
Abstract
Study Design
Prospective study.
Objective
Because single-level disk arthroplasty or arthrodesis in the lower subaxial spine improves headaches after surgery, we studied whether this effect may be better appreciated after two-level arthroplasty.
Methods
We performed an independent post hoc analysis of two concurrent prospective randomized investigational device exemption trials for cervical spondylosis, one for single-level treatment and the other for two adjacent-level treatments.
Results
For the one-level study, baseline mean headache scores significantly improved at 60 months for both the cervical disk arthroplasty (CDA) and anterior cervical diskectomy and fusion (ACDF) groups (p < 0.0001). However, mean improvement in headache scores was not statistically different between the investigational and control groups from 6 months through 60 months. For the two-level study, baseline mean headache scores significantly improved at 60 months for both the CDA and ACDF groups (p < 0.0001). The CDA group demonstrated greater improvement from baseline at all points; this difference was statistically significant at 6, 12, 24, 36, and 48 months but not at 18 and 60 months.
Conclusion
Both CDA and ACDF at either one or two levels are associated with sustained headache relief from baseline. Patients undergoing two-level arthroplasty had significantly greater improvement in headache at all points except for at 18 and 60 months. This difference in improvement was not observed in patients undergoing single-level arthroplasty. The mechanism of greater headache relief after two-level arthroplasty remains unclear.
Introduction
Sjaastad first coined the term “cervicogenic headache” in 1983 to describe headache referred from the neck. 1 , 2 An estimated 1 to 4% of the general population experiences cervicogenic headaches. 3 , 4 , 5 The international Headache Society (IHS) first described the criteria for cervicogenic headache in 1988 and updated the criteria in 2004. 2 Although the criteria have evolved throughout the years, the underlying clinical feature is pain originating in the neck that radiates unilaterally to the frontal, parietal, and orbital regions. The IHS proposed diagnostic criteria for cervicogenic headache that include pain referred from the neck and involving the head and/or face, clinical or radiographic evidence that suggests a cervical spine lesion, elimination of the headache after diagnostic blockade, and pain resolution 3 months after treatment. 3 For the diagnostic blockade, pain anesthesiologists target the C1–C2 joint, the C2–C3 joint, and C3–C4 joint to provide possible relief and objective evidence of a cervical source of the headache. 6 , 7 Various mechanisms to explain cervicogenic headache have been proposed, including the role of spinal kinematics. 3 Although cervicogenic headache was previously thought to be associated with upper cervical spine pathology (C1–C3), the treatment of lower surgical pathology results in headache relief. 8 , 9 , 10 , 11 Recent work by Schrot et al has illustrated not that only was lower cervical disk disease an apparent headache generator, but also that differences in headache relief after upper- or lower-level subaxial surgery was not observed. 9
Cervical total disk replacement in comparison with fusion has equivalent or better outcomes. 12 , 13 In addition, the recent long-term data demonstrates that cervical disk arthroplasty (CDA) not only preserves motion at the index level but also reduces adjacent-segment disease compared with fusion procedures. 7 , 14 , 15 , 16 Although Riina et al found that patients undergoing single-level arthroplasty had greater headache relief in comparison with patients undergoing arthrodesis, our group did not find a significant difference between the two groups using a similar data set for single-level surgeries. 8 , 9 Comparing the data from a two-level arthroplasty versus fusion may better resolve this difference if improved cervical spine biomechanics contributes to headache relief.
A prospective, randomized, controlled multicenter study of two-level anterior cervical disk surgery conducted by Davis et al reported improved neck disability index (NDI) and visual analog scale (VAS) neck pain scores for arthroplasty compared with fusion at 2 years. 17 If headache relief is facilitated by improved cervical kinematics after arthroplasty, patients undergoing two-level arthroplasty may experience even greater headache relief than patients undergoing two-level fusion surgery.
In this study, we analyzed the 5-year follow-up data from a prospective randomized investigational device exemption (IDE) clinical trial to evaluate the following: the incidence of cervicogenic headache in patients suffering from myelopathy or radiculopathy who undergo surgery, the temporal change in headache score after surgery, and the difference, if any, between one- and two-level CDA and arthrodesis. In addition, demographic variables of interest (i.e., age, gender, and body mass index [BMI]) were analyzed to determine their effect on headache relief. No study to date has compared headache relief between one- and two-level anterior cervical surgery and between CDA and arthrodesis.
Methods
Subjects and Study Design
A detailed description of surgical technique and the IDE study design has been previously reported. 17 Patients underwent surgery as part of a Food and Drug Administration IDE prospective, randomized clinical trial between April 2006 to March 2008 at 24 clinical sites in the United States. This study was approved by the University of California Davis Institutional Review Board (no. 217014). The study inclusion criteria (Fig. 1) were patient age 18 to 69 years with a diagnosis of degenerative disk disease with associated radiculopathy or myeloradiculopathy at a single level or at two contiguous levels from C3 to C7. The study required patients to have radiographic findings that correlated with their symptomatology and to have failed nonoperative management for at least 6 weeks or to have demonstrated progressive worsening of symptoms, calling for urgent surgery. The exclusion criteria are detailed in Fig. 2.
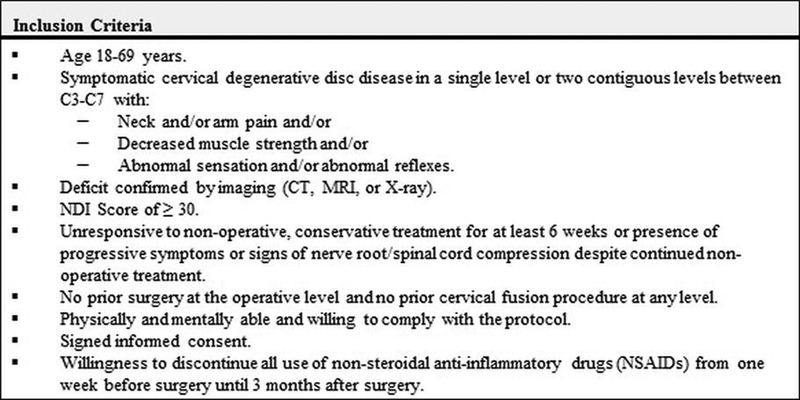
Study inclusion criteria. Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; NDI, neck disability index.
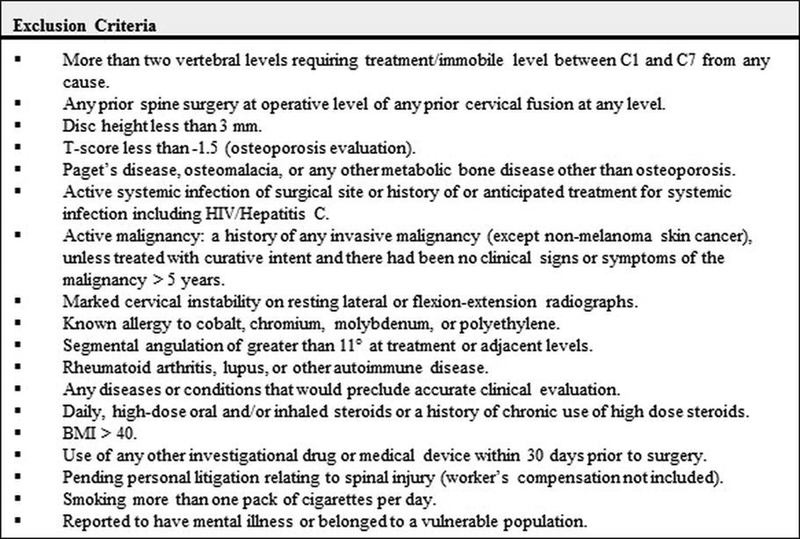
Study exclusion criteria. Abbreviations: BMI, body mass index; HIV, human immunodeficiency virus.
Patients were randomized in a 2:1 ratio (CDA to anterior cervical diskectomy and fusion [ACDF]) resulting in 164 patients receiving treatment with a Mobi-C Cervical Artificial Disc (LDR Medical, Troyes, France) at a single level, 225 patients receiving treatment with a Mobi-C Cervical Artificial Disc at two contiguous levels, 81 patients receiving corticocancellous allograft and anterior cervical plate using the standard ACDF technique at a single level, and 105 receiving the same ACDF treatment at two contiguous levels. An additional 24 patients (15 one-level, 9 two-level) were treated with the CDA device as training cases. This study only includes data from the randomized patients; the training cases were excluded from the analysis. It was not possible to blind the treating surgeons to the treatment. The patients were unblinded after surgery, because the postoperative radiographs viewed by the patient and clinician made the treatment readily apparent.
Postoperative care was left to the discretion of the treating surgeon. Patients were evaluated preoperatively and postoperatively at 6 weeks and 3, 6, 12, 18, 24, 36, 48, and 60 months. Patients were asked to refrain from taking nonsteroidal anti-inflammatory drugs from a week before surgery to 3 months after surgery. An exception was made for patients having CDA who were diagnosed with postsurgical heterotopic ossification.
Clinical Outcomes
The baseline demographics collected included height, weight, BMI, age, gender, race, ethnicity, working status, smoking status, and driving status. Assessment of pain and function outcome included the NDI. NDI is collected as a 10-section, self-reported questionnaire. Each question is scored on a scale of 0 to 5. In this study, the NDI headache component was used to assess headache outcome. The response scoring scale was as follows: 0, “I have no headaches at all”; 1, “I have slight headaches, which come infrequently”; 2, “I have moderate headaches, which come infrequently”; 3, “I have moderate headaches, which come frequently”; 4, “I have severe headaches, which come frequently”; and 5, “I have headaches almost all the time.”
Statistical Analysis
Wilcoxon signed rank tests were used to compare the change from baseline within the treatment groups. Two-tailed t tests were used to compare the mean improvement between the treatment groups at each postoperative time point. Analysis of variance was used to test the mean improvement across demographic groups. A p value less than 0.05 was considered significant.
Results
Treatment at One Level
At 60 months, NDI data was available for 82.9% (136/164) of patients having one-level CDA and 70.4% (57/81) of patients having one-level ACDF. The mean range of motion was maintained in the CDA group in both flexion–extension (10.3 ± 6.8 degrees) and lateral bending (5.5 ± 3.4 degrees) compared with baseline (8.2 ± 4.5 degrees, 5.0 ± 2.9 degrees, respectively). The mean range of motion in the ACDF group was effectively eliminated in flexion–extension (0.7 ± 1.1 degrees) and lateral bending (0.7 ± 1.0 degrees) compared with baseline (7.5 ± 4.1 degrees, 5.4 ± 3.2 degrees, respectively). For patients having one-level CDA, severe heterotopic ossification (continuous bridging bone and <2 degrees angular motion) was present in 8.5% of treated levels. Patients with continuous bridging bone and <2 degrees angular motion demonstrated similar NDI headache scores compared with the other patients having CDA.
The baseline distribution of headache scores was similar between the groups with the most frequent headache response being 3 for both groups (Fig. 3A). The percentage of patients reporting a score of 3 or more was 50.6% for patients having CDA and 53.0% for patients having CDF. The baseline mean headache scores were also similar between the two groups. The baseline mean headache scores significantly improved from a baseline of 2.52 ± 1.45 and 2.41 ± 1.57 to 1.25 ± 1.24 and 1.05 ± 1.05 at 60 months for both the CDA and ACDF groups, respectively (p < 0.0001).
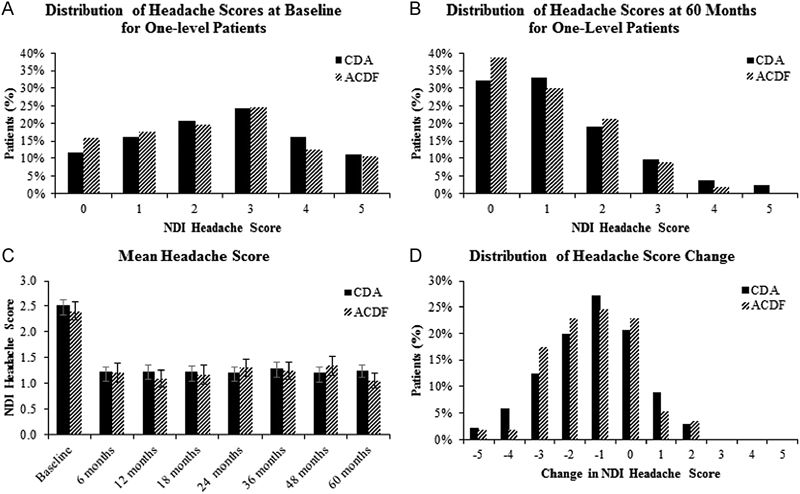
(A) The distribution of headache scores at baseline for patients having one-level cervical disk arthroplasty (CDA) and patients having anterior cervical diskectomy and fusion (ACDF). (B) The distribution of headache scores at baseline for the one-level group at 60 months. At 60 months, the distribution of headache scores shifted noticeably toward lower scores, indicating a significant reduction in pain for both groups. (C) The mean neck disability index (NDI) headache score of patients having CDA and patients having ACDF from baseline to 60 months’ follow-up. Error bars represent standard error. (D) The distribution of changes in headache score from baseline to 60 months. Although the majority of patients experienced some degree of pain relief, a minority of patients experienced no change or an increase in headache score from baseline.
Both the investigational and control groups experienced a significant improvement from the baseline headache scores at each point up to 60 months (p < 0.0001). The distribution of headache scores shifted noticeably toward lower scores with the most common headache score being 1 for the CDA group and 0 for the ACDF group (Fig. 3B). At 60 months, the percentage of patients reporting a score of 3 or more was 15.4% for patients having CDA and 10.5% for patients having ACDF, a nonsignificant difference (p = 0.5). The CDA group had a mean headache score improvement of 1.24 ± 1.53 from baseline, and the ACDF group experienced a similar mean improvement of 1.26 ± 1.43. The mean improvement in headache scores was not statistically different between the investigational and control groups at each point from 6 months through 60 months (Fig. 3C). The most common improvement in headache score was by 1 point for both groups (Fig. 3D). Additionally, 11.8% (12/136) of patients having CDA experienced an increase in headache score of 1 to 2 points more from baseline compared with 8.77% (5/57) of patients having ACDF, though this difference was not statistically significant (p > 0.99).
The mean improvement in headache score was not significantly different between the demographic groups stratified by age, gender, and BMI in both the single-level and two-level cohorts (Tables 1 2).
Headache data for patients having one-level treatment stratified by age, gender, and BMI
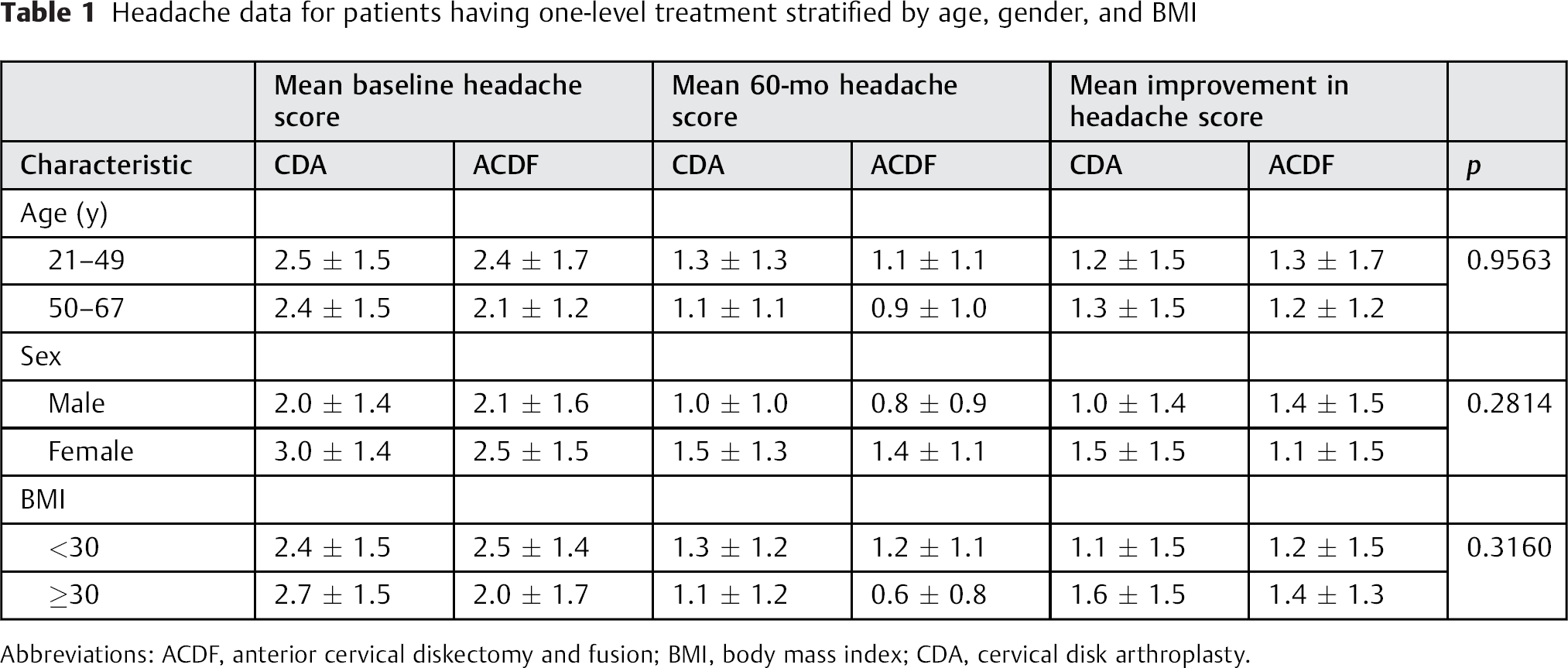
Abbreviations: ACDF, anterior cervical diskectomy and fusion; BMI, body mass index; CDA, cervical disk arthroplasty.
Headache data for patients having two-level treatment stratified by age, gender, and BMI
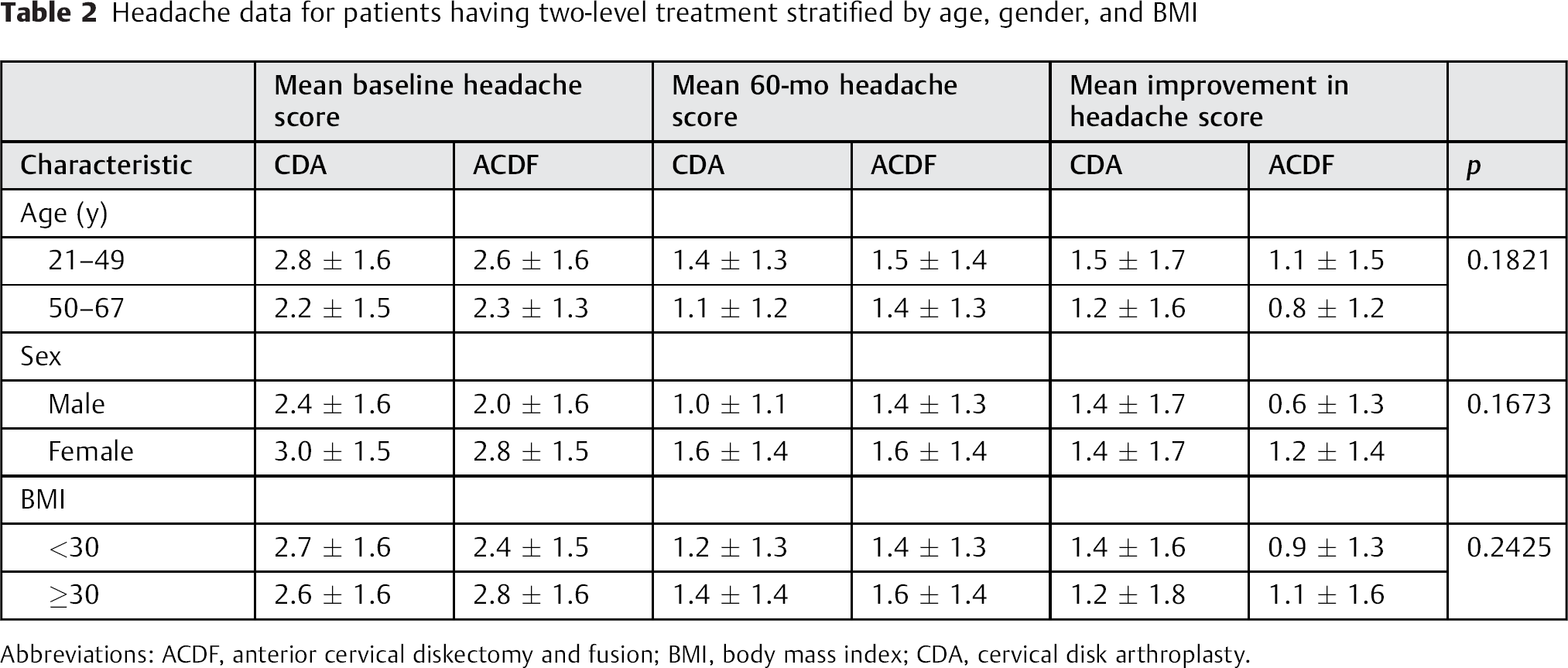
Abbreviations: ACDF, anterior cervical diskectomy and fusion; BMI, body mass index; CDA, cervical disk arthroplasty.
Treatment at Two Levels
At 60 months, data was available for 85.3% (192/225) of patients having two-level CDA and 70.5% (74/105) of patients having two-level ACDF. As in the one-level cohort, the mean range of motion was maintained in the two-level CDA group in both flexion–extension (superior: 10.1 ± 6.1 degrees, inferior: 8.4 ± 5.0 degrees) and lateral bending (superior: 5.6 ± 3.6 degrees, inferior: 5.1 ± 3.5 degrees) compared with baseline (superior: 9.1 ± 4.8 degrees, inferior: 7.4 ± 4.3 degrees; superior: 5.8 ± 3.4 degrees, inferior: 4.9 ± 3.4 degrees). The mean range of motion in the ACDF group was eliminated in flexion–extension (superior: 0.3 ± 0.3 degrees, inferior: 0.6 ± 0.9 degrees) and lateral bending (superior: 0.8 ± 1.9 degrees, inferior: 0.6 ± 0.7 degrees), compared with baseline (superior: 9.3 ± 4.9 degrees, inferior: 7.1 ± 3.9 degrees; superior: 5.5 ± 3.0 degrees, inferior: 4.8 ± 2.9 degrees). For patients having two-level CDA, severe heterotopic ossification (continuous bridging bone and <2 degrees angular motion) was present in 5.9% of superior levels and 5.4% of inferior levels. Patients with continuous bridging bone and <2 degrees angular motion demonstrated similar NDI headache scores compared with other patients having CDA.
The distribution of headache scores at baseline was similar between the groups with the most frequent headache response being scored 3 for the two-level CDA group and 2 and 3 for the two-level ACDF group (Fig. 4A). At baseline, 55.1% of patients having CDA and 51.4% of patients having ACDF reported a score of 3 or more. The mean baseline headache scores were similar between the two groups. The baseline mean headache scores significantly improved from 2.65 ± 1.56 and 2.49 ± 1.58 to 1.29 ± 1.30 and 1.50 ± 1.34 at 60 months for both the CDA and ACDF groups, respectively (p < 0.0001).
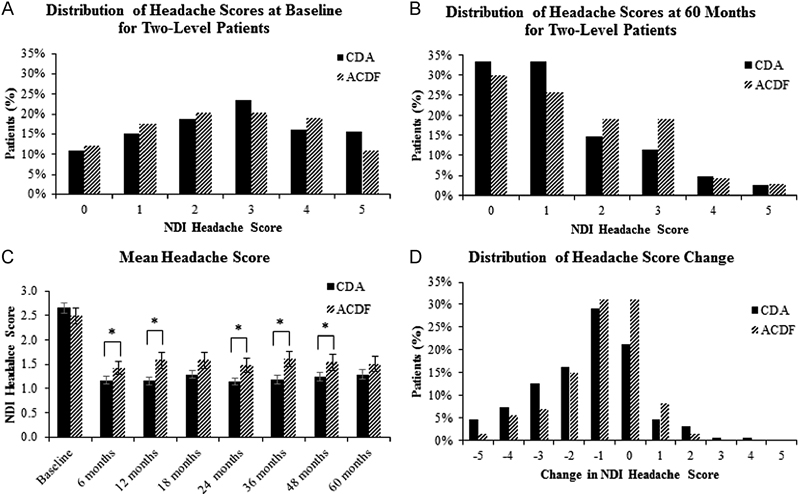
(A) The distribution of headache scores at baseline for patients having two-level cervical disk arthroplasty (CDA) and patients having anterior cervical diskectomy and fusion (ACDF). (B) The distribution of headache scores for the two-level group at 60 months. At 60 months, the distribution of headache scores shifted noticeably toward lower scores, indicating a significant reduction in pain for both groups. (C) The mean neck disability index (NDI) headache score of patients having CDA and patients having ACDF from baseline to 60 months’ follow-up. Patients having CDA demonstrated a greater mean improvement than patients having ACDF at 6, 12, 24, 36, and 48 months. Asterisks denote a statistically significant difference in mean change from baseline (p < 0.05). Error bars represent standard error. (D) The distribution of changes in headache score from baseline to 60 months for the two-level group. The majority of patients experienced some degree of pain relief. A minority of patients experienced no change or an increase in headache score from their baseline measurement.
Both the two-level CDA group and the two-level ACDF group experienced a significant improvement from the baseline headache scores at each point up to 60 months (p < 0.0001). As in the one-level cohort, the distribution of headache scores shifted significantly toward lower scores at 60 months’ follow-up. At 60 months, the most common headache score was 0 and 1 for the CDA group and 0 for the ACDF group (Fig. 4B). The percentage of patients with a score of 3 or higher decreased from 55.1 to 18.8% in the CDA group and from 51.4 to 25.7% in the ACDF group. The CDA group demonstrated a statistically significant greater improvement from baseline compared with the ACDF group at 6, 12, 24, 36, and 48 months (Fig. 4C). At 18 and 60 months, patients undergoing CDA experienced a greater mean improvement in headache scores that approached but did not reach statistical significance. At 18 months, the investigational group had a mean improvement in headache of 1.28 ± 1.29 compared with 1.57 ± 1.47 (p = 0.051). Similarly at 60 months, the CDA group had a mean improvement in headache score of 1.37 ± 1.68 compared with the ACDF group 0.986 ± 1.37 (p = 0.0824).
The most common improvement in headache score was by 1 point for both the CDA population and the ACDF population (Fig. 4D). Additionally, 8.85% (17/192) of patients having CDA experienced headaches worsening by 1 to 4 points from baseline compared with 9.46% (7/74) of patients having ACDF who experienced worsening headache scores of 1 to 2 points from baseline.
As in the one-level cohort, the mean improvement in headache score was not significantly different between the demographic groups stratified by age, gender, and BMI (Table 2). Female patients in the control group had nearly twice the improvement in headache scores than their male counterparts. However, this difference was not statistically significant (p = 0.17) and may be attributed to numerically higher baseline headache scores for female patients in the ACDF group. Although male and female patients did not demonstrate significantly different improvement in headache scores, it is interesting to note that female patients in the CDA and ACDF populations for both one-level and two-levels of treatment reported more headache than their male counterparts at baseline and at 60 months.
Discussion
The exact mechanism of cervicogenic headaches has not been elucidated. Moreover, the precise definition of cervicogenic headache continues to be debated among different groups. The mechanism of referred pain can be explained by nociceptive afferents from C1, C2, and C3 spinal nerves that synapse onto second-order neurons in the trigeminocervical nucleus. This nucleus also receives afferents from the ophthalmic division of the trigeminal nerve. This convergence described by Bogduk and Govind can help explain the referral of pain to the frontoparietal and orbital regions of the head. 3 Additional studies have shown that stimulation of the rostral spine evokes referred pain to the occipital, frontal, and orbital regions of the head, whereas stimulation of the caudal cervical spine elicits pain mainly in the occipital region. 3 , 18
The association between cervical nerve roots below C3 and headache is not as well understood. Cervicogenic headache arising from the lower cervical spine was first described by Diener et al, who theorized that nociceptive afferents from the lower cervical roots also converge on the cervical trigeminal nucleus. 2 Persson et al analyzed headaches in patients with cervical radiculopathy from the lower cervical spine. Selective nerve root blocks of the pathologic level produced a 50% or more reduction in headache with 69% of these patients reporting complete relief of headache using the VAS. 19 This study lends support to the theory that cervicogenic headache has the potential to be relieved with diskectomy in the lower cervical spine (in addition to the upper cervical levels).
Attempts have also been made to correlate cervicogenic headaches with a sympathetic phenomenon in patients with cervical spondylosis. Barre and Lieou first described these sympathetic symptoms in 1926, which include vertigo, headache, dizziness, and hyperhidrosis. 20 , 21 Li et al noted an association between anterior cervical diskectomy and improvement in these sympathetic symptoms, including headache. They hypothesized that headache relief was mediated by the removal of sympathetic nerve fibers contained within the posterior longitudinal ligmament. 21 In the one- and two-level clinical trials studied here, resection of the posterior longitudinal ligament was left to the discretion of the operating surgeon for both arthroplasty and arthrodesis treatment. 2
As noted above, cervicogenic headaches improve after anterior cervical diskectomy procedures. Schofferman et al first demonstrated headache relief after cervical arthrodesis in the upper cervical levels C2–C5. 22 Riina et al reported headache relief after either single-level arthroplasty or arthrodesis with 2-year follow-up, and patients having arthroplasty experienced even greater headache improvement compared with the patients having ACDF. 8 This result was different from another one-level analysis with 2-year follow-up, which showed no significant difference in headache relief between arthrodesis and arthroplasty. 9 Both single-level procedures, however, showed a significant improvement in headache when compared with baseline.
The mechanism for headache relief may be multifactorial, and the putative mechanisms include neuroanatomic connections of the trigeminocervical nucleus with lower cervical roots; sympathetically innervated structures, which are then denervated by surgery; relief of cerebrospinal fluid obstruction during systole caused by focal spinal stenosis; and kinesthetic improvements in the cervical spine after surgery, either through improved spinal biomechanics or relief of reflex muscle spasm. To further investigate the role that improved spinal biomechanics may have in relief of headache after anterior disk surgery, we broadened our analysis to include patients undergoing two-level surgery and with follow-up out to 5 years. We assumed that the loss versus preservation of two contiguous motion segments may have a greater impact on spinal kinesiology compared with analysis at only a single level. Indeed, Pimenta et al has shown that multilevel cervical arthroplasty when compared with single-level arthroplasty allows for a greater improvement in NDI and VAS scores. 14 Cervicogenic headaches, however, were not specifically analyzed in the study by Pimenta et al.
We found a statistically significant difference in the headache scores between the two-level procedures at all points except for 18 and 60 months. There was no difference in headache relief between the groups in patients undergoing only a single-level surgery. Both the two-level and single-level data analysis showed an improvement in headache from baseline, with the patients having two-level CDA experiencing a greater mean improvement in headache. Although the two-level CDA group demonstrated statistically significant improvement compared with ACDF at most points, there was no difference between the two groups at the last follow-up (60 months). It remains to be seen if the difference favoring the arthroplasty group will reemerge with even longer follow-up. Therefore, we are not able to draw conclusions on the clinical relevancy on the difference between CDA and ACDF.
We suggest that an improvement in spine kinematics may improve headaches and that the effect is more apparent with multilevel arthroplasty. With multilevel CDA, each vertebral segment remains biomechanically distinct, unlike with arthrodesis, which consolidates motion segments. 7 , 14 , 15 With the longer lever arm of multilevel fusion, spine kinematics is more adversely affected than with single-level fusion. However, we are not able to make a definitive conclusion, as kinematic measures were not analyzed in this study and the difference was not statistically significant at all points. Additional studies that measure the biomechanical profile at the index level and adjacent levels up to 5 years after surgery and its effects on headache relief can be done to help elucidate these relationships.
Importantly, both the fusion and arthroplasty groups had statistically significant headache relief at all points up to 60 months compared with baseline. A fundamental assumption of cervical disk arthroplasty is that loss of a motion segment is detrimental to spinal biomechanics and that preservation or restoration of motion at that segment is beneficial. Yet patients with two-level fusion still improved significantly with respect to headache scores compared with baseline. If one postulates that improvement in spinal biomechanics alone mediates headache relief, then one must assume that for fusion, the correction of deformity through the restoration of intervertebral height or lordosis improves spinal biomechanics independent of segmental motion preservation. Alternatively, additional mechanisms such as those listed above must play a role.
Previously, we reported headache outcomes for patients having one-level fusion and arthroplasty through 24 months postsurgery. We used a mixed-models repeated-measures regression to assess the postoperative pain relief and to establish a significant trend of gradually worsening pain from 6 weeks to 1 year, followed by the maintenance of pain relief from 1 to 2 years. The model accounted for differences in treatment type as well as differences in operative level. Here, we have chosen not to construct a new model or update the previous model, but focus rather on the comparative outcomes of ACDF and CDA through 5 years, extending our analysis to include a separate assessment of patients having two-level treatment. Unlike the previous 2-year analysis, this assessment does not model trends in pain attenuation nor does it account for differences in operative level. However, we were able to demonstrate that both patients having ACDF and patients having CDA maintained significant improvement from baseline headache scores through 5 years (p < 0.0001). Whether a trend in worsening pain exists as it did between 6 weeks and 12 months remains unclear, as does the effect of treatment level on long-term headache outcomes.
Limitations of this study include the inability to definitively diagnose cervicogenic headache in our patient population based on the diagnostic criteria proposed by the IHS. These patients did not undergo a diagnostic blockade to provide objective evidence of a cervical source of headache. As stated in published studies using similar methodology, 3 , 4 headache assessment using a component of the NDI only provides a very basic headache questionnaire, and thus specific headache characteristics are not captured More detailed prospective studies that precisely qualify cervicogenic headaches should be done to corroborate our findings, as this study was a post hoc analysis of prospectively collected data.
Conclusion
At 5 years, patients who undergo single- or two-level anterior cervical diskectomy procedures benefit from improvement in their baseline headaches. For one-level surgery, the mean improvement in headache scores was not statistically different between the investigational and control groups at all time points. In contrast to the one-level cohort, patients receiving two-level CDA showed a greater improvement in mean headache scores from baseline at all points except for at 18 and 60 months. We also show that headache scores were not significantly different between the demographic groups for either one-level or two-level surgery. Although headache was apparently relieved after either arthroplasty or fusion, headache was relieved by two-level arthroplasty more so than by two-level fusion, and this difference was not observed in the single-level arthroplasty trial. Improved kinematics after arthroplasty may play a role but headache alone should not be the indication for surgery.
Disclosures
Jonathan J. Liu, Grant: LDR
Gilbert Cadena, Grant: LDR
Ripul R. Panchal, Grant: LDR; Consultancy: Mizuho, Precision Spine, Biomet; Speakers’ bureau: Globus; Manuscript preparation: Baxter
Rudolph J. Schrot, none
Kee D. Kim, Grant: LDR; Speakers’ bureau: Globus; Royalties: Precision Spine, LDR, Globus; Educational presentations: Globus; Stock/stock options: Molecular Matrix, Inc.
Financial and Material Support
This work was supported by the UC Davis Department of Neurological Surgery and the UC Davis Spine Center. The LDR Company provided access to data as well as the statistical analysis for this manuscript. LDR provided no financial support for this manuscript.
Footnotes
Acknowledgments
The authors would like to thank Kyle Marshall from LDR for his expertise in statistical analysis and data interpretation.