
Abstract
Study Design
Retrospective review.
Objective
To compare clinical outcomes after transforaminal lumbar interbody fusion (TLIF) in patients with and patients without osteoporosis.
Methods
We reviewed all patients with 6-month postoperative radiographs and computed tomography (CT) scans for evaluation of the interbody cage. CT Hounsfield unit (HU) measurements of the instrumented vertebral body were used to determine whether patients had osteoporosis. Radiographs and CT scans were evaluated for evidence of implant subsidence, migration, interbody fusion, iatrogenic fracture, or loosening of posterior pedicle screw fixation. Medical records were reviewed for persistence of symptoms or recurrence of symptoms.
Results
The final data analysis included 18 (20.5%) patients with osteoporosis and 70 (79.5%) patients without osteoporosis. Males comprised 50% of patients with osteoporosis, and 64.3% of patients without osteoporosis. The mean age was significantly higher in the osteoporotic group (65.2 years) versus the nonosteoporotic group (56.9 years; p < 0.0001). We found significantly higher rates of subsidence (72.2 versus 45.7%, p = 0.05) and iatrogenic fractures (16.7% versus 1.4%, p = 0.03) in the osteoporotic group. In addition, the osteoporotic group had significantly higher radiographic complication rates compared with the nonosteoporotic group (77.8 versus 48.6%, p = 0.03). There was no difference between groups for revision surgery (16.6 versus 14.3%, p = 0.78) or postoperative symptoms (44.4% versus 50.0%, p = 0.69).
Conclusions
Our data demonstrated significantly increased rates of cage subsidence, iatrogenic fracture, and overall radiographic complications in patients with osteoporosis. However, these radiographic complications did not predispose patients with osteoporosis to an increased risk of surgical revision or worse clinical outcomes.
Keywords
Introduction
Osteoporosis is a disease characterized by the structural deterioration of bone and low bone mass. The World Health Organization defines osteoporosis as a bone mineral density (BMD) value of 2.5 standard deviations or more below the young adult mean. 1 An estimated 10 million patients in the United States have osteoporosis, and its prevalence is expected to continue to rise in the world population. 2 Degenerative spondylolisthesis and spinal stenosis, as well as vertebral compression fractures, have been reported at an increased rate in patients with osteoporosis, 3 and the disease requires special consideration for any older patient undergoing spine surgery. Obtaining optimal fixation in the osteoporotic spine is technically challenging; osteoporosis may also be associated with a poor fusion rate, with rates as low as 56% in elderly patients. 4 However, for appropriately selected patients, the presence of osteoporosis is not a contraindication to surgical intervention.
Very little available literature exists specifically evaluating the clinical and radiographic outcomes in patients with osteoporosis undergoing transforaminal lumbar interbody fusion (TLIF). In fact, to our knowledge, no previous study has examined the effect that osteoporosis may have on rates of interbody cage subsidence, migration, pedicle screw loosening, or iatrogenic fractures in patients undergoing instrumented TLIF. Therefore, we sought to compare the radiographic and clinical outcomes of TLIF in patients with and patients without osteoporosis.
Methods
After institutional review board approval, we retrospectively reviewed all patients aged 50 years or older undergoing instrumented TLIF for any indication at one of three institutions between July 2004 and June 2014. All patients received pedicle screw instrumentation with polyetheretherketone cage placement. Only patients with immediate postoperative and follow-up radiographs and computed tomography (CT) scans available for evaluation of the interbody cage were included in the study. We excluded all patients without at least a 6-month follow-up CT scan. Utilizing a technique similar to that described by Lee et al, 5 we measured CT Hounsfield units (HUs) on the lumbar vertebrae for all included patients using preoperative CT scans. Patients were then stratified as either osteoporotic or nonosteoporotic based on average lumbar vertebral body HU values. The HU cutoff values were previously determined from a separate study at our institution and found to correlate with BMD obtained from dual-energy X-ray absorptiometry (DEXA) scans (P.M. Formby et al, personal communication). Patients with HU ≤ 112.4 were considered osteoporotic, and those with HU > 112.4 were considered nonosteoporotic. Plain radiographs and CT scans were evaluated for evidence of implant subsidence, migration, interbody fusion, iatrogenic fracture, or loosening of posterior pedicle screw fixation. Patient medical records were then reviewed for postoperative symptoms, which were further subdivided into persistence of symptoms or recurrence of symptoms. We used the Student t test to evaluate continuous variables and Mid-P exact tests for dichotomous data, and p values ≤0.05 were considered statistically significant.
Results
We identified 128 patients upon initial review. Twenty-five (19.5%) of these patients were designated as osteoporotic based on the postoperative CT HU measurements versus 103 (80.4%) patients without osteoporosis. We excluded 40 patients who did not have at least a 6-month follow-up CT imaging, leaving 18 (20.5%) patients with osteoporosis and 70 (79.5%) patients without osteoporosis. These patients had a mean radiographic follow-up of 35.8 ± 27.9 months. The mean age was significantly higher in the osteoporotic group (65.2 years) versus the nonosteoporotic group (56.9 years, p < 0.0001). Males comprised 50 and 64.3% of the osteoporotic and nonosteoporotic patient groups, respectively, with a combined mean age of 58.5 ± 7.9 years. We found no significant differences between the osteoporotic and nonosteoporotic groups with regard to sex (p = 0.28), body mass index (27.6 versus 29.9, p = 0.12), number of identified medical comorbidities (2.3 versus 1.8, p = 0.15), total number of vertebral levels fused (1.9 versus 1.8, p = 0.56), or fusion rate (83.3 versus 88.6%, p = 0.56).
There were no statistically significant differences between groups for gross implant migration in the coronal or sagittal planes (11.1 versus 1.4%, p = 0.11), pedicle screw loosening (22.2 versus 8.6%, p = 0.14), revision surgery (16.6 versus 14.3%, p = 0.78), or postoperative symptoms (44.4 versus 50.0%, p = 0.69; Tables 1, 2). There were no statistically significant differences between the osteoporotic and nonosteoporotic groups in persistent or recurrent symptoms, though the rate of recurrence in the nonosteoporotic group was three times higher (persistent symptoms: 38.9 versus 30.0%, p = 0.47, respectively; recurrent symptoms: 5.6 versus 18.6%, p = 0.18, respectively).
Patient demographic and osteoporosis evaluation information
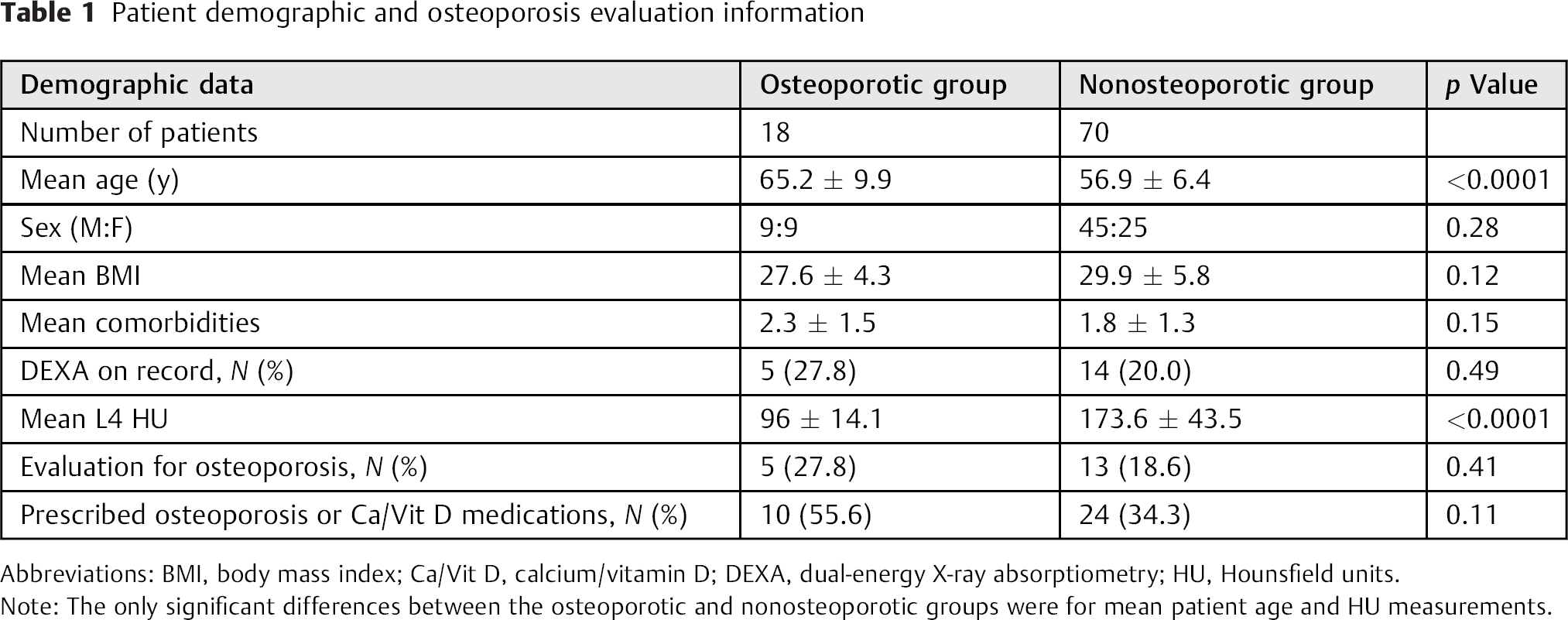
Abbreviations: BMI, body mass index; Ca/Vit D, calcium/vitamin D; DEXA, dual-energy X-ray absorptiometry; HU, Hounsfield units.
Note: The only significant differences between the osteoporotic and nonosteoporotic groups were for mean patient age and HU measurements.
Summary of perioperative data
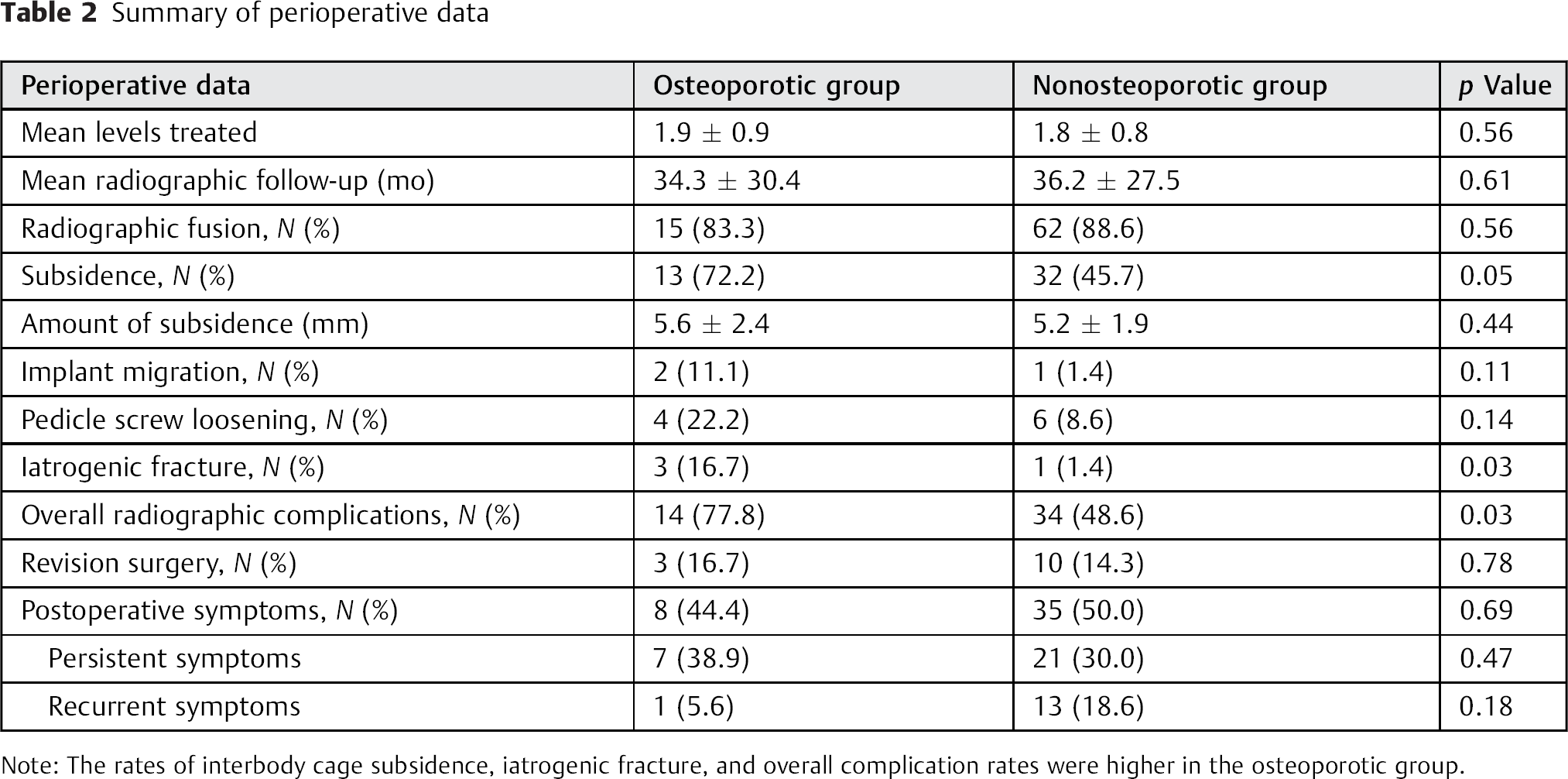
Note: The rates of interbody cage subsidence, iatrogenic fracture, and overall complication rates were higher in the osteoporotic group.
Significantly higher rates of subsidence (5.6 ± 2.4 [72.2%] versus 5.2 ± 1.9 [45.7%], p = 0.05) and iatrogenic fractures (16.7 versus 1.4%, p = 0.03) were found in the osteoporotic group. Overall, the osteoporotic population had significantly higher radiographic complication rates compared with patients without osteoporosis (77.8 versus 48.6%, p = 0.03; Table 2).
Discussion
As the average life expectancy continues to increase in the United States, spine surgeons should expect to manage a greater proportion of elderly patients with degenerative spinal conditions. Concomitant with increasing age is an associated increase in the prevalence of osteopenia and osteoporosis. In a study of patients over the age of 50 years undergoing spinal surgery in South Korea, Chin et al found osteopenia and osteoporosis rates of 41.4 and 51.3%, respectively, based on DEXA. 3 Despite the growing population of elderly patients, however, few studies have evaluated the role that low lumbar BMD may have in the complication rates and overall outcomes of patients undergoing lumbar interbody fusion.
We found that a minority of patients (21.5%) undergoing TLIF had any DEXA information available at the time of surgery, despite advancing age and clinical risk factors for osteoporosis. Utilizing HU measurements to assess lumbar vertebral body BMD, we found that of the patients with HU values consistent with osteoporosis, only 27.8% had any workup for osteoporosis prior to or following their TLIF. This finding is concerning, particularly because we found a higher overall radiographic complication rate in patients with osteoporosis undergoing TLIF, and it suggests that patients are undergoing spinal fusion surgery without being appropriately evaluated for low BMD. Although there were few patients with osteoporosis in this study, we found an increased incidence and amount of cage subsidence (Fig. 1), a higher rate of iatrogenic fractures, and more overall radiographic complications in patients with osteoporosis. Though our data did not reach statistical significance, we also found a greater propensity for implant migration and posterior pedicle screw loosening.
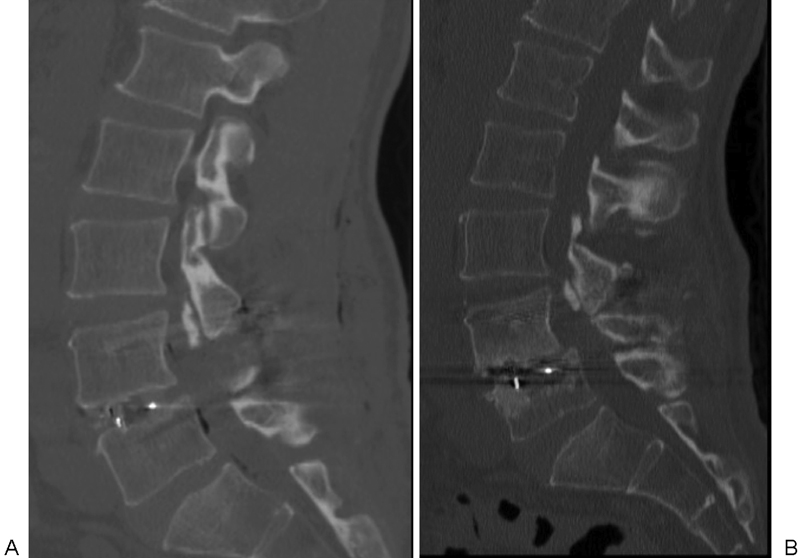
(A) Immediate postoperative and (B) 2-year follow-up sagittal computed tomography (CT) scans of a 53-year-old man who underwent L4–L5 transforaminal lumbar interbody fusion. The patient had Hounsfield unit (HU) measurements on immediate postoperative CT scan consistent with osteoporosis (average L4 HU = 105.7). Interbody cage subsidence into the superior end plate of L5 with interspace collapse is evident (9.9 mm), with evidence of increased fusion mass in the anterior column. However, at 26-month clinical follow-up, he had no recurrence of symptoms.
However, it is important to note that the increased overall radiographic complication rate did not necessarily portend worse clinical outcomes for patients with osteoporosis. Patients with osteoporosis and patients without osteoporosis underwent similar rates of revision surgery (16.7 versus 14.3%, respectively), and patients without osteoporosis actually had a higher prevalence of postoperative symptoms following TLIF, particularly when stratifying the constellation of symptoms based on persistence versus subsequent recurrence of symptoms: we found that the rate of recurrent symptoms was higher in the nonosteoporotic group (18.6 versus 5.6%, respectively), although this finding also did not reach statistical significance. It is unclear, however, why this trend was observed, and it may be related to the fact that we only included patients with six-month or later postoperative CT scans in our study, which may have biased our clinical data with an increased proportion of patients with postoperative symptoms. Despite a higher interbody cage subsidence rate in the osteoporotic group, which in turn would theoretically lead to loss of foraminal height and eventual recurrence of radiculopathy, there did not appear to be any association between osteoporosis and recurrence of symptoms.
We are unaware of any other studies specifically evaluating postoperative radiographic complications in patients with osteoporosis undergoing TLIF. Previous studies have drawn conflicting conclusions regarding whether elderly patients are at increased risk for postoperative complications following lumbar fusion. Carreon et al found a 79.6% rate of postoperative complications in patients ≥65 years old at the time of posterior lumbar instrumented fusion. 6 However, Cassinelli et al found a much lower rate of major complications (3%) and minor complications (∼31%) in a similar cohort of patients ≥65 years undergoing instrumented and noninstrumented lumbar spine arthrodesis. 7 Similarly, Cavagna et al evaluated patients > 65 years undergoing instrumented lumbar fusions and found good clinical outcomes and no serious postoperative complications or reoperations in this cohort. 8 However, they did find a 10.3% rate of implant failure (two screws and two rods failed) at 2-year or later follow-up. Glassman et al investigated clinical outcomes of patients ≥65 years old compared with those < 65 years old undergoing single-level instrumented posterolateral lumbar arthrodesis; the authors found that the older population had similar clinical and health-related quality-of-life improvements when compared with the younger cohort. 9 However, the older cohort experienced significantly increased rates of serious (38 versus 17%) and overall adverse postoperative events (56 versus 36%), although there was no increased risk of revision or reoperation between these groups. Likewise, Okuda et al did not find major differences in clinical outcomes between patients ≥70 years old and those < 70 years old undergoing instrumented lumbar interbody fusion. 10 These authors found no increased risk or instrument failure between groups, although they did find lower rates of fusion and higher rates of collapsed union and delayed union in the elderly group. 10
Inherent to any small retrospective study, the possibility of type II statistical error limits the generalizability of our analysis. The proportion of patients with osteoporosis in our study was low, which could be a source of bias. Our study was also limited by the quality of the medical records, as well as available radiographs and CT scans. In addition, despite a minimum age of 50 years for inclusion in this study, our patients were still relatively young and healthy, with few comorbidities and a mean age of only 58.5 years. We looked at a heterogeneous group of patients with disparate preoperative diagnoses undergoing TLIF for any reason, which could contribute to bias in this study. We used HU to classify patients into either osteoporotic of nonosteoporotic categories. The use of HU for measurement of bone density has not been validated in the literature, with few reports of its use to date. Further studies are needed to determine if this method is widely reproducible. Future studies may consider evaluating older patients with greater BMD loss. Further prospective studies are needed to evaluate the role that osteoporosis plays in complication rates and overall clinical outcomes in patients undergoing lumbar fusion surgery.
Conclusion
In conclusion, we found significantly increased rates of cage subsidence, iatrogenic fractures, and overall radiographic complications in patients with osteoporosis undergoing TLIF. However, these radiographic complications did not predispose patients with osteoporosis to worse clinical outcomes, and larger, prospective studies are needed to further evaluate lumbar fusion surgery in patients with osteoporosis.
Disclosures
Peter M. Formby: none
Daniel G. Kang: none
Melvin D. Helgeson: none
Scott C. Wagner: none
Footnotes
Note
This study was performed at the Walter Reed National Military Medical Center, Bethesda, MD. The views expressed in this manuscript are those of the authors and do not reflect the official policy of the Department of Army, Department of Defense, or U.S. Government. All authors are employees of the United States government. This work was prepared as part of their official duties and as such, there is no copyright to be transferred. The authors have no potential conflicts of interest to report. No funding was received from any sources. No previous publications of this work. No reproduced copyrighted materials. Institutional review board approval with publication clearance was obtained for this study.