
Abstract
Study Design
Case series and review of the literature.
Objective
To review the management of giant calcified disks in our large cohort and compare with the existing literature. We discuss our surgical technique.
Methods
Twenty-nine cases of herniated thoracic disk between 2000 and 2013 were reviewed. Eighteen patients were identified as having giant calcified thoracic disks, defined as diffusely calcified disks occupying at least 40% of the spinal canal. Demographic data was collected in addition to presentation, imaging findings, operative details, and outcomes using the modified Japanese Orthopaedic Association (mJOA) scale.
Results
Giant calcified thoracic disks (GCTDs) are unique clinical entities that require special neurosurgical consideration owing to significant (≥40%) involvement of the spinal canal and compression of the spinal cord, often leading to myelopathy. The median age at diagnosis was 51.2 years (range 37 to 70) with the mean duration of presenting symptoms being 9.9 months (range 2 weeks to 3 years). Seventeen (94.4%) patients presented with at least one sign of myelopathy (hyperreflexia, hypertonia, bladder or bowel dysfunction) with the remaining 1 (5.6%) patient presenting with symptoms in keeping with radiculopathy. Thoracotomy was performed on 17 (94.4%) patients, and 1 (5.6%) patient had a costotransverse approach. Mean follow-up was 19.8 months (range 7 months to 2 years). mJOA score improved in 15 (83.3%) patients. mJOA scores in the other patients remained stable.
Conclusions
GCTDs are difficult neurosurgical challenges owing to their size, degree of spinal cord compression, and consistency. We recommend a trench vertebrectomy via a thoracotomy in their surgical management. This procedure safely allows the identification of normal dura on either side of the compressed segment prior to performing a diskectomy. Excellent fusion rates were achieved with insertion of rib head autograft in the trench.
Introduction
Thoracic disk herniation is a rare surgical entity that is estimated to account for ∼0.25 to 1.8% of all spinal herniated disks, 1 , 2 , 3 , 4 with an estimated incidence of 1 per million patient-years. 2 They usually present between the third and sixth decades with a female predilection. 5 Hott et al described giant calcified thoracic disks (GCTDs) as a specific subgroup of herniated thoracic disks with a distinct clinical presentation, work-up, and management. 6 GCTDs were defined as “occupying more than 40% of the spinal canal based on preoperative computed tomography (CT), myelography, magnetic resonance imaging (MRI) or both.” 6 GCTDs offer a neurosurgical challenge owing to their size, consistency, and degree of spinal cord compression. Careful consideration of the surgical approach is necessary to ensure the best outcomes. Some diversity in the surgical management of GCTDs still exists among neurosurgeons. Here, we present 18 cases of GCTDs, which represents the second largest cohort in the literature, and we describe the trench vertebrectomy via a thoracotomy as a safe and effective surgical technique.
Materials and Methods
Twenty-nine patients who underwent surgical treatment in our unit for herniated thoracic disks between the years 2000 and 2013 were reviewed. Following radiologic review, 18 patients were found to have GCTDs as defined by Hott et al. 6 Retrospective data was collected on patient demographics, presentation, operative details, and imaging findings including the fusion rates. The modified Japanese Orthopaedic Association (mJOA) score was used to assess the outcomes.
Results
Clinicopathologic Characteristics
There was a female preponderance in our series with a male-to-female ratio of 4:14. The median age at diagnosis was 51.2 years with a range of 37 to 70 years. The mean duration of presenting symptom(s) was 9.9 months, with a range of 2 weeks to 3 years. Seventeen (94.4%) patients in this series presented with signs and/or symptoms of myelopathy, with the remaining 1 (5.6%) patient presenting with symptoms more in keeping with a radiculopathy. The commonest presenting symptom was lower limb weakness in 66.7% of the series, and the commonest clinical sign was hyperreflexia in 83.3% (Table 1).
Clinicopathologic presentation
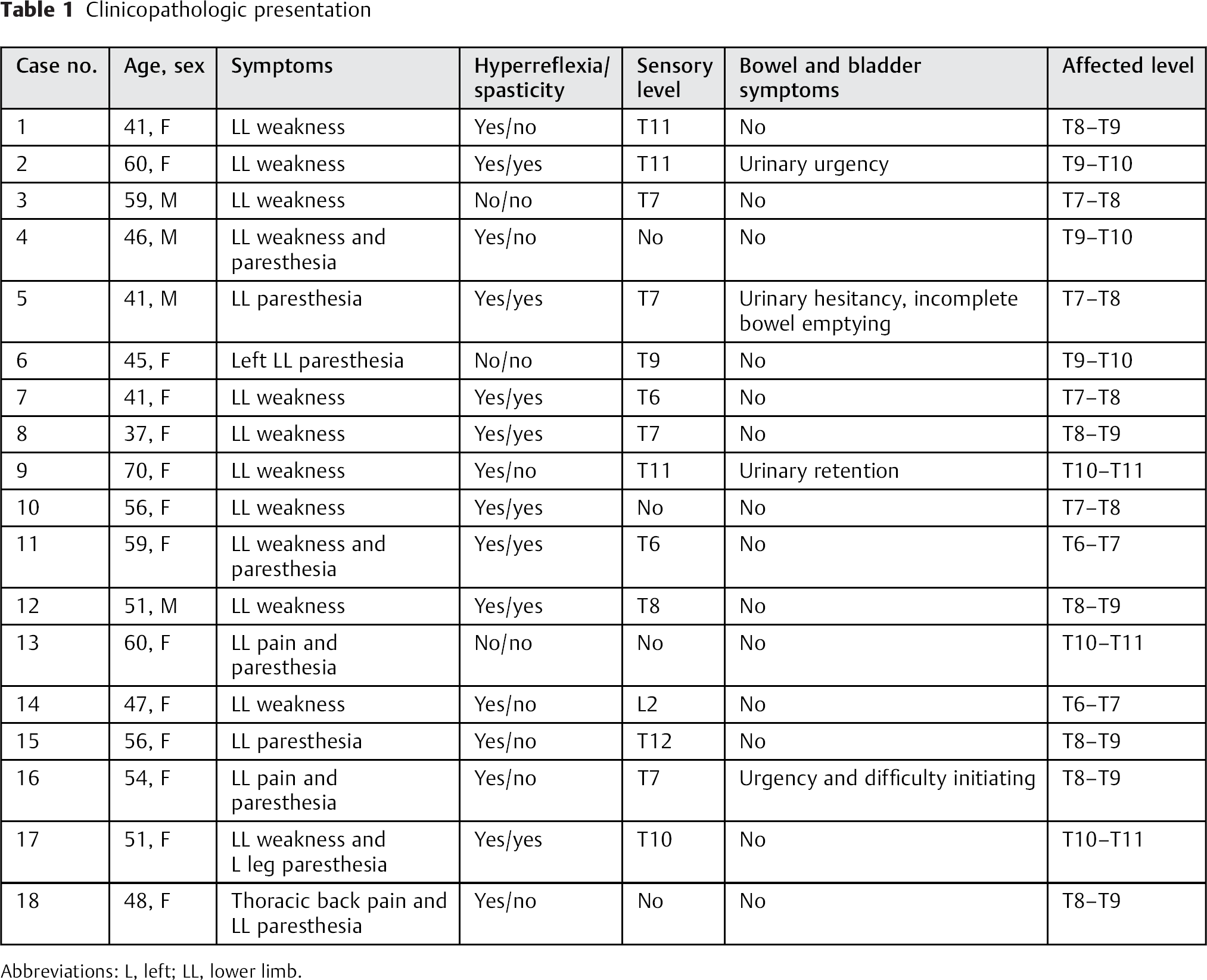
Abbreviations: L, left; LL, lower limb.
Diagnostic Workup
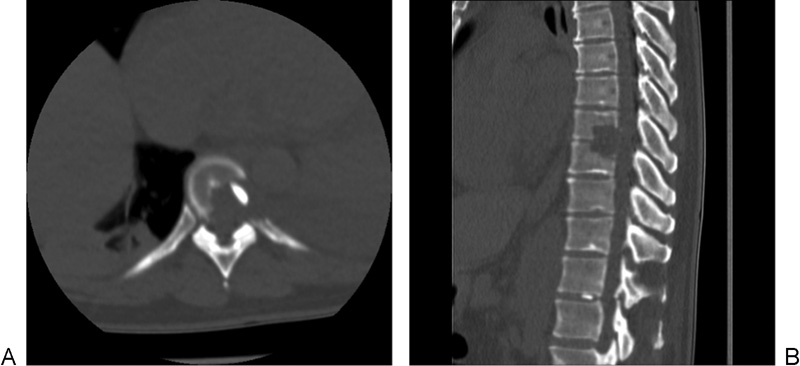
All patients in our center had both a preoperative computed tomography (CT) scan and MRI (Figs. 1 and 2). A CT scan defines the degree of calcification, disk morphology, and aids in preoperative planning (Fig. 1). The commonest affected level in our cohort was at T8–T9 in 6 patients (33.3%), followed by T7–T8 in 22.2% (Table 1).
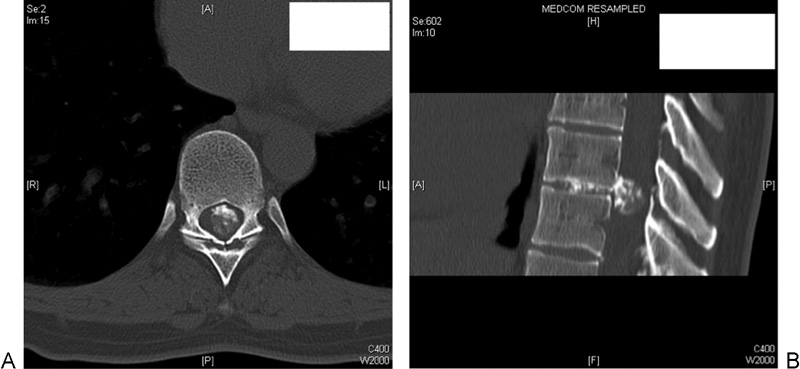
(A) Preoperative axial computed tomography (CT) showing the giant calcified thoracic disk (GCTD) within the spinal canal. (B) Preoperative sagittal CT showing the same GCTD.
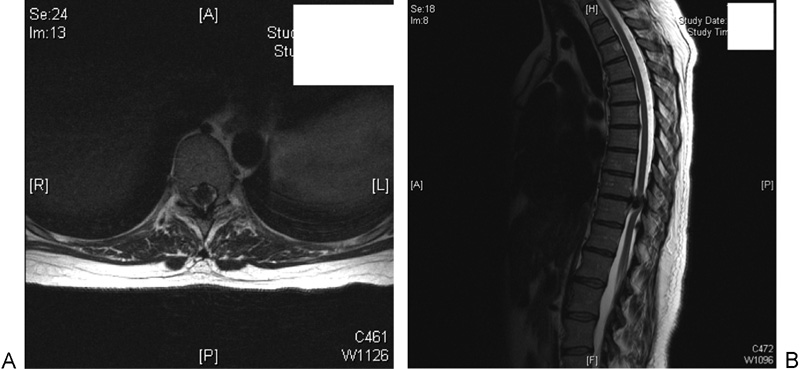
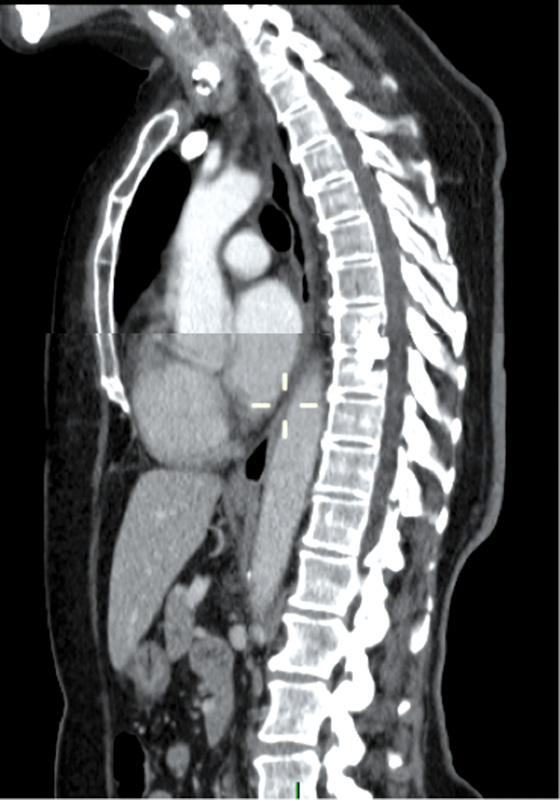
(A) Preoperative axial magnetic resonance imaging (MRI) of the same disk space as Fig. 1. (B) Preoperative sagittal MRI showing severe involvement of the spinal cord.
Surgical Technique
The disk was excised via a trench vertebrectomy in all patients. The access was through a thoracotomy in all but one patient, in whom a costotransverse approach was used. The ultrasonic bone cutter was used to facilitate the vertebrectomy in the last three patients in our series.
The patient was positioned in the lateral position with the side of the thoracotomy uppermost. For localization of the affected level, we used a combination of intraoperative X-ray and rib counting. The thoracotomy was usually from the left side, because the chest cavity is larger on this side and it is also easier to mobilize the aorta than the great veins. In the upper thoracic levels (above T5), a right-sided thoracotomy may be used to avoid the arch of the aorta.
To gain access to the affected level, the rib two levels above the disk is excised at the midportion. The lung was collapsed at this stage and the pleura opened. Once the affected level was identified and confirmed with an X-ray, the parietal pleura was opened over the vertebral bodies below and above and reflected away from the spine. To allow better visualization of the lateral disk, the rib head was resected, revealing the pedicle and neural foramen. The costovertebral and costotransverse ligaments were divided, and up to ∼2 cm of rib head were removed with bone nibblers or a drill if necessary. A trench vertebrectomy was performed with half of vertebra on either side excised; it was not necessary to extend this procedure to remove the anterior part of the vertebral body (Figs. 3 and 4). The ultrasonic bone cutter was useful here as an alternative to piecemeal resection or using a pneumatic drill. The bone cutter can be used to demark the partial vertebrectomy. The groove was deepened until enough bone was removed to access the disk and normal dura on either side (Fig. 3).
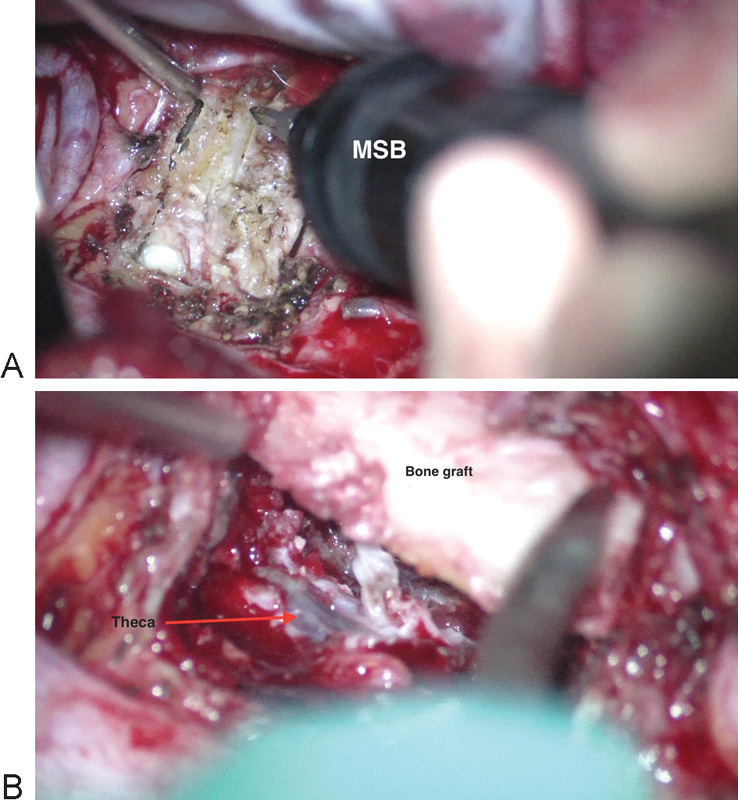
(A) Intraoperative image using the Misonix bone cutter (MSB; Misonix, Farmingdale, New York, United States) to drill the giant calcified thoracic disk. (B) Intraoperative image of the bone graft being placed. The theca is also visible.
(A) Postoperative axial computed tomography (CT) outlining decompression using the trench technique. (B) Postoperative sagittal CT clearly delineating the trench vertebrectomy.
At this stage, the dura proximal and distal to the calcified disk was identified. The calcified disk was removed piecemeal. The base of the disk was eased away from the posterior longitudinal ligament, a layer of which may be left if adherent to the dura. After complete excision, the dura will move forward. In 8/18 cases (44.4%), the disk material was noted to be adherent to the cord. In such instances, a remnant layer of disk was often left attached to the cord. For the bony defect, we fashioned a graft from the excised portion of rib (Fig. 2). An example of the histologic appearance from the excised material is shown in Fig. 6A, B. It shows fragments of calcified material within the degenerate disk associated with peripheral ossification.
Outcomes
Fifteen (83.3%) patients experienced a postoperative improvement of at least 1 point in the mJOA score on last follow-up. The remaining three patients’ mJOA scores remained unchanged (Table 2). Postoperative complications included cerebrospinal fluid leak in 2 patients (11.1%). This complication was identified and repaired intraoperatively with no further sequelae. Six (33.3%) patients required a blood transfusion during their hospital stay, which ranged from 2 to 5 U. One (5.6%) patient was transferred to the intensive care unit for ventilatory support due to development of adult respiratory distress syndrome. The average length of stay was 10.7 days, with a range of 4 to 35 days. There was no surgical mortality.
Pre- and postoperative mJOA scores
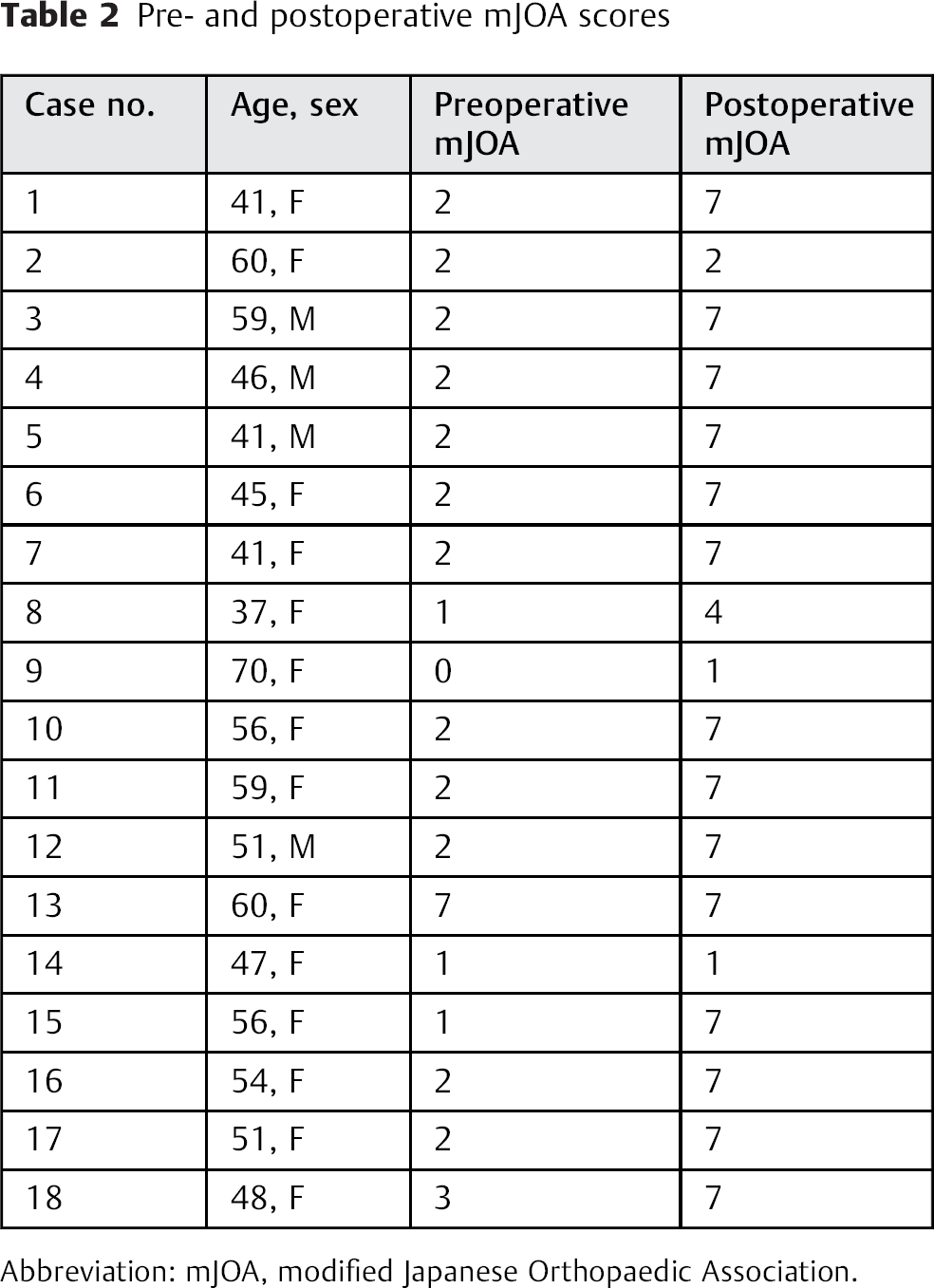
Abbreviation: mJOA, modified Japanese Orthopaedic Association.
Follow-Up
The mean duration of follow-up was 19.8 months (range 7 months to 2 years). Postoperative imaging was performed on all patients but was heterogeneous in modality including plain films, CT scans, or MRIs at 6 to 12 months. Fusion was reported in all patients on the follow-up radiology reports; the criteria used were the documentation of bony trabeculation and absence of bony lucency at the graft/vertebral end plate interface (Fig. 5). The postoperative imaging was not standardized compared with the preoperative imaging, and formal sagittal alignment measures were not calculated; however, no patient developed a clinically or radiologically evident kyphotic deformity.
Delayed postoperative sagittal computed tomography showing fusion at T8–T9.
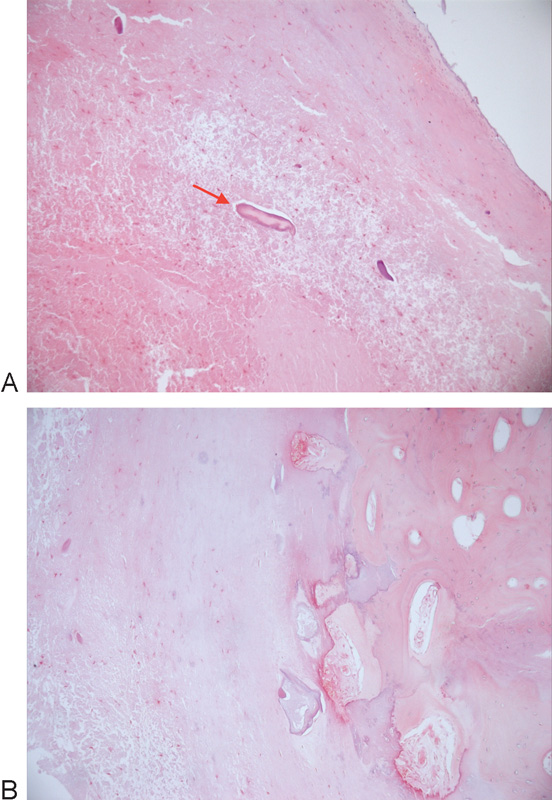
(A, B) Histologic appearance of the excised disk. Hematoxylin and eosin, ×10. (A) Fragments of calcified material (red arrow) within degenerate fibrocartilage. (B) Peripheral calcification. All the bluish areas in right side of the slide represent calcium; this tissue has been decalcified to be able to cut it, hence the rest of the right side is pink.
Discussion
GCTDs are rare and present a technical neurosurgical challenge. Because of their size and degree of calcification, a significant proportion of GCTDs display some degree of thecal involvement, with penetration into the subarachnoid space via tears of the posterior longitudinal ligament and the dura mater. 7 , 8 Presentation may be with clinical signs and symptoms of a compressive myelopathy, radiculopathy, and/or back pain. 1 , 6 , 8 , 9 , 10
In our series, the median age and female preponderance is a finding echoed in other studies, 11 , 12 , 13 , 14 which is speculated to be secondary to altered calcium-phosphate metabolism that occurs postmenopausally. 8 The pathophysiology of the calcification process is also poorly understood, although it has been suggested that calcium deposition originates from the posterior longitudinal ligament with extension into the disk space.15 All of the lesions in our cohort occurred at the lower thoracic levels, which is consistent with the findings by other authors. 1 , 6 , 8 , 10 It is estimated that 75% of herniated thoracic disks occur below the level of T8, which is a probable combined consequence of the greater weight load in the lower thoracic spine and its greater range of movement. 6 , 12 , 14 , 16
Myelopathy was present in 17 (94.4%) of our patients. The other large case series in the literature describing GCTDs reported similar high rates of myelopathy, 1 , 6 , 8 , 10 with Hott et al comparing these high rates to ∼47% in smaller, nongiant THDs. 6
Various surgical techniques and approaches to manage GCTDs are advocated in the literature. The choice of surgical approach has evolved over the last century and has included laminectomy, transpedicular, costotransversectomy, and transthoracic methods. Posterior approaches are more or less obsolete owing to extremely poor results, particularly from laminectomy. 7 , 17 , 18 , 19 , 20 Despite the refinement of several approaches, the optimal operative treatment for thoracic disk herniations remains open to debate and may in part be dictated by the skills of the operating surgeons, whether the disk is central, and the presence of calcification. 4 , 14 , 17 , 21 In their review, Mulier and Debois compared 7 of their own patients between 1986 and 1993 with 384 others to compare transthoracic, lateral, or posterolateral approaches to THDs; their results illustrated that transthoracic surgeries were associated with better neurologic outcomes. 21
Most authors advocate an open thoracotomy approach, in particular for centrally located calcified disk herniations. 1 , 4 , 6 , 21 , 22 Technical variations in the anterior transthoracic approach exist, with Moran et al recommending a mini-open retropleural transthoracic approach with comparable results, 10 although some authors advocate a two-level vertebrectomy followed by instrumented fusion. 6 , 22 Barbanera et al suggest using a mini-vertebrectomy, although instrumentation was still required in 2 (28.5%) cases of their series. 1
In our view, a trench vertebrectomy has the advantage of visualizing the dura on either side of the herniated disk, allowing a safe excision, especially in the cases of a broad, central, heavily calcified disk prolapse with severe cord compression. In addition, this technique enables minimal bone removal compared with a complete two-level vertebrectomy. A costotransverse approach may be an alternative and can be utilized if the anatomy of the prolapsed disk is suitable (e.g., a more lateral cord compression) and good visualization of the anterolateral dura above and below the compressed segment can be safely attained.
The transthoracic approach to the thoracic spine has several advantages. It enables direct visualization of the ventral spinal column, which is essential in anterior spinal pathologies such as GCTDs. The approach enables the greatest access and avoids manipulation of the spinal cord, which is already compromised in GCTDs. 23 , 24 A left-sided thoracotomy evades the vena cava and liver on the right, though a right-sided approach may be undertaken if the pathology is predominately on that side or to evade poor visualization from structures such as the aortic arch around the level of T3 and T4. 24 Disadvantages of this approach are that it may require a longer hospitalization and longer intensive care stay than with other procedures, with a greater risk of pulmonary complications; also, postoperative pain may be greater. 4 , 17 , 21
Thoracic excision of GCTDs is known to be associated with possible significant blood loss, 10 particularly where vertebrectomy is conducted, 25 which can mandate the ligation of two radicular arteries above and below the disk space. The use of the bone cutter in our experience allows all radicular arteries to be preserved, even those at the disk space level, thereby reducing the risk of spinal cord stroke secondary to ligation of the radicular artery of Adamkiewicz. Spinal cord injury and dural tears are also less likely due to the selective tissue-cutting properties of the ultrasonic bone cutter. Bone is cut in preference to soft tissue, which responds elastically in contact with the blade and therefore moves and vibrates, causing dissemination of the energy. 26 , 27 , 28
The complications associated with anterior approaches to the spine vary depending upon the specific approach, surgical indication, and patient factors. A large meta-analysis by McDonnell et al reviewed 447 patients undergoing anterior surgery to the thoracic, thoracolumbar, or lumbar spine. 25 Indications included correction of deformity, tumor, vertebral osteomyelitis, or diskitis. The authors’ aim was to determine the perioperative complications, which were divided by the authors into major and minor as per Table 3. Major complications were reported in 11% and minor complications in 24%. Others have also used this system to report their complication rates. 22 In a large meta-analysis of thoracic spine surgery, Fessler and Sturgill reported a complication rate of 11% in transthoracic approaches. 17 Ayhan et al reported a complication rate of 21.4%, with two of these complications arising secondary to instrumentation. 22
McDonnell complication definitions 25
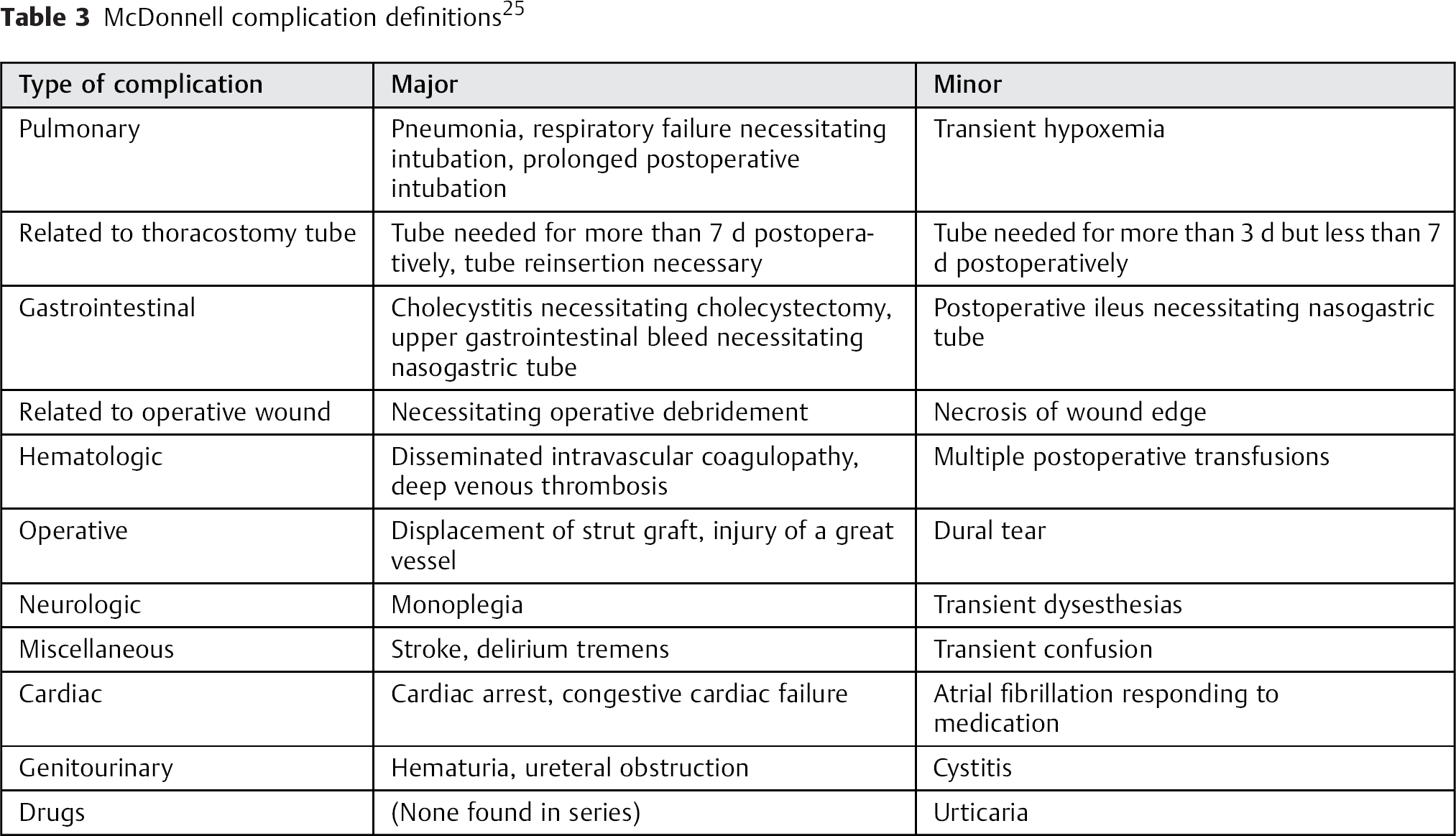
In utilizing the criteria for perioperative complications from McDonnell et al, 25 we report a major complication rate of 5.6% with one of our patients being intubated and ventilated for adult respiratory distress syndrome. Minor complications occurred in 2 (11.1%) patients; both had an intraoperative cerebrospinal fluid leak, which was repaired at the time with no sequelae. Intraoperative blood transfusion occurred in 6 (33.3%) patients, which is an expected complication of transthoracic surgery with vertebrectomy as previously mentioned.
In our series, 15 (83.3%) patients had a functional improvement of at least one grade on the mJOA scoring system, with the remaining patients’ mJOA scores remaining unchanged. No patient had decline in neurologic status. These results compare favorably with those from the other GCTD series. 1 , 6 , 10 , 22
None of the major series on GCTDs reported on fusion rates or development of kyphosis. 1 , 6 , 10 , 22 In our case cohort, all patients had evidence of fusion on postoperative imaging as defined by documentation of bony trabeculation and absence of bony lucency at the graft/vertebral end plate interface on radiology reports. No patient developed a clinically or radiologically evident kyphotic deformity on follow-up; we acknowledge the limitations of our cohort study in this regard as Cobb angles were not recorded and compared pre- and postoperatively. However, others have also noted that when the amount of bone removed is minimal in an anterior approach, it is not likely to produce frank spinal instability, and instrumentation is not required in these cases. 4 , 10 Better long-term data from cohort studies is required to make firm conclusion. Various instrumentation techniques are an alternative and have been reported in the literature. Some surgical series that analyzed their results following cage fixation post–thoracic vertebrectomy for a variety of indications have reported worsening of the kyphotic angle postoperatively, albeit the change was minimal. 29 , 30 , 31 , 32
Conclusions
A transthoracic approach is the gold standard surgical strategy in dealing with GCTDs. A trench vertebrectomy via a thoracotomy allows safe identification of normal dura on either side of the compressed segment prior to performing a diskectomy. A rib autograft has achieved 100% fusion rates with no kyphotic deformities reported in our series. Preservation of radicular arteries protects the spinal blood supply despite a wide trench decompression. Overall, 83% of patients showed postoperative improvement in their mJOA score with none of our cohort experiencing neurologic decline. These results are encouraging compared with early reports on this disease entity.
Disclosures
Rafid Al-Mahfoudh: none
Paul S. Mitchell: none
Martin Wilby: Grant (NIHR)
Daniel Crooks: none
Chris Barrett: none
Robin Pillay: none
Tim Pigott: none