
Abstract
Study Design
Systematic literature review.
Objective
The Thoracolumbar Injury Classification and Severity Score System (TLICS) is widely used to help guide the treatment of thoracolumbar spine trauma. The purpose of this study is to evaluate the safety of the TLICS in clinical practice.
Methods
Using the Medline database without time restriction, we performed a systematic review using the keyword “Thoracolumbar Injury Classification,” searching for articles utilizing the TLICS. We classified the results according to their level of evidence and main conclusions.
Results
Nine articles met our inclusion and exclusion criteria. One article evaluated the safety of the TLICS based on its clinical application (level II). The eight remaining articles were based on retrospective application of the score, comparing the proposed treatment suggested by the TLICS with the treatment patients actually received (level III). The TLICS was safe in surgical and nonsurgical treatment with regards to neurologic status. Some studies reported that the retrospective application of the TLICS had inconsistencies with the treatment of burst fractures without neurologic deficits.
Conclusions
This literature review suggested that the TLICS use was safe especially with regards to preservation or improvement of neurologic function. Further well-designed multicenter prospective studies of the TLICS application in the decision making process would improve the evidence of its safety. Special attention to the TLICS application in the treatment of stable burst fractures is necessary.
Introduction
The thoracolumbar spine is the most common site of spinal fractures in many series. Over the years, many classification systems for thoracic and lumbar spine trauma (TLST) have been described in the literature. In 2005, Vaccaro et al proposed a new classification of thoracolumbar injuries that considered the neurologic status, and the authors proposed an injury severity score that could help surgeons in the decision-making process. 1 The Thoracolumbar Injury Classification and Severity Score System (TLICS) is based upon three critical injury characteristics: (1) the morphology of the injury determined by the radiologic patterns, (2) the integrity of the posterior ligamentous complex (PLC), and (3) the neurologic status of the patient. The final calculated score can be utilized to guide conservative (<4 points) or surgical treatment (>4 points), whereas a score of 4 points can be managed according to surgeon's preference.
Many studies have evaluated the TLICS reliability and validity in assessing TLST and guiding treatment. 2 , 3 , 4 However, safety is an important characteristic of a spinal trauma classification system. 5 The most important outcome to be evaluated is the neurologic status of the patient. If a system cannot guide neurologic preservation or improvement, the system may be considered too dangerous to be used.
Although very intuitive and rational, the TLICS is a theoretical proposal to help management of the TLST. The purpose of our study is to identify the safety of the TLICS based upon the reported literature.
Materials and Methods
A literature review was performed using the Medline database without time restriction. The term “thoracolumbar injury classification” was used in the main entry search on February 7, 2015. The general term was used to obtain a comprehensive amount of publications potentially related to the TLICS. The search results were reviewed by two authors (A.F.J. and A.A.P.). Only articles written in English (or translated text) were reviewed. We included only clinical publications, retrospective or prospective, evaluating the safety or validity of the TLICS in patients with thoracolumbar spine trauma. The exclusion criteria included case reports, literature review, paper presentations, or personal communications. Publications evaluating only the reliability of the system without considering its safety were also excluded. Information to determine safety included the patients’ neurologic status as well as the complications from care. The articles selected were then classified according to evidence-based medicine criteria proposed by Wright et al. 6
Results
Search and Screening Results
A total of 355 abstracts were initially identified with our primary search criteria and were reviewed. Nine articles met all inclusion and exclusion criteria. Only one article evaluated the safety of the TLICS based on its clinical application. 7 The eight remaining articles were based on retrospective application of the score comparing the proposal treatment suggested by the TLICS with the treatment patients really received. Two publications evaluating validity had the same methodology but both were included because they had complementary information resulting from different subgroup analysis. 8 , 9 Another two publications reported similar results but were maintained because they had different methodologies and study analysis. 10 , 11 A great heterogeneity was observed in the study design.
Table 1 summarizes the nine papers included in our review.
Summary of the full articles included in our literature review of the clinical validity of the TLICS
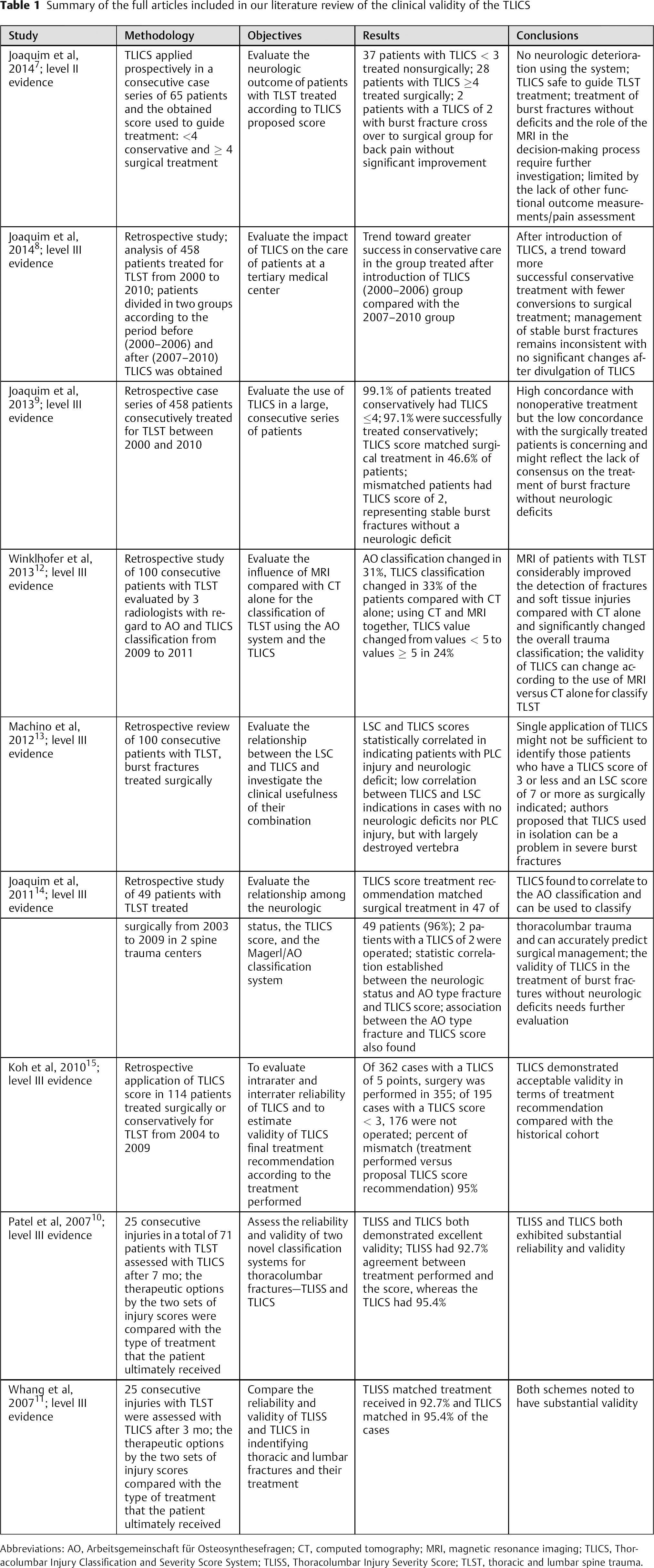
Abbreviations: AO, Arbeitsgemeinschaft für Osteosynthesefragen; CT, computed tomography; MRI, magnetic resonance imaging; TLICS, Thoracolumbar Injury Classification and Severity Score System; TLISS, Thoracolumbar Injury Severity Score; TLST, thoracic and lumbar spine trauma.
Safety
Joaquim et al used the TLICS score to guide treatment in a Brazilian population with spine trauma. A total of 37 patients with TLICS of 3 or less points were initially treated conservatively. 7 All patients were neurologically intact, and no new deficits occurred with the conservative treatment. Late surgery was required in 2 patients with back pain and mild kyphosis, without neurologic worsening. The average TLICS was 1.5 points, ranging from 1 to 2. In the surgically treated group, with 28 patients, no patients had neurological deterioration and those with incomplete deficits improved during follow-up. The average TLICS was 7 points (range 4 to 10 points). Although the authors demonstrated that use of the TLICS in the decision-making process was safe with regards to the neurologic status, the study was limited by its short follow-up, potential underreporting of failures, and lack of other outcome measures, such as pain status or functional disability.
In another study, Joaquim et al evaluated the retrospective application of the TLICS in a series of 458 patients within the United States. Patients were divided in two groups: treated from 2000 to 2006 and from 2007 to 2010. 8 In the first period, the authors reported that TLICS was not utilized in the studied institution and therefore did not affect decision making. From 2007 to 1010, the TLICS utilized and influenced decision making. The authors reported that from 2000 to 2006, the retrospective application of the TLICS matched treatment in 97.9% of the patients treated nonsurgically and in 39.4% of the surgically treated patients. The discordance in 60.6% of patients was due to the surgical treatment of burst fractures without neurologic deficits (TLICS 2). Surgery was required after initial conservative treatment in 7 patients (4.7%): 3 patients with unrecognized PLC injuries, 1 with severe radiculopathy and a burst fracture (TLICS of 4 points), and 2 with severe back pain without deficits. None of the patients had neurologic deterioration.
From 2007 to 2010, initial conservative treatment provided matched with TLICS ≤ 4 in 100% of the 162 patients. However, 2 patients required late surgery, none with neurologic deterioration, for pain and mild deformity. In the surgical group, 52.4% matched the TLICS recommendations (≥4 points). The discordance in 47.5% of patients was also for burst fractures without deficits that had surgery, a decrease from the initial cohort. Although this result suggests that the TLICS can improve surgical decision making, the study was limited by its retrospective application and short follow-up of the majority of patients.
In another study with the same patients but with a global analysis of all the 458 patients together, from 2000 to 2010, the same authors applied the TLICS retrospectively in the whole cohort. 9 From the 310 (67.6%) patients treated conservatively, the TLICS matched recommendations in 307 of 310 (99%), with 3 patients having TLICS of 7 points requiring late surgery. Furthermore, 4 other patients with TLICS < 5 points had surgery: 1 with a TLICS of 4 points (severe radiculopathy and burst fractures) and 3 with burst fractures that were neurologically intact, with intractable pain and/or worsening of kyphosis. In the surgical group, however, the TLICS matched with just 46.6% of the surgical indications. All the discordances in patients were due to burst fractures without neurologic deficits that were neurologically intact (TLICS of 2 points). The authors suggested that lack of standardized criteria for treatment of burst fractures without neurologic deficits was a potential cause for the discordances found between the TLICS score and surgical treatment. The potential limitations of this study include its retrospective nature, as well as the inconsistencies in defining PLC injury based on magnetic resonance imaging (MRI).
Winklhofer et al performed a retrospective analysis of 100 patients with TLST classified according to the Arbeitsgemeinschaft für Osteosynthesefragen (AO) and the TLICS based on the computed tomography (CT) findings by three radiologists. 12 Six weeks after the first analysis of the data, the patients were analyzed using CT and MRI. CT and MRI together increased the number of fractures detected to 196 compared with 162 detected only on CT scan. The TLICS classification changed in 33% patients compared with CT findings alone. CT and MRI findings together changed the decision of conservative treatment (TLICS < 5) to surgical treatment (TLICS > 5) in 24% of the cases. These findings suggested that the safety of the system can be clearly and significantly influenced by the radiologic method used for evaluation, with the addition of MRI increasing the detection of injuries. However, the low specificity of MRI in this setting may also lead to unnecessary surgeries as well.
Machino et al retrospectively reviewed 100 consecutive patients with burst fractures, evaluating the relationship between the Load Sharing Classification (LSC) and TLICS. 13 The patients were classified according to both classifications; the PLC status was classified as injured when diastasis was present in the facet joints, facet perch, or subluxation, splaying the spinous process, as well as when suggestive changes were present on MRI. The patients with PLC injuries had higher TLICS scores (9 ± 1.3 points compared with 4.5 ± 1.7 points; p < 0.001). Interestingly, although the LSC and the TLICS scores had clinical correlation in patients with PLC injury and neurologic deficits, there was a low correlation in cases where the PLC was intact and there was no neurologic impairment. The authors concluded that for patients with low TLICS scores (<4) and severe burst fractures, the TLICS used in isolation was not helpful. They proposed that inclusion of the LSC can lead to a higher agreement between the TLICS score and historical cohorts.
Joaquim et al evaluated retrospectively a series of 49 patients consecutively treated in two Brazilian centers. 14 A total of 47 patients (95.9%) had a TLICS of 4 or more points, with 2 patients having a TLICS of 2. The authors also reported an association between the AO type fractures, the TLICS score, and the neurologic status. They concluded that the historical indications for surgical treatment in their institution were similar to the indications proposed according to the TLICS.
Koh et al applied the TLICS score to 114 patients treated conservatively or surgically between 2004 and 2009. 15 They reported that, among 362 cases with a TLICS of 5 or more points, 355 underwent surgical treatment, and in 195 patients with a TLICS score lower than 3, 176 did not have surgery. In total, the authors reported 95% concordance between treatment performed and the TLICS proposal. The authors concluded that the TLICS had an acceptable validity in terms of the treatment recommendations within this historical series.
Whang et al evaluated the validity of the TLICS with 25 consecutive injuries treated consecutively, reassessing the score 3 months after the first evaluation. 11 They found that the TLICS matched with treatment performed in 95.4% of the cases, reporting substantial validity. The same agreement rate was obtained with the study performed by Patel et al, who also analyzed 25 patients and assessed the TLICS 7 months after the first assessment. 10
Discussion
The current evidence in evaluating the safety of the TLICS is favorable. The TLICS has been demonstrated to provide concordant treatment recommendations compared with historical controls and that treatment rendered in accordance with the TLICS demonstrates the maintenance or improvement of patients’ neurologic status. 7
An important problem raised in our review is that the retrospective evaluation of the TLICS had inconsistencies with the treatment of burst fractures without neurologic deficits. 8 , 9 , 13 , 14 Potential explanations for the inconsistencies are that many different surgical indications can be found in the spine trauma literature for treatment of stable burst fractures, such as loss of vertebral body height, segmental kyphosis, vertebral body comminution, canal compromise, among many others. 16 The TLICS did not consider any one of these factors for guiding surgical treatment, as none have shown any evidence-based relationship with patients’ outcome. 1
Another potential explanation for inconsistencies in the retrospective application of the TLICS is that the score can change according to the type of radiologic assessment. For instance, addition of MRI in the evaluation, as reported by Pizones et al and Winklhofer et al, has been shown to change the final TLICS score. 12 , 17 Although spinal MRI is not part of routine care in many trauma centers, studies suggested that it can be useful and can add additional information. 17 , 18 However, the role of the MRI in the evaluation of the TLST, especially on the PLC status, had been debated due to concerns about the specificity of abnormal MRI findings. 19
Finally, the last potential problem in evaluation of the TLICS safety is the lack of a gold standard for measuring the outcomes of using the TLST. There are many studies in the literature evaluating outcomes of specific injuries patterns, such as burst fractures with or without neurologic deficits of severe dislocations. 20 , 21 , 22 However, the lack of a widely adopted standard, with a patient-based outcomes system, limited our ability to assess the utility of the TLICS and the conclusions of our study. For this reason, we suggest that a well-designed, prospective multicenter study evaluating the TLICS impact on patient's outcome is needed.
Conclusions
This literature review suggested that use of the TLICS is safe, especially with regards to neurologic status both in surgical and nonsurgical treatment. The neurologic status preservation, with improvement in patients with incomplete deficits, was also obtained with the prospective use of TLICS in the decision-making process.
Further well-designed, multicenter, prospective studies of the TLICS application in the decision-making process would improve the evidence of its safety. Special attention to the TLICS application in the treatment of stable burst fractures with incorporation of standardized patient reported outcomes is necessary.
Disclosures
Andrei Fernandes Joaquim, none
Dhiego Chaves de Almeida Bastos, none
Hélio Henrique Jorge Torres, none
Alpesh A. Patel, Consultant: Depuy, Zimmer, Stryker, Biomet; Owner/shareholder company: Amedica, Nocimed, Vital 5, Cytonics; Royalties: Biomet, Ulrich, Amedica