
Abstract
Study Design:
Multicenter retrospective case series.
Objective:
To determine the rate of thoracic duct injury during cervical spine operations.
Methods:
A retrospective case series study was conducted among 21 high-volume surgical centers to identify instances of thoracic duct injury during anterior cervical spine surgery. Staff at each center abstracted data for each identified case into case report forms. All case report forms were collected by the AOSpine North America Clinical Research Network Methodological Core for data processing, cleaning, and analysis.
Results:
Of a total of 9591 patients reviewed that underwent cervical spine surgery, 2 (0.02%) incurred iatrogenic injury to the thoracic duct. Both patients underwent a left-sided anterior cervical discectomy and fusion. The interruption of the thoracic duct was addressed intraoperatively in one patient with no residual postoperative effects. The second individual developed a chylous fluid collection approximately 2 months after the operation that required drainage via needle aspiration.
Conclusions:
Damage to the thoracic duct during cervical spine surgery is a relatively rare occurrence. Rapid identification of the disruption of this lymphatic vessel is critical to minimize deleterious effects of this complication.
Introduction
The thoracic duct is the body’s largest lymphatic vessel; its proximity to the vertebral bodies makes it an important anatomical consideration during low anterior spine surgery. Variability in the anatomic course of the vessel, as well as its small size, can result in potential injury. 1 Damage to the thoracic duct during spinal operations is a rare but potentially serious complication that manifests as a cervical chylous fistula, chylothorax, or chyloretroperitoneum. 2 Serious insult to the structure can result in significant nutritional deficiency, respiratory dysfunction, and considerable immunosuppression. 3,4 Conservative therapy initially consists of diet modification, electrolyte monitoring, and appropriate drain placement. 5 If needed, definitive treatment requires ligation of the thoracic duct, a procedure that can result in significant morbidity. 6
Current data regarding the occurrence of thoracic duct injury during spine surgery is primarily found as isolated case reports. 7 -14 This study is the first to report the overall incidence of thoracic duct injury during cervical spine surgery based on a multicenter retrospective review.
Methods
We have conducted a retrospective multicenter case series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network, selected for their excellence in spine care and clinical research infrastructure and experience. Medical records for 17 625 patients who received cervical spine surgery (levels from C2 to C7) between January 1, 2005, and December 31, 2011, inclusive, were reviewed to identify occurrence of 21 predefined treatment complications. The complications included reintubation for the purpose of a hematoma evacuation, esophageal perforation, epidural hematoma, C5 palsy, recurrent laryngeal nerve palsy, superior laryngeal nerve palsy, hypoglossal or glossopharyngeal nerve palsy, dural tear, brachial plexopathy, blindness, graft extrusion, misplaced screws requiring reoperation, anterior cervical infection, carotid artery injury or cerebrovascular accident, vertebral artery injuries, Horner’s syndrome, thoracic duct injury, quadriplegia, intraoperative death, revision of arthroplasty, and pseudomeningocele. Trained research staff at each site abstracted the data from medical records, surgical charts, radiology imaging, narratives, and other source documents for the patients who experienced one or more of the complications from the list. Data was transcribed into study-specific paper case report forms. Copies of case report forms were transferred to the AOSpine North America Clinical Research Network Methodological Core for processing, cleaning, and data entry. Descriptive statistics were provided for baseline patient characteristics.
Results
Of the 17 625 total patients reviewed, 9591 individuals underwent surgery of the cervical spine using an anterior approach only. These cases were reviewed to identify cases of iatrogenic thoracic duct injury. There were 2 (0.02%) instances of damage to the thoracic duct. The highest incidence for any single institution was 0.079%, while 19 of 21 institutions reported zero instances of thoracic duct injury.
Case 1
The first occurrence of thoracic duct injury was in a previously healthy male that was involved in a motor vehicle accident. As a consequence, the patient developed radicular pain for which physical therapy did not provide adequate symptom relief. Therefore, the patient opted to undergo anterior cervical discectomy and fusion (ACDF) at the level of C5-C6. The operation was conducted using a left-sided approach. Intraoperatively, a chyle leak was noted and the otolaryngology team was consulted to address the disruption of the thoracic duct. Surgical clips were utilized to control the leakage. The patient was discharged home on postoperative day 1. There was one postoperative visit 80 days following discharge. No residual effects were noted from the intraoperative leak during the follow-up period.
Case 2
This patient underwent ACDF to address a herniated nucleus pulposus with associated radiculopathy at the level of C5-C6. The patient was female, had a body mass index of 21.9, and had no comorbid conditions at the time of the index surgery. A left-sided approach was used to gain access to the cervical spine. There were no issues intraoperatively and no chyle leak was noted. The patient was discharged home following the operation in stable condition. Approximately 2 months after surgery, the patient presented for outpatient follow-up during which a 2.5 × 2.5 cm nontender, mobile mass was noted superior to the incision. There were no accompanying symptoms of fever or dysphagia; no signs of infection were noted around the incision. Ultrasound revealed a complex fluid collection sizing 2.3 cm in diameter. Needle aspiration of the lesion removed 3.5 mL of milky white fluid identified as chyle. The patient recovered uneventfully and no additional problems were noted during further follow-up. In all, the patient had 8 postoperative visits with the most recent occurring 3.5 years following the index operation.
Discussion
Anatomy of the Thoracic Duct
The thoracic duct serves as the primary conduit for the return of lymph to the bloodstream from all lymphatic vessels except those found on the right side of the head, neck, thorax, and arm (Figure 1). As such, it delivers three quarters of the lymph produced in the body to the venous circulation. 15 The length of the thoracic duct ranges from 36 to 45 cm in adults. Its origin is in the retroperitoneum at the cisterna chyli, located on the anterior surface of the first or second lumbar vertebra. After reaching the fifth thoracic vertebra, its course veers left and continues its ascent posterior to the aortic arch and the thoracic portion of the left subclavian artery. Traveling between the left side of the esophagus and pleura, it reaches the root of the neck and forms an arch rising approximately 3 to 4 cm above the clavicle. At the superior border of the clavicle, the thoracic duct is bordered by the left carotid sheath anteriorly, the omohyoid muscle laterally, the anterior scalene fascia posteriorly, and the esophagus medially. It then crosses anterior to the subclavian artery, vertebral artery and vein, and the thyrocervical trunk and terminates by opening into the junction of the left subclavian and left internal jugular veins. 16
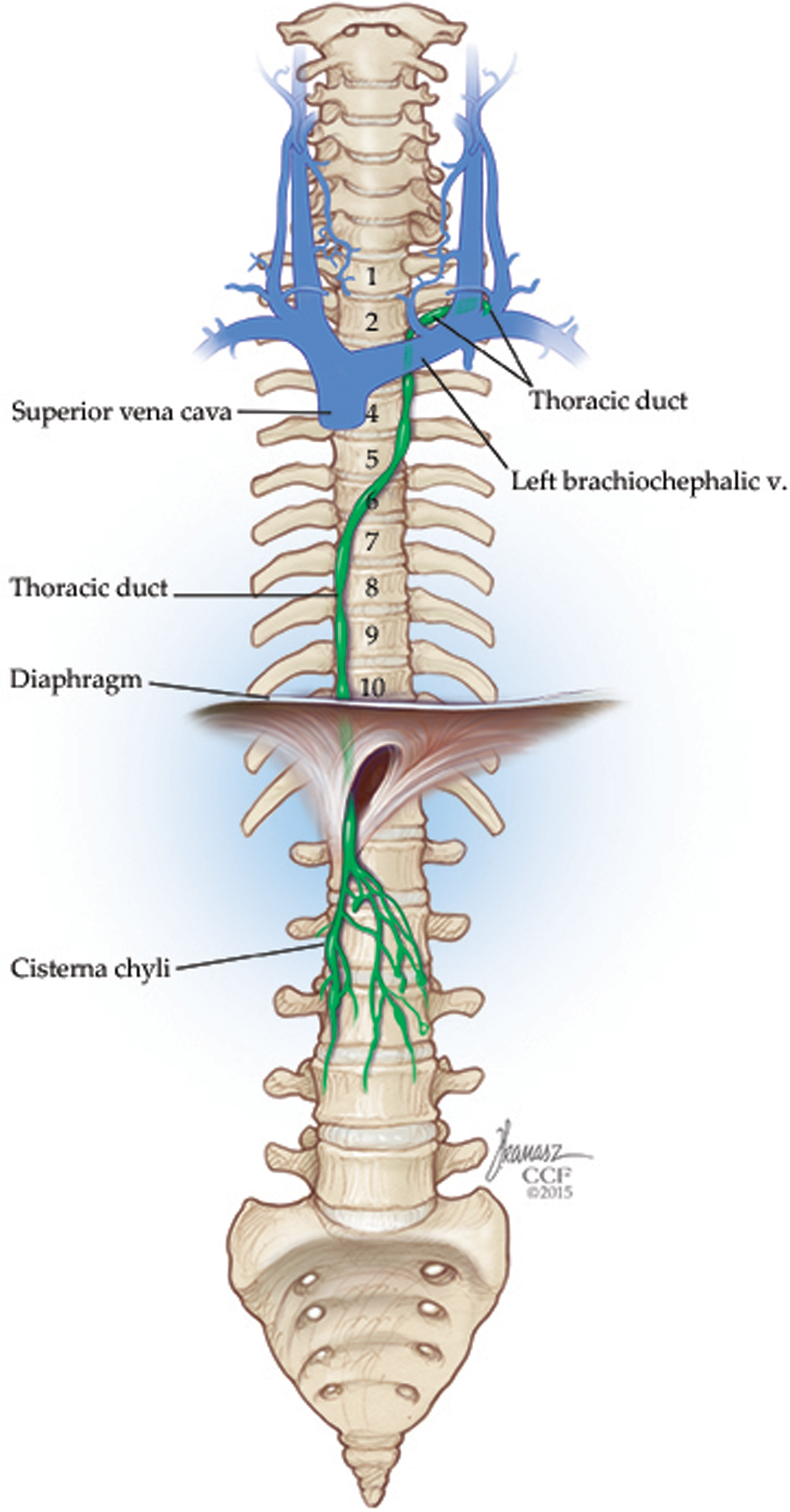
Drawing depicting the origin of the thoracic duct, its usual course of ascension through the thorax, and its termination in the root of the neck.
Important variations in the course of the thoracic duct have been reported as a result of various cadaver studies. Gottlieb and Greenfield found one cadaver out of 75 with a thoracic duct that remained on the right side during its ascent and emptied into the right internal jugular vein. 17 The height of the arch of the thoracic duct in the root of the neck also varies, as it can be inferior to, at, or superior to the clavicle. 18 Hart et al described a case in which the arch was situated 7 to 8 cm above the clavicle. 13 Importantly, there is significant deviation in the termination pattern of the thoracic duct as it joins the systemic circulation. It may end as single or multiple outlets into the left internal jugular vein, the left subclavian vein, the left external jugular vein, the left brachiocephalic vein, the left transverse cervical vein, or the right internal jugular vein. 17 -20 Greenfield and Gottlieb’s study of 75 cadavers found 89.4% of thoracic ducts to have 1 termination, 6.6% to have 2 terminations, and 4% to have 3 terminations. 17
Chyle Leak During Spinal Surgery
The majority of reported cases of thoracic duct injury during spine operations have occurred during surgery of the thoracolumbar spine. 7 -12 Colletta and Mayer describe a case report in which an intraoperative chyle leak is noted. 7 Despite attempted intraoperative repair, the patient developed a postoperative chylothorax, which was subsequently managed with a chest tube and low-fat diet until resolution was achieved. Nakai and Zielke reported 6 instances of chylothorax in an estimated 2000 cases of thoracolumbar spinal surgery; 8 all were treated conservatively with a combination of diet modification, needle aspiration, and chest tube placement. Propst-Proctor et al surveyed a total of 10 orthopedic spine surgeons who had combined to perform an estimated 1000 anterior thoracolumbar operations. 9 They reported a total of 3 cases of chylothorax that were managed conservatively with closed chest tube drainage and a restricted fat diet. Similarly, Bhat and Lowery reported 3 operations complicated by chyloretroperitoneum and/or chylothorax that resolved with a combination of diet modification, chest tube drainage, and/or continued maintenance of a retroperitoneal drain. 10 Su and Chen also described a patient that experienced retroperitoneal chyle leakage after undergoing lumbar fusion; 11 this patient had spontaneous cessation of drainage upon temporary clamping of his drain tube. Hussain et al described a series of 4 patients that developed chyloretroperitoneum following anterior lumbar surgery. 12 Three patients’ symptoms resolved with fluoroscopic-guided percutaneous aspiration as well as drainage catheterization. The fourth patient had continued drainage of her abdominal lymphocele despite placement of a catheter and required reoperation 6 weeks after the initial surgery to create a peritoneal window to allow drainage of the lymphocele into the peritoneal space.
Thoracic duct injury during cervical spine surgery is sparsely described in the literature. Two case reports describing its occurrence in this setting were identified. Hart et al described a case of a patient undergoing a left-sided ACDF in which an intraoperative chyle leak was identified secondary to disruption of the thoracic duct in the supraclavicular region. 13 In this case, the arch of the thoracic duct extended 7 to 8 cm above the clavicle, making it significantly more superior than expected. Intraoperative suture ligation of the duct was conducted and the leakage was confirmed to have stopped; there were no postoperative complications. Warren et al reported a case of cervical lymphocele formation following right-sided ACDF during which the right lymphatic duct was penetrated. 14 Surgical closure of the lymphocele attempted 2 weeks postoperatively was unsuccessful; subsequent percutaneous drainage and sclerotherapy revealed a large branch of the thoracic duct communicating with the lymphocele. This branch was embolized via a percutaneous transcervical approach, resulting in immediate resolution of the patient’s symptoms.
The rate of thoracic duct injury during anterior cervical spine surgery was 0% at the majority of institutions reviewed (19 of 21). The highest incidence at any single institution was found to be 0.079%. Estimates by Nakai and Zielke as well as Propst-Proctor et al suggest that the rate of thoracic duct injury during thoracolumbar surgery is approximately 0.3% 8,9 : Nakai and Zielke reported 6 cases of injury out of an estimated 2000 cases, and Propst-Proctor et al found 3 instances out of an estimated 1000 patients. The present study is the first to report an incidence of thoracic duct injury following cervical spine surgery, revealing a substantially lower incidence of this complication in cervical surgery versus thoracolumbar. This discrepancy is possibly due to the longer anatomic course of the thoracic duct in the thoracolumbar area as compared to the cervical spine.
Chyle Leak During Other Surgeries
The thoracic duct is subject to injury during any operation that involves the root of the neck. Such procedures are commonly conducted by thoracic surgeons and otolaryngologists in addition to spine surgeons. For instance, Marthaller et al describe a series of patients that incurred damage to the thoracic duct following esophagectomy; 21 this manifested through the formation of a chylothorax and/or a high-output chylous fistula. For such cases, the authors advocated for percutaneous embolization of the thoracic duct prior to open re-exploration. Similarly, Patel et al describe a case of thoracic duct injury following neck dissection that was treated by percutaneous embolization. 22 Thoracic duct damage leading to chylous leakage occurs in 1% to 2.5% of radical neck dissections. 23 In a retrospective review of 221 patients that underwent neck dissection, de Gier et al identified 11 individuals that suffered a chylous fistula. Dietary modifications alone were sufficient to stop the leak in 5 of these patients. The other 6 cases necessitated initiation of total parenteral nutrition. Two of these individuals required surgical re-intervention via a pectoralis major muscle flap transfer. Overall, there were no cases that resulted in permanent damage.
Identification and Management
If left untreated, injury to the thoracic duct can lead to chronic chyle loss and eventually result in significant weakness, dehydration, and emaciation. 24 Unfortunately, intraoperative diagnosis of lymphatic vessel injury can be difficult due to the usual fasting state of patients prior to surgery, which reduces lymphatic production and transport. Positive pressure application with the patient in Trendelenburg position may facilitate identification of a suspected leak. If a leak is observed intraoperatively, suture ligation of the corresponding lymphatic vessel should be carried out. Postoperative presentation of a thoracic duct injury is dependent on the location of the injured vessel, although the presence of a variably cloudy and white fluid (ie, chyle) from an operative drain or upon aspiration is often seen. Conservative management of a chylothorax in these circumstances consists of a low-fat diet or total parenteral nutrition, supportive care (eg, correction of electrolytes, rehydration), and, in severe cases, adequate drainage via insertion of chest tube. 5,25 Treatment with somatostatin or octreotide has also been shown to be effective in treating thoracic duct injury, as it decreases drainage output and results in earlier fistula closure. 26 -28 Definitive management in refractory cases involves ligation of the thoracic duct; 6 however, conservative therapy for at least 1 to 2 weeks is recommended prior to taking this course.
Limitations
Limitations to consider when interpreting the results of this study include the consideration of biases (eg, selection bias, information bias) inherent to retrospective reviews. The multicenter, retrospective nature of the study prevented a standard methodology for identifying, documenting, and monitoring iatrogenic injury postoperatively between various institutions. This variation in follow-up protocols may have resulted in an underreporting of cases of thoracic duct injury occurring during the postoperative period. Additionally, there were likely other cases of thoracic duct injury that would have increased our understanding of the natural history and treatment of this complication that we did not encounter as they occurred on other services (eg, otolaryngology, thoracic surgery).
Conclusion
Complications involving the thoracic duct are rarely encountered during anterior cervical spine operations. Nevertheless, surgeons operating in this area need to remain cognizant of the presence of this critical lymphatic structure and should be cautious of anatomic variants that may increase the risk of injury. The manifestations resulting from thoracic duct disruption are dependent on the degree of injury as well as its location. In many cases, prompt identification of damage to the duct will allow for conservative management and resolution of symptoms without significant long-term effects.
Footnotes
Authors’ Note
This study was ethically approved by the institutional ethics committees at all participating sites.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Adeeb Derakhshan reports grants from AOSpine North America during the conduct of the study; Michael P. Steinmetz reports grants from AOSpine North America during the conduct of the study; Gabriel A. Smith reports grants from AOSpine North America during the conduct of the study; Ziya Gokaslan reports grants from AOSpine North America, personal fees from AO Foundation, grants from AOSpine, outside the submitted work; Michael G. Fehlings reports grants from AOSpine North America during the conduct of the study; K. Daniel Riew reports personal fees from AOSpine International, other from Global Spine Journal, other from Spine Journal, other from Neurosurgery, personal fees from Multiple Entities for defense, plantiff, grants from AOSpine, grants from Cerapedics, grants from Medtronic, personal fees from AOSpine, personal fees from NASS, personal fees from Biomet, personal fees from Medtronic, nonfinancial support from Broadwater, outside the submitted work; Thomas E. Mroz reports other from AOSpine during the conduct of the study, personal fees from Stryker, personal fees from Ceramtec, other from Pearl Diver, outside the submitted work; Daniel Lubelski reports grants from AOSpine North America during the conduct of the study; Mark Corriveau, reports grants from AOSpine North America during the conduct of the study; Sungho Lee, reports grants from AOSpine North America during the conduct of the study; Jonathan R. Pace, reports grants from AOSpine North America during the conduct of the study; Mohamad Bydon, reports grants from AOSpine North America during the conduct of the study; Paul M. Arnold reports grants from AOSpine North America during the conduct of the study; other from Z-Plasty, other from Medtronic Sofamore Danek, other from Stryker Spine, other from FzioMed, other from AOSpine North America, other from Life Spine, other from Integra Life, other from Spine Wave, other from MIEMS, other from Cerapedics, other from AOSpine North America, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by AOSpine North America Inc, a 501(c)3 nonprofit corporation.