
Abstract
Study Design
Retrospective study.
Objective
Traumatic atlanto-occipital dissociation (AOD) remains a diagnostic challenge, and delay in diagnosis is associated with catastrophic outcomes. Recently, a revised version of the condyl–C1 interval (CCI) utilizing parasagittal computed tomography (CT) reconstruction was used successfully with unilateral dislocation of 2.5 mm at the level of that joint diagnostic of AOD. We report the utility of this simple technique in the diagnosis of six patients with AOD.
Methods
Two blinded neurosurgeons assessed CTs of six patients with AOD and 30 patients without AOD. The following methodologies were applied: basion–dens interval (BDI), basion–axial interval (BAI), Lee X-lines, Powers ratio, CCI, and revised CCI. The average sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) as well as the kappa statistic indicating interrater reliability of each method were investigated.
Results
The average sensitivity for BDI, BAI, Lee X-lines, Power ratio, CCI, and revised CCI was 0.75, 0.33, 0.67, 0.50, 1.00, and 1.00, respectively. The average specificity was 1.00, 1.00, 0.50, 1.00, 0.94, and 1.00, respectively. The average PPV was 1.00, 1.00, 0.25, 1.00, 0.80, and 1.00, respectively. The average NPV was 0.96, 0.88, 0.89, 0.91, 1.00, and 1.00, respectively, and the kappa statistic was 0.57, 0.25, 0.25, 0.20, 1.00, and 1.00, respectively.
Conclusion
Based on this study, the revised CCI method is simple yet the most sensitive and reliable technique for the diagnosis of AOD.
Keywords
Introduction
Traumatic occipitocervical dislocation, also known as atlanto-occipital dislocation (AOD) or dissociation, accounts for up to 20% of fatalities during high-speed blunt trauma accidents. 1 This highly unstable upper cervical spine injury is associated with mortality and morbidity as a result of respiratory arrest and quadriplegia secondary to injury to the cervicomedullary junction region. 2 , 3 , 4 In the recent years, reports indicting favorable outcomes have emerged reflecting improvements in the emergency management, transport, and, most importantly, recognition of this injury. 5 , 6 , 7 , 8
Most of the current diagnostic modalities and techniques used in diagnosing AOD are originally based on plane X-ray radiographic measurements. 3 , 9 , 10 , 11 , 12 Very few reports have investigated the applicability of these techniques to computer tomography (CT) scans, which are the standard of care in assessing patients with suspected cervical spine injuries. 6 , 13 According to the most recent Congress of Neurological Surgeons/American Association of Neurological Surgeons recommendations, the condyle–C1 interval (CCI) in the CT coronal plan is the preferred technique used in diagnosing AOD. 3 However, similar to the other techniques, the sensitivity and utility of this modality are still lacking. Moreover, some of these techniques are complex and operator-dependent with variable reproducibility. 6
Because the dislocation occurs at the level of the condyle and lateral mass of C1 joint, a better appreciation of its occurrence would be visualization of the dislocation in the sagittal plane following CT reconstruction. A simple method to diagnose AOD using sagittal CT reconstruction was proposed by Gire et al in 2013. 6 The technique is a revised version of Pang CCI, 14 , 15 where unilateral dislocation of the condyle lateral mass interval of more than 2.5 mm in the sagittal plane is considered diagnostic of AOD.
We report our experience in managing six patients with AOD. The modified or revised CCI along with other commonly used methodologies were retrospectively applied to these patients and to a cohort of 30 patients without AOD.
Methods
Ethics Statement
Institutional Review Board (IRB) approval was obtained from both institutions for this study (Northwestern University IRB [STU00099266] and University of Iowa IRB-01 Biomedical [201407771]). Prior to analysis, all the patient information was anonymized and deidentified.
Data Collection
We conducted a retrospective review of all adult patients (age > 18 years) diagnosed with AOD admitted to two level I trauma centers between January 2009 and January 2014. Six patients were identified with AOD. The electronic medical charts were reviewed. A cohort of 30 patients who were evaluated with a CT scan of the cervical spine for nontraumatic reasons were identified as a control group. Radiographic CT assessments were conducted by two blinded spine fellowship–trained neurosurgeons with expertise in managing traumatic spine injuries. These included the most common methods used in diagnosing AOD: basion–dens interval or index (BDI), 16 basion–axis interval (BAI), 10 Lee X-lines, 11 Powers ratio, 12 CCI, 14 , 17 as well as the modified or revised CCI utilizing sagittal CT reconstruction at the level of the condyle lateral mass of C1 joint. 6 The CT measurements were done using the picture archiving and communication system. All patients with AOD had grade II occipitoatlantal injury according to the classification of Horn et al. 18
To make the diagnosis of AOD, the BDI should be >12 mm, BAI > 12 mm, Powers ratio > 1, CCI > 2 mm, or X-lines of Lee rule should be violated (Fig. 1). The revised CCI includes the presence of a unilateral and or bilateral malalignment or dislocation between the occipital condyle and the C1 lateral mass socket in the sagittal plane of >2.5 mm (Fig. 2).
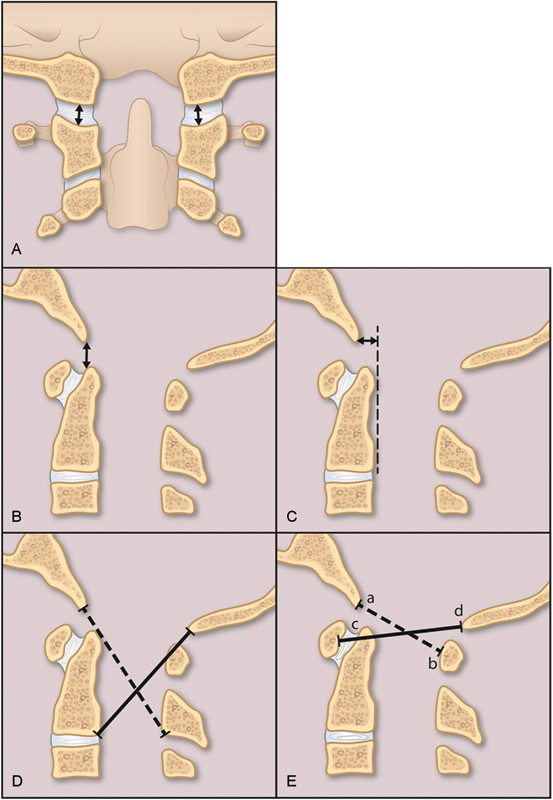
Various methodologies used to diagnose atlanto-occipital dissociation. (A) The condyle–C1 interval in the coronal plane > 2 mm; (B) basion–dens interval > 12 mm; (C) basion–axial interval > 12 mm (dotted line represents the posterior border of the dens); (D) violation of X-lines of Lee rule (dotted line is drawn from the basion to the anterior base of the spinous process of C2, and the continuous line is drawn from the opisthion to the posterior base of C2 vertebral body); and (E) Powers ratio (ab/cd) > 1 (dotted line is drawn from the basion to the posterior arch of C1, and the continuous line is drawn from the opsithion to the anterior arch of C1; a = basion, b = posterior arch of C1, c = anterior arch of C1, d = opisthion).
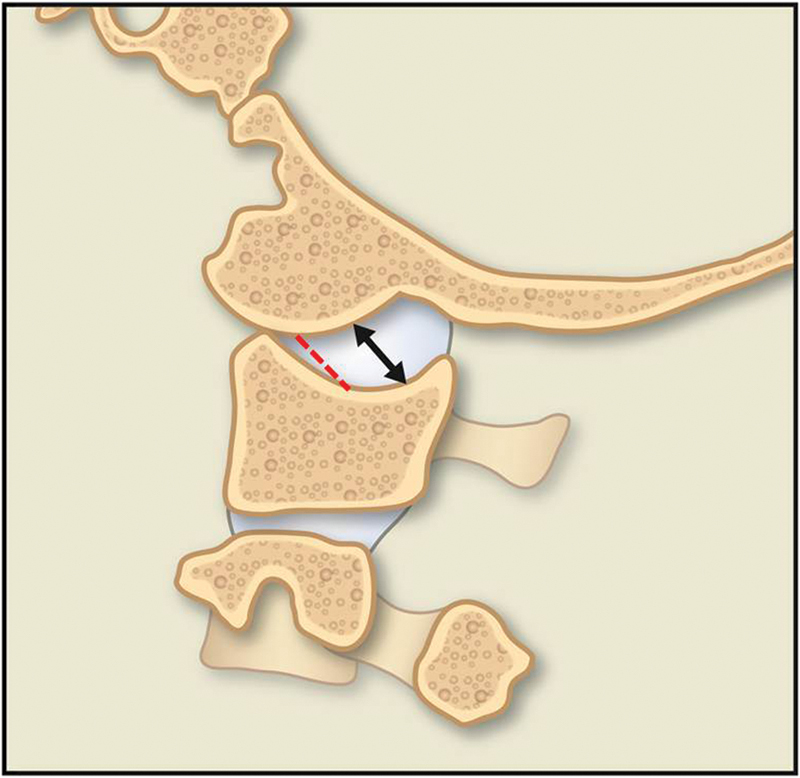
The revised CCI. Dislocation (arrows) in the parasagittal plane at the level of the condyle C1 joint of >2.5 mm measured from the bottom of the C1 condyle to the bottom of the “valley” of the C1 socket (dotted line).
Analysis
All continuous measurements from both the AOD and normal cohorts were converted to binary format (diagnostic of AOD: yes, no). Average sensitivities, specificities, and positive and negative predictive values for each method were then calculated. An interrater reliability analysis using the kappa statistic was performed to determine the consistency among raters. The Cohen kappa was run to determine if there was agreement between the two neurosurgeons’ judgment on the six patients clinically diagnosed with AOD. A kappa value of 1 represented perfect agreement, a value of 0.75 to 1 represented an excellent agreement, a value of 0.4 to 0.75 represented fair to good agreement, and a value less than 0.4 was poor agreement.
Results
The average age of the patients who suffered AOD was 33.3 ± 10.1 years, and the average age of the normal cohort was 46.6 ± 16.5 years. Women accounted for 33.3% of the AOD patients and 20% of the control patients. A summary of the associated injuries, type of surgery and outcome, and follow-up of the patients with AOD is presented in Table 1. All patients were treated with occipitocervical fusion.
Summary of patients diagnosed with atlanto-occipital dissociation
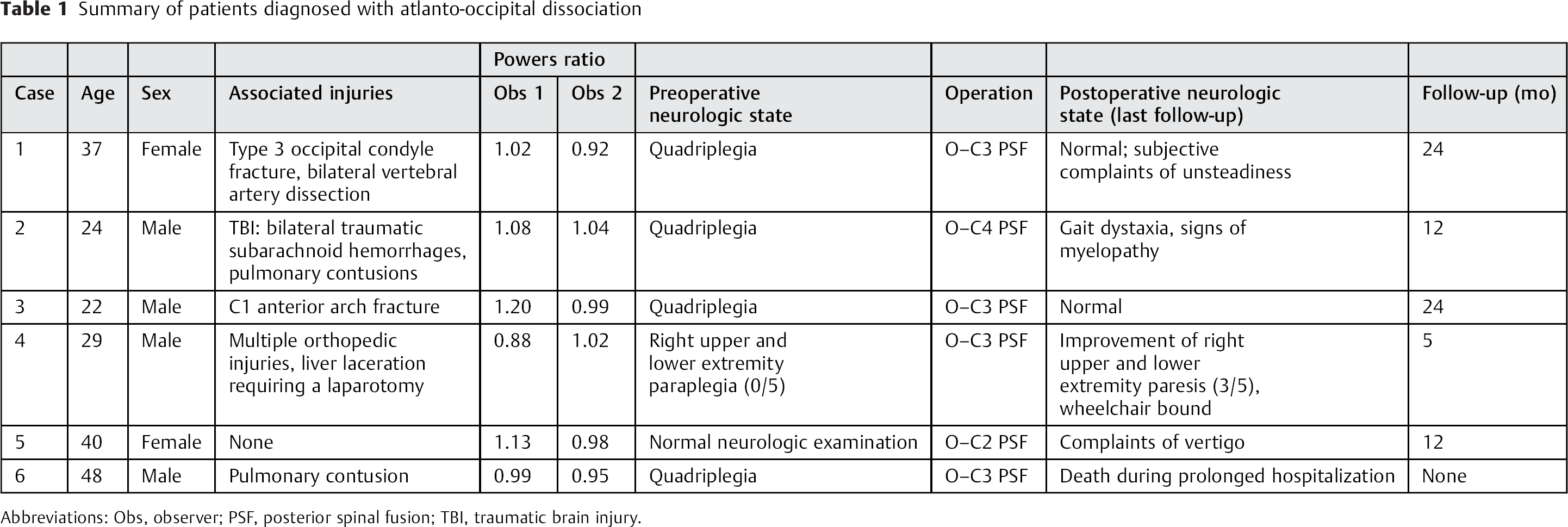
Abbreviations: Obs, observer; PSF, posterior spinal fusion; TBI, traumatic brain injury.
The sensitivity, specificity, and positive and negative predictive values of each method are summarized in Table 2. The kappa statistic for interrater reliability is summarized in Table 3. The average sensitivity for BDI, BAI, Lee X-lines, Power ratio, CCI, and revised CCI was 0.75, 0.33, 0.67, 0.50, 1.00, and 1.00, respectively. The average specificity was 1.00, 1.00, 0.50, 1.00, 0.94, and 1.00, respectively. The average positive predictive value was 1.00, 1.00, 0.25, 1.00, 0.80, and 1.00, respectively. The average negative predictive value was 0.96, 0.88, 0.89, 0.91, 1.00, and 1.00, respectively. The kappa statistic was 0.57, 0.25, 0.25, 0.20, 1.00, and 1.00, respectively. Compared with all other modalities, the modified CCI had the highest sensitivity, specificity, and positive and negative predictive values of 1.00. Perfect agreement between both observers was achieved with CCI and the revised CCI methods. All bilateral parasagittal CT constructions at the level of the occipital condyle/lateral mass of C1 joint of patients with AOD are presented in Fig. 3.
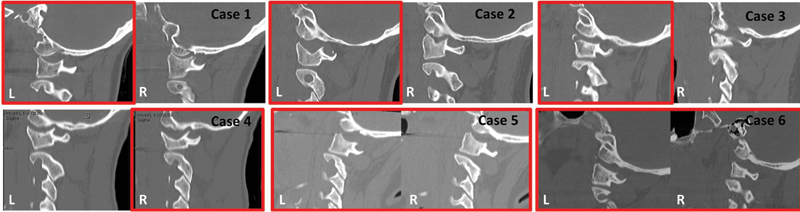
Occipitocervical dissociation. All six cases of occipitocervical dissociation at the level of the occipital condyle–C1 joint parasagittally on both sides. Unilateral or bilateral dislocation is present (red box).
Comparison between different criteria to diagnose atlanto-occipital dissociation
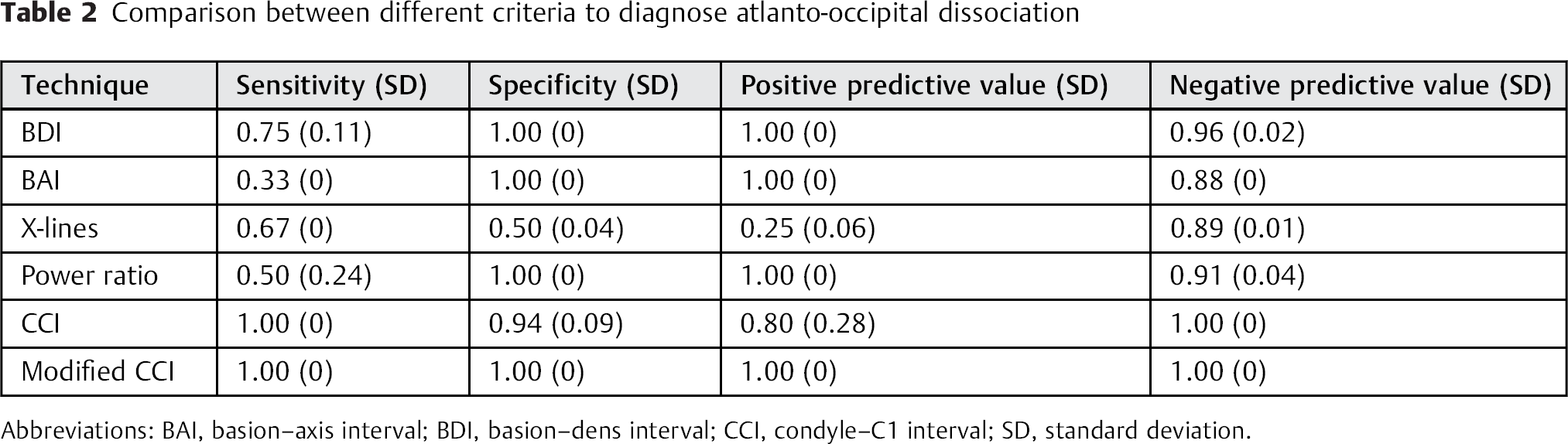
Abbreviations: BAI, basion–axis interval; BDI, basion–dens interval; CCI, condyle–C1 interval; SD, standard deviation.
Reliability of different criteria to diagnose atlanto-occipital dissociation
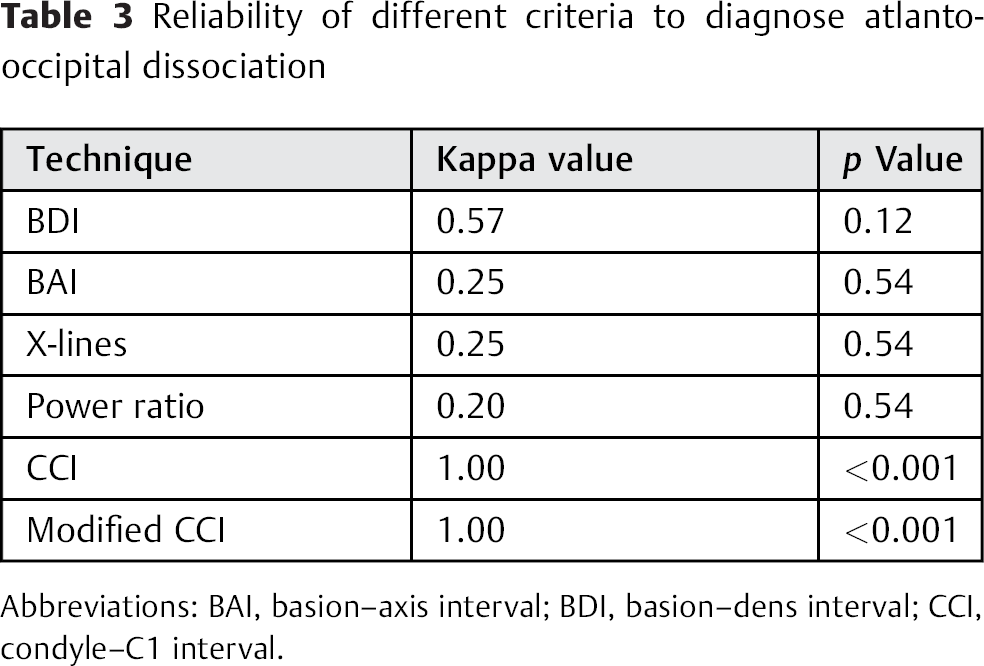
Abbreviations: BAI, basion–axis interval; BDI, basion–dens interval; CCI, condyle–C1 interval.
Discussion
The diagnosis of AOD is challenging, and hence multiple diagnostic criteria have been put forth with the intention of making an accurate diagnosis. Most of the original criteria are based on X-rays, and their utilization is oftentimes limited by the difficulty of recognizing abnormalities involving the upper cervical spine. 10 , 11 , 12 , 19 , 20 Recently, Pang et al analyzed the CTs of a cohort of pediatric cervical spine and determined that the average condyle C1 interval is 1.28 mm. 15 Following that, in 2013 Gire et al proposed a revised CCI and determined that unilateral dislocation or dissociation in the sagittal plane at the level of condyle C1 joint of 2.5 mm is sufficient to make an accurate diagnosis. 6 In their study, a cohort of 10 pediatric and adult patients with AOD were compared with 10 patients without AOD. Five observers analyzed the scans. They determined that the revised CCI had an average sensitivity and specificity of 1.0 and 0.84, respectively. Their interrater kappa value was 0.78, indicating excellent agreement. Compared with other techniques studied, the revised CCI was a highly sensitive and reliable criterion.
Our study is in agreement with that of Gire et al. 6 The CT scans of six patients with the diagnosis of AOD were compared with scans from a cohort of 30 patients without AOD. In comparison with BAI, BDI, X lines of Lee, the Powers ratio, and CCI > 2 mm methods, the revised CCI had 1.00 specificity, sensitivity, positive, and negative predictive values and had perfect agreement based on the analysis of two blinded neurosurgeons. Moreover, our study also showed that the lowest sensitivities were those for BAI and Powers ratio of 0.33 and 0.50, respectively, which is in agreement with Gire et al. 6 In their study, the lowest sensitivities were 0.26 for both BAI and Powers ratio. The X-lines of Lee showed the lowest specificity of 0.50, which is also in agreement with the Gire et al study of 0.38.
Achieving a rapid and a reliable diagnosis of AOD cannot be overemphasized, as missed diagnoses are associated with catastrophic outcomes. 21 Many of these patients’ neurologic examinations are often confounded by other associated intracranial injuries. The revised CCI technique offers a rapid method of diagnosing patients with AOD as only unilateral dissociation in the sagittal plane is sufficient to make the diagnosis. On the other hand, it should be noted that cases of purely ligamentous AOD have been described. 13 , 21 If a ligamentous injury is suspected, it should be identified with magnetic resonance image with short tau inversion recovery, which should be obtained once the patient is medically stable. 20
This study is one of few to compare CT findings in such a rare but catastrophic injury. The limitations of this study include the small number of patients with AOD, its retrospective nature, and the limited number of observers.
Conclusion
The revised CCI method is simple yet a sensitive and reliable technique for the diagnosis of patients with AOD.
Disclosures
Nader S. Dahdaleh: none
Ryan Khanna: none
Arnold H. Menezes: none
Zachary A. Smith: none
Stephanus V. Viljoen: Personal fees (Medtronic)
Tyler R. Koski: Consultant (Medtronic, Nuvasive, SpineWave); Stock ownership (Nuvasive); Honorarium (Depuy)
Patrick W. Hitchon: none
Brian J. Dlouhy: none