-defined fusion was used to determine success. Fusion percentages were compared at final follow-up because follow-up times were reported inconsistently across the studies. All extracted data was examined for trends and possible pooling.
Study Quality and Overall Strength
The risk of bias was assessed for each article using criteria set by The Journal of Bone & Joint Surgery, American Volume for therapeutic studies and modified to delineate criteria associated with methodological quality described elsewhere (see
After individual article evaluation, the strength of the overall body of evidence with respect to each outcome was determined based on the precepts outlined by the Grades of Recommendation Assessment, Development and Evaluation (GRADE) Working Group and recommendations made by the Agency for Healthcare Research and Quality (AHRQ).17–19 Qualitative analysis was performed considering AHRQ-required and additional domains.
When the majority of the studies were randomized controlled trials, the initial strength of the overall body of evidence was considered high, and low if otherwise. Published evidence could be downgraded based on the inconsistency of results, indirectness of evidence, imprecision of the effect estimates (e.g., wide confidence intervals), or not having an a priori statement of subgroup analyses. Alternatively, the body of evidence could be upgraded one or two levels if there was a large magnitude of effect or dose–response gradient.
The final overall strength of the body of literature expresses our confidence (high, moderate, or low) that the effect size lies close to the true effect and the extent to which it is believed to be stable based on the adequacy or deficiencies in the body of evidence. A rating of insufficient means that we have very little confidence in the effect estimate; the true effect is likely to be substantially different than the estimated effect. In addition, this rating was used when there was no evidence or it was not possible to estimate an effect.
Data Analysis
The data was then summarized in tables and further stratified based on the graft tissue preparation and preservation method. The mean differences and variance between baseline and follow-up values were calculated for available continuous variables. Risk proportions (percents) were determined for dichotomous variables by tallying risks as the proportion of patients experiencing an event. When the complication risk was greater in one treatment group compared with another, we calculated the risk ratio and 95% confidence interval using STATA 9.0 (StataCorp., College Station, Texas, United States).
Results
Study Selection
The search strategy yielded 136 potentially relevant citations. Of these, 112 were excluded based on title and/or abstract. Twenty-four were selected for full text review. An additional 11 were excluded based on full text review for the following reasons: not a comparison of interest (n = 4), not a population of interest (n = 3), n < 10 for each group (n = 2), or not a study type of interest (n = 2; see
Evidence Available
There was no evidence found for key question 1, comparing autologous ICBG with other types of autograft in the cervical spine. The majority of the publications identified supported key question 2, which included two prospective20,21 and nine retrospective cohorts.22–30 Further details are presented in
Characteristics of included cervical fusion studies by key question
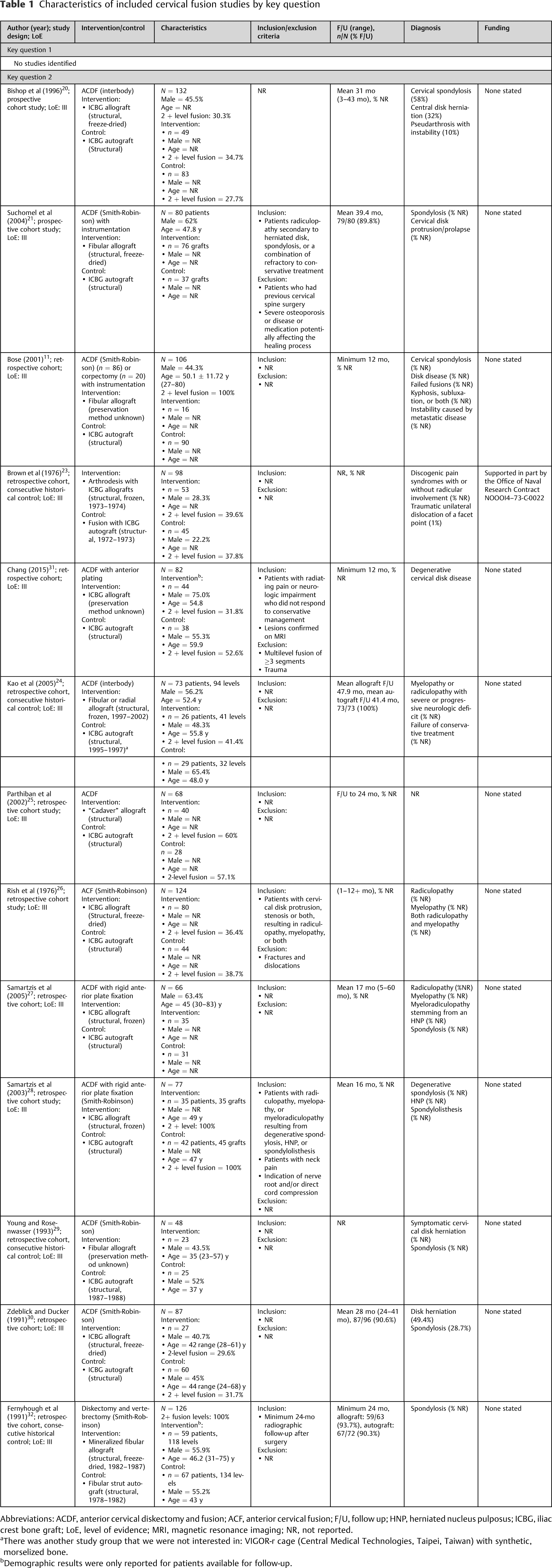
Abbreviations: ACDF, anterior cervical diskectomy and fusion; ACF, anterior cervical fusion; F/U, follow up; HNP, herniated nucleus pulposus; ICBG, iliac crest bone graft; LoE, level of evidence; MRI, magnetic resonance imaging; NR, not reported.
aThere was another study group that we were not interested in: VIGOR-r cage (Central Medical Technologies, Taipei, Taiwan) with synthetic, morselized bone.
bDemographic results were only reported for patients available for follow-up.
Efficacy/Effectiveness
Key Question 1—Iliac Crest Bone Grafting versus non–Iliac Crest Bone Grafting Autograft
There was no evidence found.
Key Question 2—Iliac Crest Bone Grafting versus Allograft
All but one study showed similar fusion percentages across the groups (
Fusion (%) comparing ICBG with allograft in the cervical spine
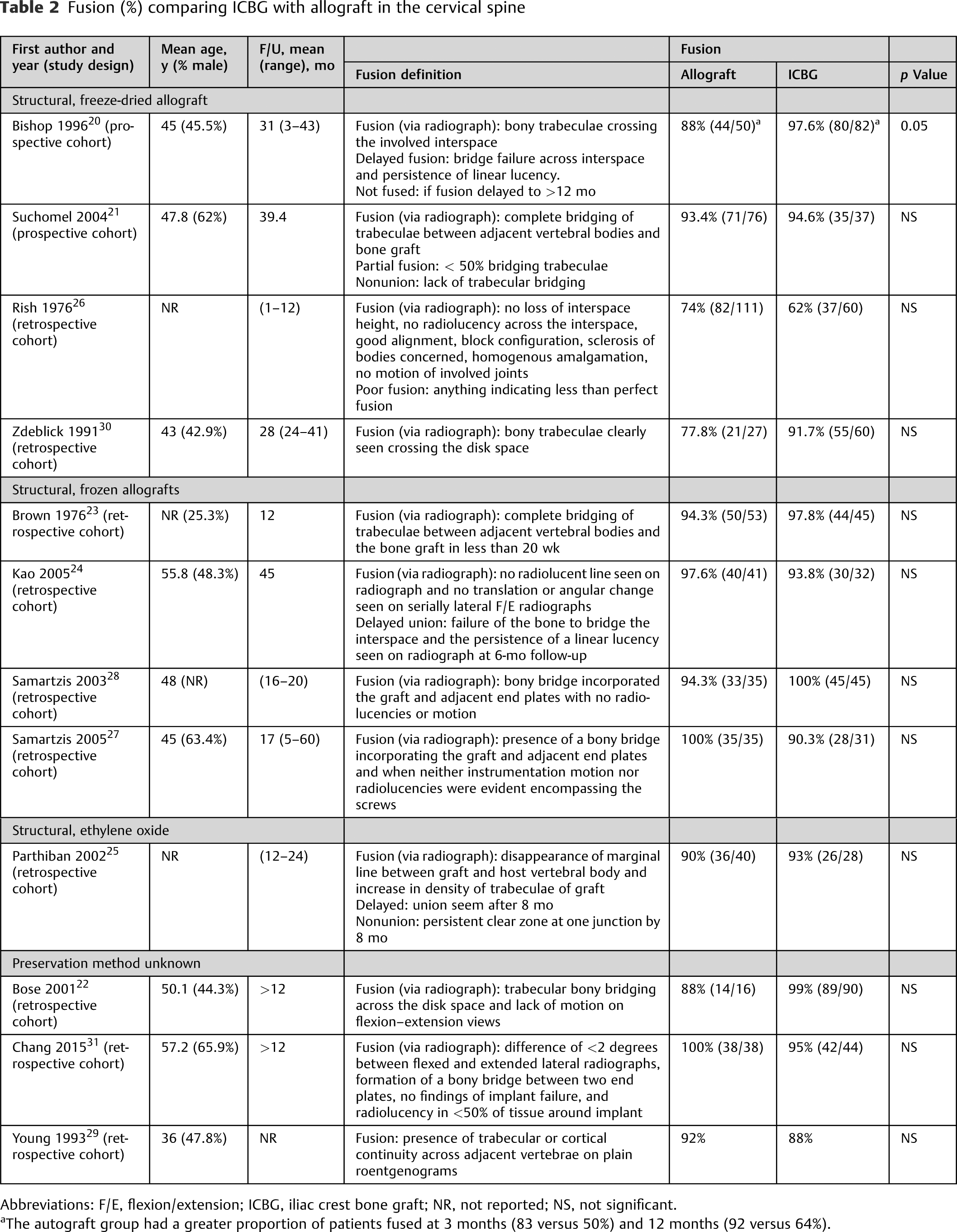
Abbreviations: F/E, flexion/extension; ICBG, iliac crest bone graft; NR, not reported; NS, not significant.
aThe autograft group had a greater proportion of patients fused at 3 months (83 versus 50%) and 12 months (92 versus 64%).
Two studies included cervical pain outcomes.30,31 One reported no differences in the proportion of patients with mild cervical pain between the allograft group (7%) and ICBG group (5%) at final follow-up. The second reported no difference between groups in the percent improvement in pain from baseline to follow-up: 58.9% in the allograft group compared with 54.1% in the ICBG group. 31
There were no significant differences noted for outcome measures of clinical success in studies comparing allograft to autologous ICBG for cervical fusion (Odom's criteria, neck disability index, clinical success;
Pain and clinician-based and patient-reported outcomes following ICBG compared with allograft in cervical spinal fusion
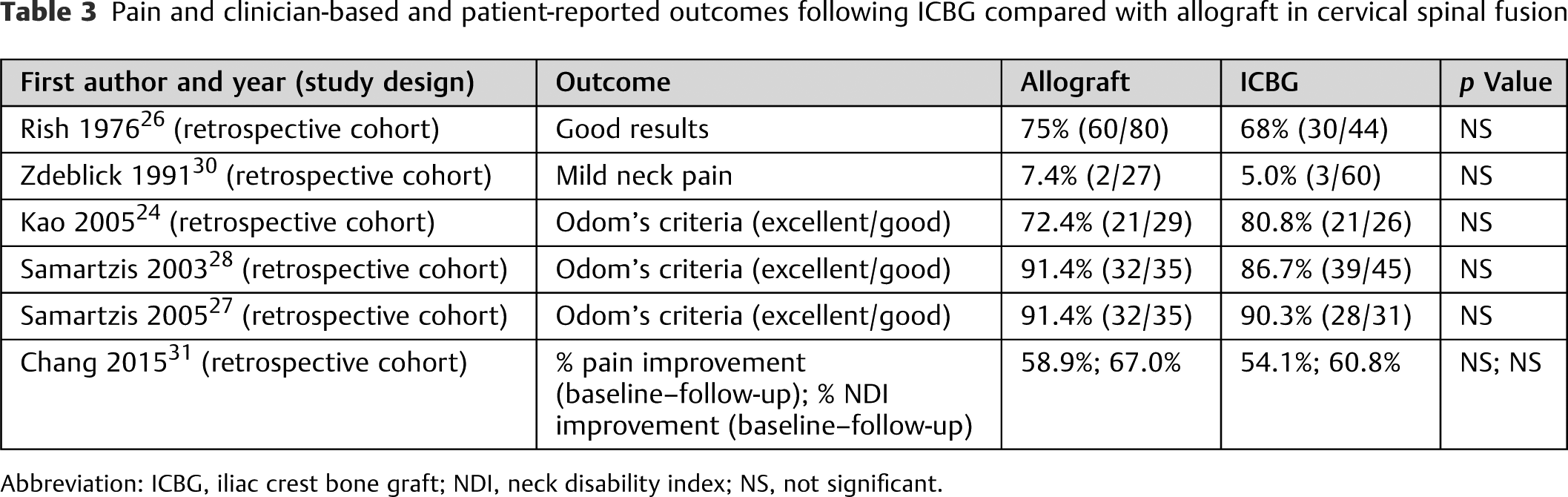
Abbreviation: ICBG, iliac crest bone graft; NDI, neck disability index; NS, not significant.
Key Question 3—Non–Iliac Crest Bone Grafting Autograft versus Allograft
In the single publication that addressed key question number 3, the fibular strut autograft group (98/134, 73%) demonstrated a better fusion rate than the freeze-dried fibular allograft group (70/118, 59%; p < 0.01). Mean follow-up was reported to be greater than 24 months. The study did not include axial or radicular pain outcomes. 32
Safety
Key Question 1—Iliac Crest Bone Grafting versus non–Iliac Crest Bone Grafting Autograft
There was no evidence found.
Key Question 2—Iliac Crest Bone Grafting versus Allograft
Donor site complications among patients who received autologous ICBG varied across studies (
Complications at final follow-upa comparing allograft versus ICBG in cervical fusion
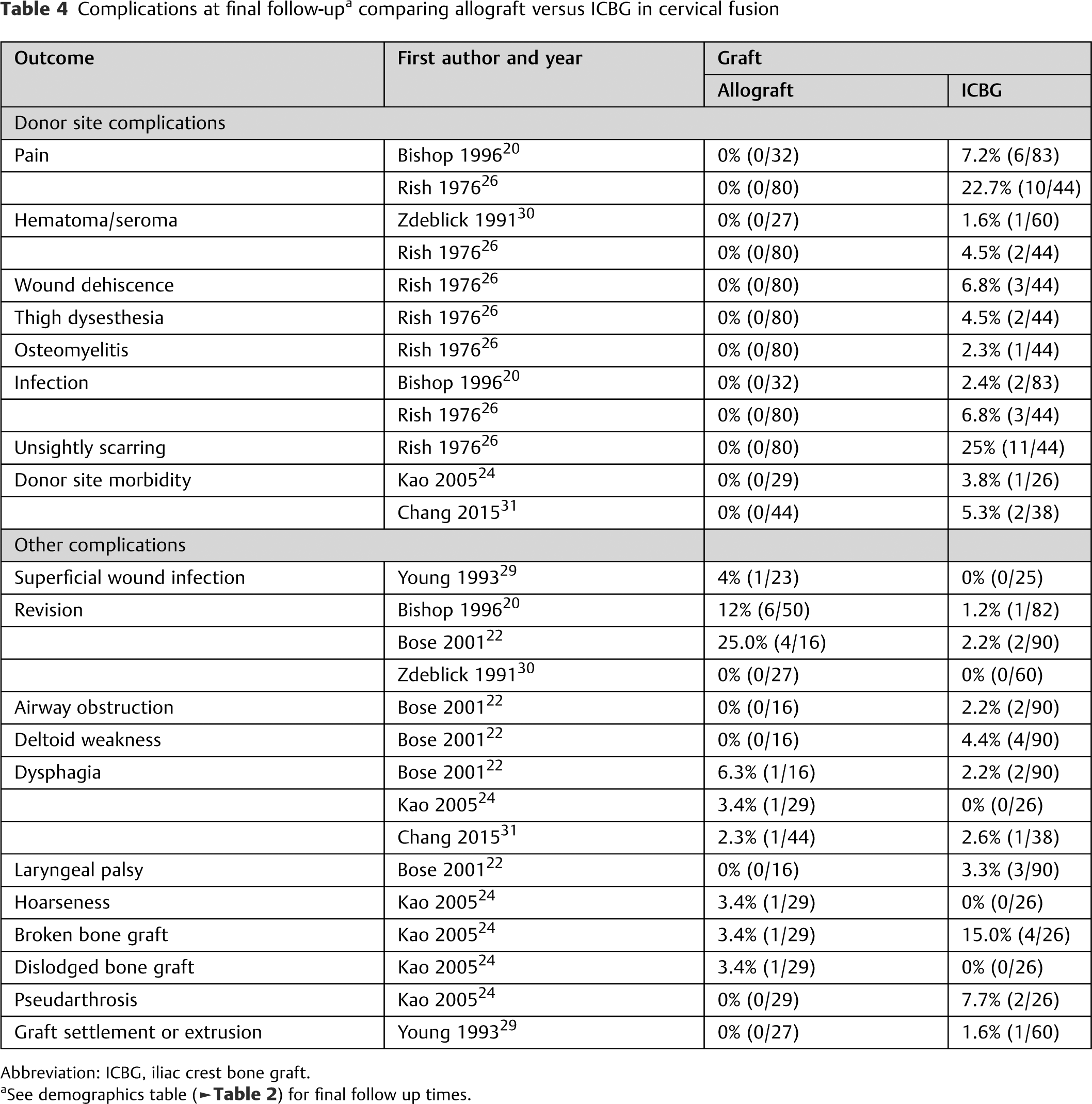
Abbreviation: ICBG, iliac crest bone graft.
aSee demographics table (
Key Question 3—Non–Iliac Crest Bone Grafting Autograft versus Allograft
Safety outcomes for key question 3 were not reported.
Evidence Summary (
Table 5
)
Summary of quality of evidence: ICBG autograft compared with allograft in the cervical spine (key question 2)
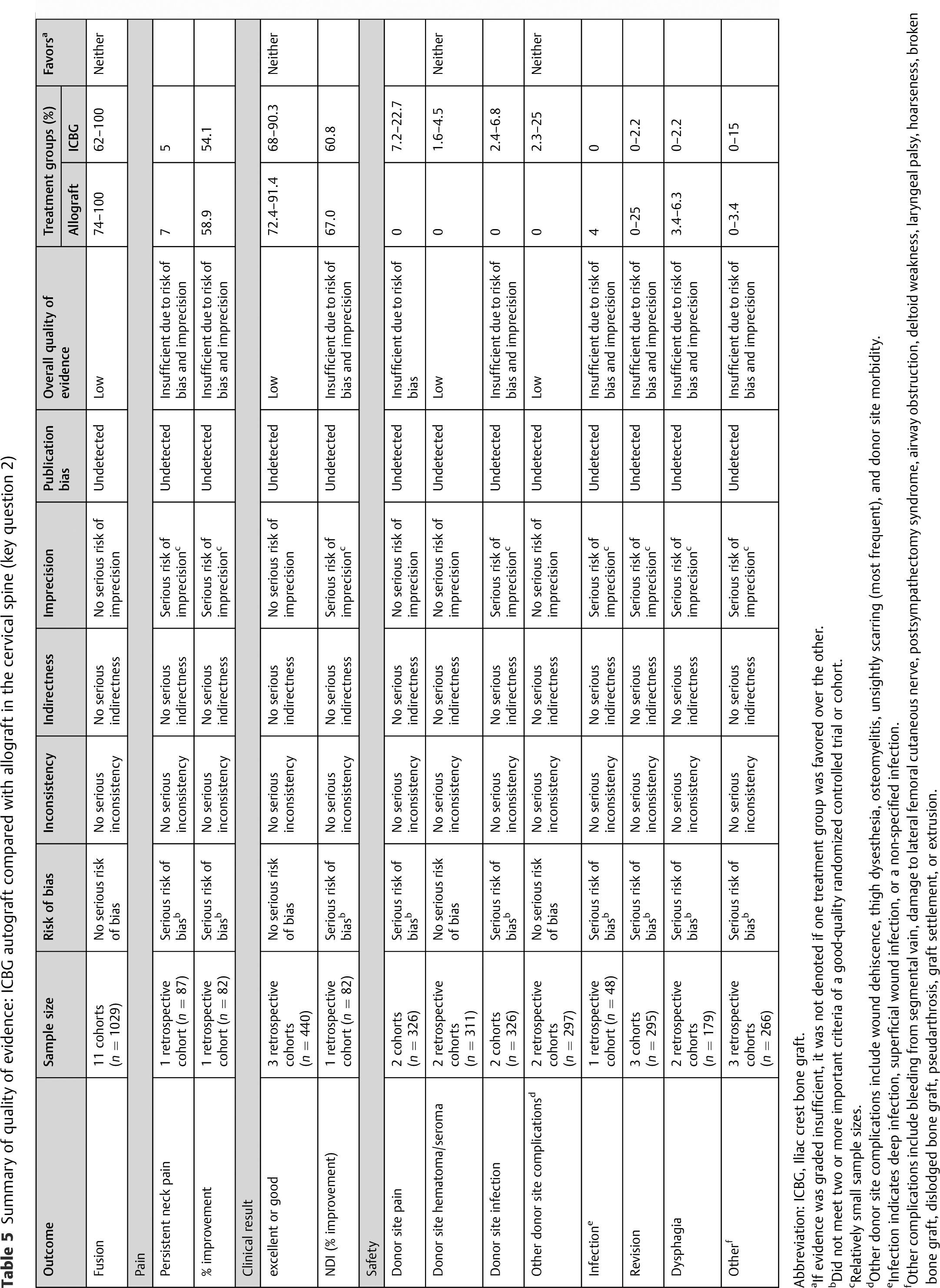
Abbreviation: ICBG, Iliac crest bone graft.
aIf evidence was graded insufficient, it was not denoted if one treatment group was favored over the other.
bDid not meet two or more important criteria of a good-quality randomized controlled trial or cohort.
cRelatively small sample sizes.
dOther donor site complications include wound dehiscence, thigh dysesthesia, osteomyelitis, unsightly scarring (most frequent), and donor site morbidity.
eInfection indicates deep infection, superficial wound infection, or a non-specified infection.
fOther complications include bleeding from segmental vain, damage to lateral femoral cutaneous nerve, postsympathectomy syndrome, airway obstruction, deltoid weakness, laryngeal palsy, hoarseness, broken bone graft, dislodged bone graft, pseudarthrosis, graft settlement, or extrusion.
Key Question 1—IIliac Crest Bone Grafting versus non–Iliac Crest Bone Grafting Autograft
There was no evidence comparing patients who had received non-ICBG autograft versus ICBG autograft in the cervical spine.
Key Question 2—Iliac Crest Bone Grafting versus Allograft
There was low evidence to support no difference between ICBG and allograft in terms of fusion rates and clinical result.
Though donor site pain and hematoma/seroma occurred more frequently in the ICBG autograft group, there is insufficient evidence to state with reasonable certainty what proportion of patients will experience pain at the donor site due to serious risk of bias in the included studies. There is low evidence around the estimated percent of patients with donor site hematoma/seroma following ICBG harvesting, ranging from 1.6 to 4.5%. There is also low evidence for other donor site complications such as wound dehiscence, thigh dysesthesia, osteomyelitis, unsightly scarring (most frequent), and donor site morbidity occurring more frequently in the ICBG autograft group, ranging from 2.3 to 25% of patients.
Key Question 3—Non–Iliac Crest Bone Grafting Autograft versus Allograft
Only one retrospective cohort study using historical controls that were not applied equally met the inclusion criteria of this review. Thus, the evidence for fusion success, pain, and functional and safety outcomes were deemed insufficient due to imprecision.
Discussion
Based on the current data, during anterior cervical fusion no consistently reported differences in fusion rates or patient outcomes were identified when utilizing autologous ICBG versus allograft. The current state of the published literature is insufficient to comment on the comparative safety of these two graft types or to make any distinctions between ICBG and non-ICBG autograft or non-ICBG autograft and allograft.
Autologous bone graft exhibits many properties that give it theoretical benefits over other materials including its osteoinductive and osteoconductive properties, as well as its inherent growth factors and osteogenic cells that are native to the patient and thus represent lower immune or infection risk. 3 In contradistinction, the overall body of clinical literature failed to show a benefit in terms of long-term fusion rates when comparing ICBG to allograft for anterior cervical fusion. Fusion rates using ICBG or allograft are by far the best-characterized outcome in the literature with 11 studies reporting data on 1,029 patients. But even these publications had limitations in study design that could affect the conclusions. No study had an initial level of evidence rating greater than class III, and all studies had at least one further limitation in relation to lack of blinding, inequality of intervention application, unacceptably high rates of loss to follow-up, inadequate sample size, or lack of control for confounders. Finally, each study had a distinct definition of fusion with no study routinely utilizing computed tomography scan and only five using flexion–extension radiographs.22,24,26–28,33
In interpreting the results of this review regarding fusion rates of allograft versus autograft, it is important to recognize that other patient factors and surgical techniques play a role in the outcome of cervical fusion surgery. Anterior cervical plating has been shown to significantly increase the fusion rate. A meta-analysis by Fraser and Härtl et al found superior fusion rates with anterior cervical plating compared with uninstrumented interbody fusion. 34 Furthermore, there is evidence that the type of plating system can affect fusion rates.35–38 Only half of the included studies provided information on the use of cervical instrumentation. Four studies used a fixed plating system,21,22,27,28 and two studies stated no instrumentation was used.20,24 It is important to note that the one study that reported a difference in fusion rates between ICBG and allograft did not use instrumentation, 20 and the study reporting superiority of fibular strut autograft over allograft did not report on the use of instrumentation. 32 Other operative factors such as adequate end plate preparation and decortication can also have an effect on achieving fusion. 39 Patient-related factors such as age, osteoporosis, and tobacco use all seem to have an effect on the fusion rate as well.3,20,40
The main limitation of ICBG for cervical fusion is the remote surgical site required for harvest and the associated morbidity reported to be as high as 22% with up to 90% of patients complaining of donor site pain,41,42 although recent studies have reported significantly lower complication rates especially with allograft reconstruction.43–45 Consistent with the overall body of literature, higher rates of donor site complications, such as donor site pain, hematoma/seroma, wound dehiscence, thigh dysesthesias, osteomyelitis, infection, and unsightly scarring, were found in all the pertinent studies related to cervical fusion; however, the overall quality of the evidence related to most donor site complications using the GRADE and AHRQ guidelines was deemed insufficient to draw any conclusion comparing ICBG and allograft. The exceptions were the donor site hematoma or seroma group and the “other” donor site complications groups where there was low evidence of no statistically significant difference between the two interventions. This result likely represents a type II error as few studies reported complications and those that did tended to have low morbidity rates leading to a small sample available for analysis.
Though using an allograft removes the donor site risks from the patient while maintaining osteoconductive properties, it tends to incorporate more slowly, leading to longer times to fusion, and it is associated with higher direct costs. 4 Furthermore, there are concerns that immunologic mismatch or inflammatory reactions to the products used to prepare and sterilize the allograft can put a patient at increased risk for complications.3,4,20 The preparation process required of the allograft prior to implantation has been reported to weaken it,46–49 hinting at a mechanism for loss of correction or even revision surgery. It should also be noted that there have been extremely rare infection risks associated with allograft including 2 cases of human immunodeficiency virus, 3 cases of viral hepatitis, and 26 bacterial infections.50–53
This study highlights significant limitations in the available literature and multiple avenues for further study with respect to graft choice for anterior cervical fusion. There is insufficient evidence to compare the safety and efficacy of cervical fusion when using ICBG versus non-ICBG autograft (key question 1) and non-ICBG autograft versus allograft (key question 3). Although 11 total cohorts directly compared cervical fusion with ICBG autograft versus allograft, no studies were randomized and only two studies collected data prospectively. Furthermore, there was little consistency between studies with regards to follow-up time, definition of fusion, and reporting of outcomes and complications. This inconsistency significantly limited our ability to pool the data and perform a formal meta-analysis. Thus the overall quality of the existing literature comparing these two graft types remains limited. Future studies on this topic should be aimed at comparing efficacy measures, direct and indirect costs, and safety in a prospective fashion. Future study design must include sufficient power to assess clinically relevant complications, adequate long-term follow-up, and a reliable and reproducible method to define fusion.
Conclusion
The best available evidence weakly suggests that ICBG and allograft demonstrated similar effectiveness in terms of fusion rates, pain scores, and functional outcomes following anterior cervical fusion. However, significant limitations in the available literature were obvious. Therefore, definitive judgments or suggestions with respect to the use of ICBG or allograft should be made carefully and within the framework of the current literature. At this time, ICBG versus other fusion methods remains an area of clinical equipoise and thus is not only an interesting area for further investigation but necessary. A well-designed randomized controlled trial comparing ICBG and allograft for anterior cervical fusion is warranted to address questions related to differential fusion rates, clinical efficacy, cost, and safety.
Footnotes
Disclosures
Alexander Tuchman: Grant (NuVasive)
Darrel S. Brodke: Royalties (Amedica, Depuy Synthes, Medtronic)
Jim A. Yousef: Consultant (NuVasive, Integra, Amedica, HealthTrust); Royalties (NuVasive, Osprey Medical, Integra, Amedica)
Hans-Joerg Meisel: Consultant (Zyga, Difusion, Codon); Royalties (Medtronic, Aesculap, Fehling)
Joesph R. Dettori: Personal fees (AOSpine North America, Cervical Spine Research Society)
Jong-Beom Park: none
S. Tim Yoon: Consultant (ISSLS, Stryker, Meditech); Grant (Biomet, NIH, Pfizer); Royalties (Stryker, Biomet, Meditech); Stock ownership (Alphatec, Phygen, Medyssey, Meditech)
Jeffery C. Wang: Personal fees (AO Foundation, NASS, CSRS, CSRF); Royalties (Biomet, Stryker, Alphatec, Synthes, Amedica, Osprey, Aesculap, Seaspine); Stock ownership (Fziomed, Promethean Spine, Paradigm Spine, Benevenue, NexGen, Pioneer, Amedica, Vertiflex, Electrocore, Surgitech, Axiomed, VD Innovations, CoreSpine, Expanding Orthopaedics, Syndicom, Osprey, Bone Biologics, Curative Biosciences, PearlDiver, Pioneer)
Acknowledgments
Analytic support for this work was provided by Spectrum Research, Inc. with funding from the AOSpine Foundation.