
Abstract
Study Design
Literature review and case report.
Objective
Review the existing literature and report the successful nonoperative management of a two-level craniocervical ligamentous distraction injury.
Methods
A PubMed and Medline review revealed only three limited reports involving the nonoperative management of patients with craniocervical distraction injury. This article reviews the existing literature and reports the case of a 27-year-old man who was involved in a motorcycle accident and sustained multiple systemic injuries and ligamentous distraction injuries to both occipitocervical joints and both C1–C2 joints. The patient's traumatic brain injury and bilateral pulmonary contusions precluded safe operative management of the two-level craniocervical distraction injury. Therefore, the patient was placed in a halo immobilization device.
Results
The literature remains unclear as to the specific indications for nonoperative management of ligamentous craniocervical injuries. Nonoperative management was associated with poor outcomes in the majority of reported patients. We report a patient who was managed for 6 months in a halo device. Posttreatment computed tomography and flexion–extension radiographs demonstrated stable occipitocervical and C1–C2 joints bilaterally. The patient reported minimal neck pain and had excellent functional outcome with a Neck Disability Index score of 2 points at 41 months postoperatively. He returned to preinjury level of employment without restriction.
Conclusions
Further study is needed to determine which craniocervical injuries may be managed successfully with nonoperative measures.
Introduction
Traumatic distraction injuries to the craniocervical junction are typically treated with occipitocervical fusion procedures. 1 , 2 , 3 High failure rates of nonoperative management have been reported. 4 The existing literature includes few reports of craniocervical injuries treated successfully with prolonged immobilization. 5 , 6 However, in most cases, significant follow-up of the patients and functional outcomes are not reported. We report the successful management of a unique two-level craniocervical distraction injury in a 27 year-old man who was treated with prolonged halo immobilization. To our knowledge, the successful nonoperative management of a two-level craniocervical dissociation injury has not been reported in the literature.
Methods
A PubMed and Medline search was conducted involving the nonoperative management of craniocervical distraction injury. This article reviews the existing literature and also reports the case of a 27-year-old man who was involved in a motorcycle accident and sustained multiple systemic injuries and ligamentous distraction injuries to both occipitocervical joints and both C1–C2 joints. The patient's traumatic brain injury and bilateral pulmonary contusions precluded safe operation of the two-level craniocervical distraction injury. Therefore, the patient was placed in a halo immobilization device.
Results
A PubMed and Medline search revealed only three limited reports involving the nonoperative management of patients with craniocervical distraction injury. Nonoperative management was associated with poor outcomes in the majority of the few reported patients. We report a patient who was managed for 6 months in a halo device. Posttreatment computed tomography (CT) scan and ultimate follow-up flexion–extension and traction radiographs demonstrated stable occipitocervical and C1–C2 joints bilaterally. The patient reported minimal neck pain and an excellent functional outcome with a Neck Disability Index score of 2 points at 41 months postoperatively. He returned to preinjury level of employment without restriction.
Case Report
A 27-year-old man was riding a motorcycle at a high rate of speed, lost control, and collided with a large tree. The helmet he was wearing sustained significant damage. Per the report, he was ambulating at the scene and moving all four extremities. He then lost consciousness and was intubated by emergency services technicians in the field. The patient was transferred to a level 1 trauma center where he was diagnosed with a large intraventricular hemorrhage with both frontal and temporal lobe brain contusions. He also sustained bilateral severe pulmonary contusions with multiple bilateral displaced rib fractures.
The initial lateral cervical spine image was suspicious for both widening of the occipitocervical and C1–C2 joints (Fig. 1). On physical examination, the patient was noted to be moving all four extremities spontaneously with normal muscle tone and strength. Sensation was also noted to be normal in all four extremities. Deep tendon reflexes were normoactive throughout.

Initial lateral cervical spine image is suspicious for both widening of the occipitocervical and C1–C2 joints.
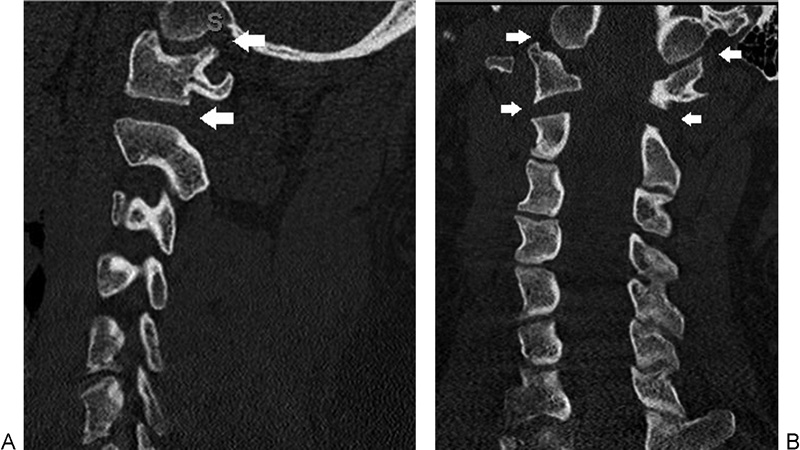
The CT scan of the cervical spine revealed evidence of two-level bilateral craniocervical distraction injuries with diastasis of the occipitocervical and C1–C2 joints bilaterally (Fig. 2A, B). Magnetic resonance imaging (MRI) of the cervical spine demonstrated severe edema and distraction injuries to both the occipitocervical and C1–C2 bilateral joints (Fig. 3A, B).
(
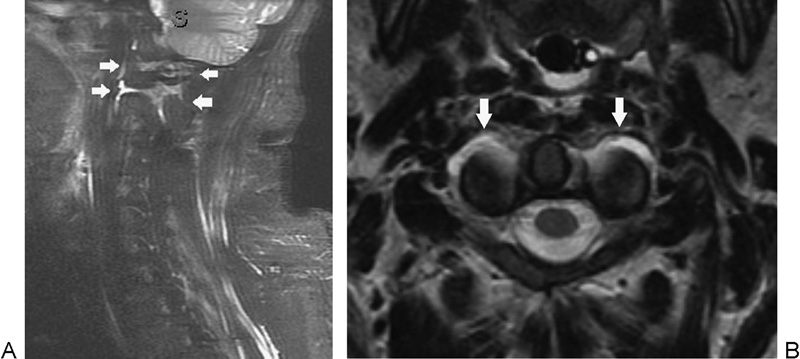
(A, B) Magnetic resonance imaging of the cervical spine demonstrated severe edema and distraction injuries to both the occipitocervical and C1–C2 bilateral joints.
The patient was deemed too medically unstable to undergo operative stabilization of his complex craniocervical distraction injuries. On postinjury day 2 in the intensive care unit, a halo vest immobilization device was placed. The initial halo radiographs demonstrated continued widening of both the occipitocervical and C1–C2 joints (Fig. 4). The patient remained hospitalized and medically unstable for several weeks after the injury date. The recommendations from the intensive care team were to not proceed with complex cervical surgery due the patient's poor pulmonary and cerebral status. The patient was maintained in his halo throughout his hospital course.

Initial halo lateral radiograph demonstrated continued widening of both the occipitocervical and C1–C2 joints.
In the months following the injury, the patient demonstrated improved pulmonary and cerebral function. At 8 weeks postinjury, the decision was made to continue halo immobilization as the primary method of spinal injury treatment. He was discharged home at 10 weeks after his injury. Spine clinic outpatient follow-up radiographs documented neutral alignment of the craniocervical junction.
At 6 months postinjury, the halo was removed. A CT scan showed maintained neutral alignment and reduction of the diastasis in all four involved joints (Fig. 5). At 41 months postinjury, flexion–extension and traction radiographs showed normal cervical motion with maintained stability (Fig. 6A, B, C). The patient had returned to unrestricted work as an emergency medical technician. He reported very minimal activity-related neck pain. At the time of ultimate follow-up, his neck disability index score was 2, indicating excellent functional outcome, and he reported an analog pain score of 0.
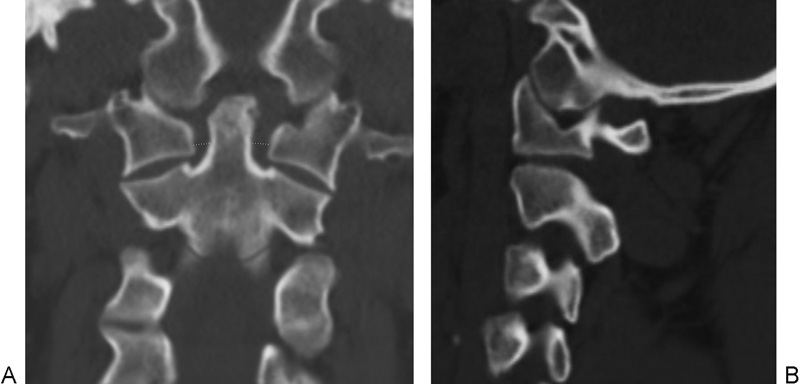
(A, B) Six-month follow-up computed tomography scan after halo removal showing neutral alignment and reduction of the diastasis in all four involved joints.
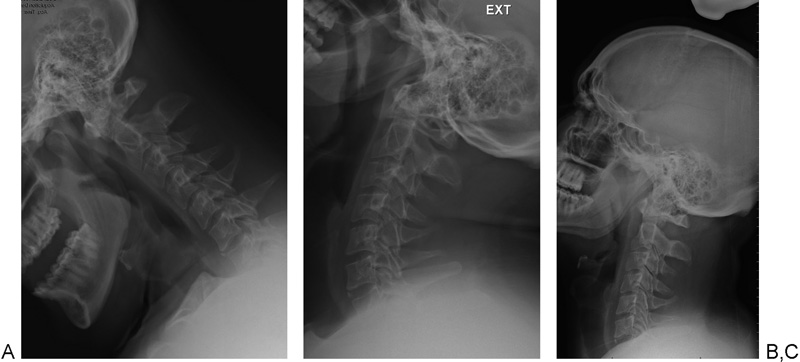
(A, B) Flexion–extension radiographs at 41-month follow-up showing normal cervical range of motion with maintained craniocervical stability. (C) Craniocervical traction lateral radiograph showing maintained stability and alignment of the upper cervical spine and occipitocervical junction.
Discussion
Distraction injuries to the craniocervical junction are the result of very high-energy trauma with powerful distractive forces. These injuries have high reported rates of fatality and severe neurologic dysfunction. 7 , 8 It has been estimated that traumatic atlanto-occipital injury may account for up to 20% of fatal high-speed blunt trauma accidents. 4 The most frequently injured ligaments in occipitocervical distraction injuries are the tectorial membrane and the alar ligaments, which are the most important stabilizing ligaments of the craniocervical junction. 2 , 3 Various reports conclude that early injury recognition and prompt stabilization are the most important factors toward successful craniocervical injury management. 9 , 10 , 11 The patient in our case report most likely sustained an incomplete rupture or stretching of the main stabilizers of the occipitocervical junction including the alar ligaments, ligamentum transversum atlantis, ligamentum flavum, tectorial membrane, and joint capsules.
Atlanto-occipital dislocation (AOD) injuries may be difficult to diagnose. The diagnosis of AOD is often missed on spine plain radiographs and is difficult to detect on the initial lateral image in our patient (Fig. 1). Early additional imaging of the craniovertebral junction with either CT or MRI is recommended in patients suspected of having craniocervical injury. Gire et al have demonstrated improved accuracy in occipitocervical injury diagnosis using the combination of CT and MRI imaging to confirm occipitocervical joint abnormalities. 12 Pang et al performed a CT scan-based anatomical evaluation of the occipitocervical joints and determined a nonpathologic normal mean occipitocervical joint interval of 1.28 mm. The authors found no cases of normal OC joint distance greater than 2.5 mm. 13 The two separate levels of injury occurring at both occipitocervical and C1–C2 joint levels are confirmed in our patient by the presence of significant abnormalities on both CT and MRI and distraction distance greater than 4 mm in both sets of joints (Figs. 2, 3). Unfortunately, the clear identification of occipitocervical ligament rupture versus ligament stretching remains difficult on static MRI and CT.
Early injury recognition and injury management is important. Reis et al reported the largest series of traumatic craniocervical dissociation survivors, which included 48 consecutive adult patients. 14 Craniocervical dissociation was identified on initial cervical spine imaging in 26 patients (84%). The remaining 5 patients (16%) were diagnosed by cervical spine MRI. Twenty-three patients (74.2%) were diagnosed within 24 hours of presentation, 4 (22.6%) were diagnosed between 24 and 48 hours, and 1 (3.2%) experienced a delay of greater than 48 hours. Four patients died during their hospital course.
Operative stabilization of the craniocervical junction is the most common treatment described in the literature. 1 , 15 , 16 Prior to performing fusion surgery, it is important for the surgeon to determine the prognosis of the patients who sustain traumatic craniocervical injury as many of these injuries are associated with other multisystem severe injuries that may preclude survival. Chaput et al suggested that AOD is a potentially survivable injury. 17 The authors suggested that a significant neurologic injury, a high degree of initial distraction, and more severe associated injuries would decrease the likelihood of survival. They evaluated 14 patients and attempted to describe the occipitocervical injury pattern in a statistically meaningful way. Patient mortality was associated with the presence of a complete neurologic deficit (p = 0.0047), a high basion-dens interval (>16 mm, p = 0.015), and a high injury severity score (p = 0.0373).
There is a plethora of literature describing the successful operative management of craniocervical injuries. 1 , 2 , 4 Good outcomes have been reported in numerous studies with a comprehensive plan that consists of accurate and timely diagnosis and stabilization of the craniocervical junction. 5 , 14 , 15
What remains unclear with respect to craniocervical distraction injuries is the distinction between the patients who should be managed with or without stabilization surgery. Bellabarba et al proposed a three-stage classification system for craniocervical junction injuries. 1 The authors indicated that stage 1 injuries, which are often mild injuries to only one of the occipitocervical joints, may be managed nonoperatively. They postulated that in some craniocervical injuries, sufficient ligamentous integrity may be present to maintain craniocervical stability. It was suggested that these lower-grade craniocervical injuries will have less than 2 mm of joint distraction on manual distraction testing using lateral fluoroscopy. Although this mild form of craniocervical injury was described, the successful nonoperative management of stage 1 injury was not demonstrated by the authors. The patient in our case report exceeds the distraction criteria as described by Bellabarba et al for mild craniocervical distraction injury as the static initial CT and MRI images demonstrate greater than 2 mm distraction of both occipitocervical and C1–C2 joints. Although this study demonstrates that advanced imaging is beneficial in making the diagnosis of craniocervical distraction injuries, the classification system proposed may not account for differentiating complete ligament rupture and stretching of the ligaments alone, which may be difficult due to the limitations of static imaging in the acute injury setting.
The existing literature lacks significant discussion of successful nonoperative management of injuries to the craniocervical junction. The indications for nonoperative management remain unclear, and the functional outcomes of nonoperative treatment have not been adequately described. The patient we report was initially indicated for occipitocervical fusion surgery and underwent nonoperative management due to other systemic injuries that precluded surgery.
There are few existing reports of nonoperative management of craniocervical distraction injuries. Much of this literature demonstrates the high failure rates with conservative management. Govender et al reported four patients who had sustained a traumatic dislocation of the atlanto-occipital joint. 5 The diagnosis was initially missed in two patients. Only one of the patients, who was neurologically intact, was treated nonoperatively with a halo body jacket. The remaining three recovered neurologically after an occipitocervical fusion. The nonoperatively treated patient had a rotatory-type subluxation injury of the occipitocervical joint. The functional outcome for the nonoperative patient in this series was not adequately reported.
In another small series, Ghatan et al described three children, age 1 to 32 months, who presented with craniocervical junction injuries. 6 Variable neurologic findings were observed at presentation (ranging from cranial nerve deficits to severe quadriparesis). All three children were treated with prolonged immobilization and recovered with minimal to no neurologic deficit. Although children younger than 3 years of age represent a distinct subpopulation of patients at particular risk for high cervical and craniovertebral injuries, there are very few descriptions of survivors of severe craniocervical trauma among the very young, and scarce data exists regarding management after initial emergency stabilization.
A recent systematic review by Theodore et al identified 13 patients initially treated with external immobilization alone: 4 worsened transiently and 3 were unstable after 6 to 22 weeks of immobilization, 4 and 7 of the 13 patients either deteriorated neurologically or failed to achieve craniocervical stability. Only 5 patients with AOD described in the literature were successfully treated with external immobilization alone (1 type I, 2 type II, 2 other type dislocations). The authors suggested that because 7 of 12 (58%) patients managed with external immobilization either deteriorated neurologically or failed to achieve craniocervical stability without surgical internal fixation and fusion, the treatment of AOD with external immobilization alone should be considered with extreme caution. In this literature meta-analysis, the failure to treat AOD with surgery resulted in worsening in 7 of 13 patients (54%) with most patients deteriorating neurologically. Although the use of external immobilization for AOD was often associated with late instability, several patients achieved stability without operative management. The authors also suggested that the use of both CT and MRI for differentiation of partial and complete ligament tears from stretch injuries may be useful in identifying a subgroup of patients in whom craniocervical stability might be achieved with external immobilization alone.
Bellabarba et al, in a retrospective evaluation of institutional databases, reviewed medical records and original images obtained in 17 consecutive surviving patients with craniocervical distraction injury. 1 The diagnosis of craniocervical distraction injury was frequently delayed, and the delay was associated with an increased likelihood of neurologic deterioration. All the patients were treated with craniocervical fusion surgery. The authors concluded that early diagnosis and spinal stabilization protected against worsening spinal cord injury.
It is apparent from the existing craniocervical literature that operative management of these highly unstable injuries leads to improved patient outcomes. Although we report a patient with a unique two-level distraction injury who was successfully managed with prolonged halo immobilization, the indications and role of nonoperative treatment still remain undefined. It is very likely that our reported patient sustained incomplete rupture of the main occipitocervical stabilizing structures and thus successful treatment was achieved with nonoperative management of the injury. Long-term follow-up of both surgically and halo-managed patients will improve our understanding of the ideal treatment for this unusual and potentially lethal injury.
Conclusions
The literature remains unclear as to which craniocervical injuries may be managed successfully with nonoperative measures and further study is needed. Only three limited reports have been published to date describing the nonoperative management of patients with craniocervical distraction injury, and most patients had poor outcomes. In addition, although advanced imaging with MRI and CT has been shown to be helpful in diagnosing these injuries, the reliability of these diagnostic modalities to identify the severity of the ligamentous injury may be misleading in the acute setting. We describe successful nonoperative management of a unique two-level craniocervical ligamentous distraction injury using a halo device in a 27-year-old man who had multiple systemic injuries that precluded safe operative management. Excellent functional and radiographic outcome was maintained at 41 months posttreatment. Further study is recommended.
Disclosures
Nathan B. Kaplan, none
Christine Molinari, none
Robert W. Molinari, none
So why publish a case, which defies all published odds?
Evidence-Based Spine-Care Journal (EBSJ) has selected this single-patient case report for the very reason that it contradicts the current conventional wisdom that patients with craniocervical dissociation past pediatric age are preferably treated with open reduction and internal fixation with arthrodesis of the injury zone. The case as described involves a polytraumatized patient with severe head injury and chest trauma in addition to an unstable appearing ligamentous craniocervical junction injury with a vertical atlanto-occipital and a vertical atlanto-axial disruption. Although we are not given details of the head injury (location of the bleed, presence or absence of displaced skull fracture, intracranial pressure, burr holes, and craniectomy sites) and the chest injury (rib and or sternal fractures, acute respiratory distress syndrome, hemato- or pneumothorax), none of these injuries make for a particularly good argument in favor of halo vest immobilization and recumbent immobilization-based treatment. Although the authors emphasize that their patient was not cleared for any spine surgery, one could make the counterargument how the patient could be cleared for prolonged recumbent immobilization treatment in light of this serious injury constellation? From a biomechanical standpoint, this treatment choice is also less than desirable as well because a halo vest serves more of a distraction function along the craniocervical junction and is not suitable to exert a compression function in this region. 1 This injury as shown is clearly a distractive injury and as such not really amenable to halo vest reduction.
The final healing result is certainly convincing. So how did the authors succeed in getting this distractive, purely ligamentous injury of the craniocervical junction to heal so well—without apparent instability or subluxation and without visible heterotopic bone formation? The exact reasons were unclear to the reviewers at EBSJ-Global Spine Journal (GSJ) but several factors were offered:
Perhaps the severity of the head trauma immobilized the patient effectively for the critical first weeks to allow for healing. Having the patient's head slightly elevated in the intensive care unit bed might have reduced the head back down onto the neck, allowing the halo vest to do what it is designed to do by preventing translation in the sagittal plane.
The head trauma may have induced osseous heterotopic bone formation (which we do not see on the provided final radiographs and CT scan) or excessive scar formation that provided such reassuring stability.
Perhaps the ligamentous injury was indeed just a severe sprain and not a complete disruption, a circumstance that a surgeon-conducted traction test such as promoted by the Harborview group would have revealed. 2
An incomplete craniocervical ligament injury may have left several key ligaments. For instance, it appears that the patient retained an intact transverse atlantal ligament—an important anchoring structure and part of the cruciform ligament complex at the center of the craniocervical junction. 3 Perhaps other key ligaments such as the tectorial membrane, the atlanto-occipital facet capsules, and the often overlooked but mechanically relevant transverse occipital ligament were also structurally intact to allow for sufficient mechanical healing of the craniocervical osteoligamentous complex? 4 No doubt the patient was fortunate to have recovered so well from this serious injury constellation with what appears to be a very favorable result, but how we could predict such a favorable healing result in the first place remains somewhat unpredictable.
What conclusions can we draw from a single case report, which defies the vast majority of published reports on this subject?
Of course, this single case report should not call into question the advancements of the past two decades in terms of diagnosis and emergent as well as surgical treatment for survivors of traumatically disrupted craniocervical junctions. As presented in the preceding article, these published outcomes collectively are impressive and have provided a clear improvement over the past. Perhaps this article by Kaplan et al can inspire us to reflect on how we remain quite unrefined in our attempts at identifying and properly grading ligamentous injuries of the spine—despite MRI and increasingly accurate CTs.
Finally, this article can also remind us that conventional wisdom is a powerful force—one most often desirable in its benefits, but also a force that can lead to dogma where plurality of approaches and some variances still can and perhaps should play an important role. In the right circumstances, and if done well, nonoperative care, as in this example, can still play an important part in spine trauma care. Sadly, in everyday practices nonoperative spine trauma care has become increasingly obsolete for more serious injuries because it is more arduous and difficult to apply compared with surgery, it may have more uncertain outcomes, and it is commonly more cost-intensive due to longer inpatient stays. Nonoperative care in most well-developed countries is rapidly becoming a lost art as newer resident generations are well trained in surgical details but—for instance—have never applied a halo vest.
EBSJ/GSJ welcomes the comments of its readership on this subject.