
Abstract
Study Design
Systematic Review and Meta-analysis
Objective
The purpose of this study is to synthesize recommendations for perioperative medical management of RA patients and quantify outcomes after spine surgery when compared to patients without RA.
Methods
A search of available literature on patients with RA and spine surgery was performed. Studies were included if they provided a direct comparison of outcomes between patients undergoing spine surgery with or without RA diagnosis. Meta-analysis was performed on operative time, estimated blood loss, hospital length of stay, overall complications, implant-related complications, reoperation, infection, pseudarthrosis, and adjacent segment disease.
Results
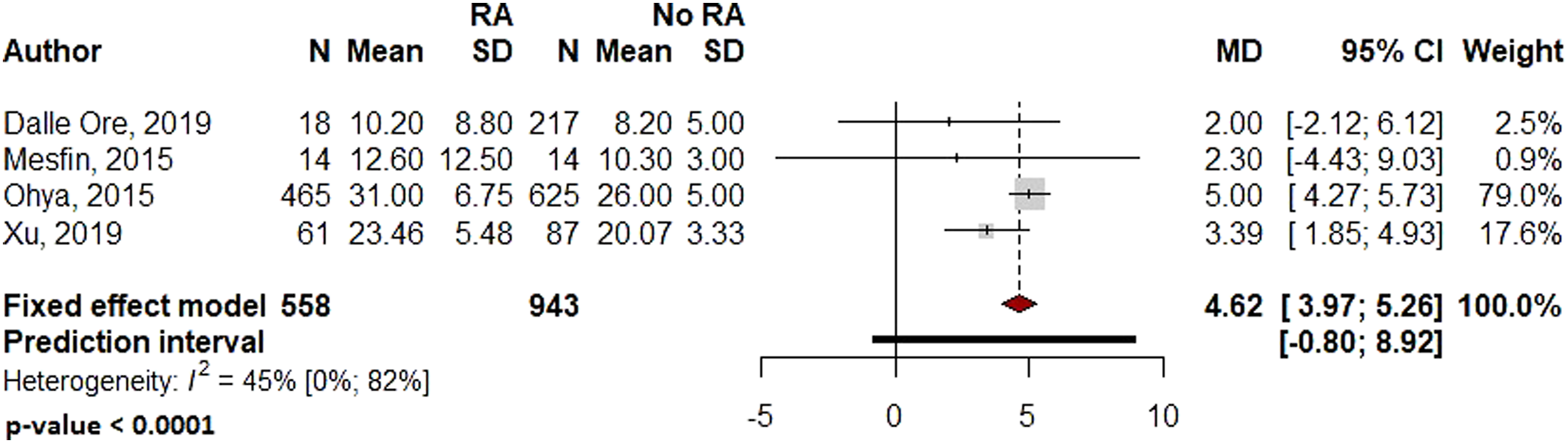
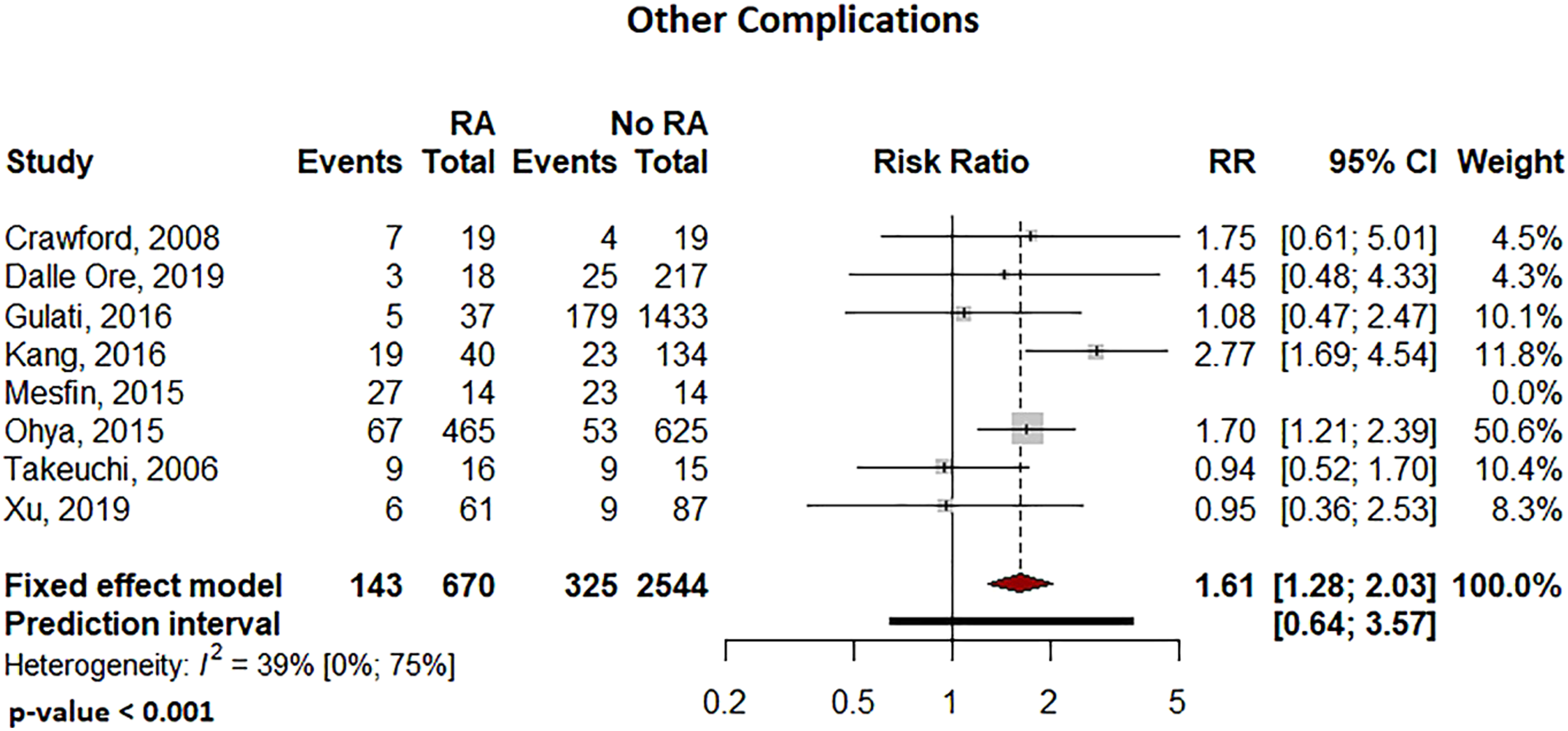
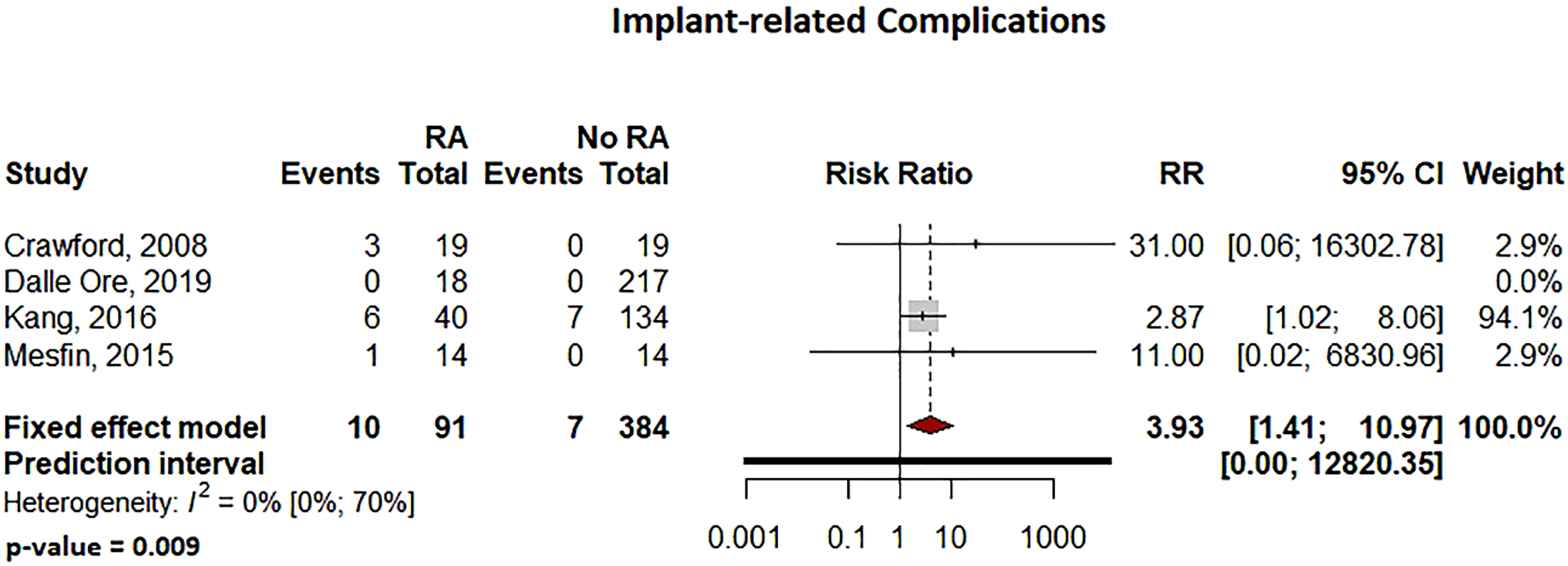
Included in the analysis were 9 studies with 703 patients with RA undergoing spine surgery and 2569 patients without RA. In RA patients compared to non-RA patients undergoing spine surgery, the relative risk of infection was 2.29 times higher (P = .036), overall complications 1.61 times higher (P < .0001), implant-related complications 3.93 times higher (P = .009), and risk of reoperation 2.45 times higher (P < .0001). Hospital length of stay was 4.6 days longer in RA patients (P < .0001).
Conclusions
Treatment of spinal pathology in patients with RA carries an increased risk of infection and implant-related complications. Spine-specific guidelines for perioperative management of antirheumatic medication deserve further exploration. All RA patients should be perioperatively co-managed by a rheumatologist. This review helps identify risk profiles in RA specific to spine surgery and may guide future studies seeking to medically optimize RA patients perioperatively.
Keywords
Introduction
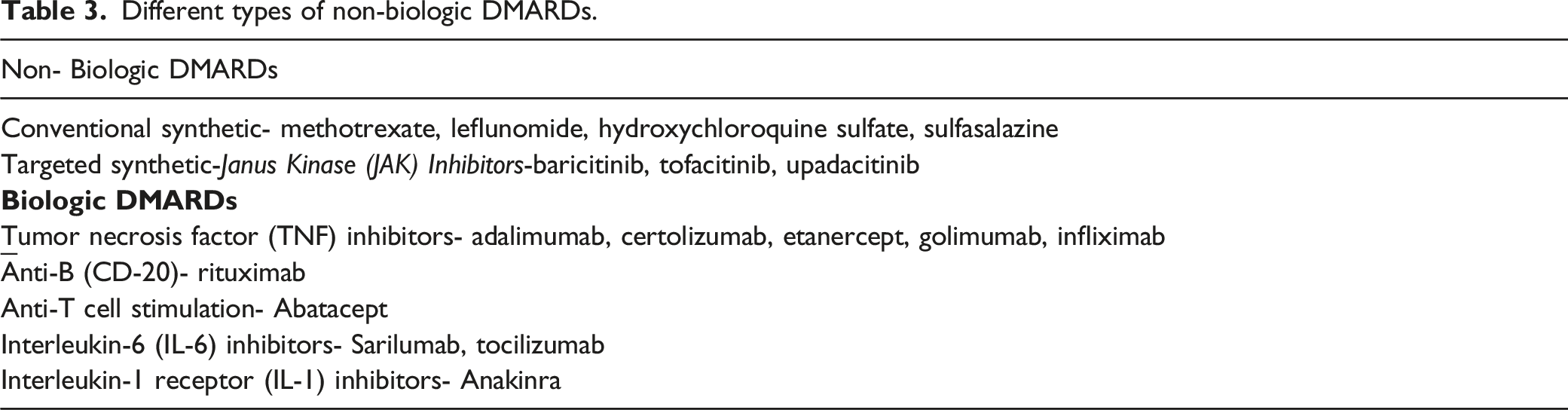
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease affecting 1–2% of the global population.1,2 Initial treatment is medical management with nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroids, and others, 2 including novel disease modifying antirheumatic drugs (DMARDs) and biologics that directly affect the host autoimmune response. Although DMARDs and biologics have the potential to slow the progression of rheumatoid arthritis and protect the joints from permanent damage,3,4 infectious and potentially other side effects have been attributed to use of DMARDs.5,6
Many patients with RA will require surgical treatment for advanced disease even with a proper use of medication regimen,3,7,8 though this may be decreasing over time. 9 As the spine is a frequent location for RA involvement, surgical intervention may be indicated in patients with myelopathy, radiculopathy, instability, or deformity.7,8,10-12The systemic inflammatory nature of this autoimmune disease as well as the subsequent medical treatments have been implicated in increasing complication rates in orthopedic and other surgery. Numerous studies have shown that RA may increase the risk of developing a variety of postoperative complications, including wound infection and instrument failure, ultimately necessitating revision after initial spine surgery,3-7 though other reports presented no appreciable differences in surgical outcomes or complications.8,9
Prior studies have suggested the perioperative continuation of some DMARDs, biologics, and other antirheumatic medications may increase infection rates after surgery;15-19 however, current evidence is varied based on type of medication, power of available studies to detect low probability events such as infection or other complications, and sometimes conflicting results.15,16,18-22 Additional concern exists for precipitating RA disease exacerbation while off medication. 20 Although this question is studied extensively in elective hip and knee arthroplasty and other elective orthopedic procedures,15,18,20,23,24 there is a paucity of literature on spine surgery.
Considering these knowledge gaps, the objectives of this study were to synthesize recommendations for perioperative medical management of RA patients and quantify outcomes and complications after spine surgery when compared to patients without RA.
Methods
Data Sources and Search Strategy
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and checklists were used for this systematic review. 10 A certified, experienced librarian carried out an extensive search of electronic databases in PubMed, Ovid/MEDLINE, Cochrane, and Scopus for published articles for all available years. A search strategy including keywords for “spine” or “spinal” or rheumatoid or (rheumatic adj arthritis) or “inflammatory arthritis” “lumbar” or “lumbosacral” “occipital-cervical” or atlantoaxial or “atlanto-axial” or “occipitoatlantoaxial” or “occipito-atlantoaxial” or “craniovertebral junction” or “subluxation” or “vertebral” or “intervertebral” or “disc” or “discs” or “sacral” or “sacrum” or “fusion” or “fused” or “fusing” or “fixation” or “decompression’ or “arthrodesis” or “reconstruct.” Two authors (C.O. and Y.Y) screened the studies for eligibility after a list of articles was obtained. The senior author (M.B.) was consulted in final decision-making for any discrepancies.
Eligibility Criteria
The following inclusion criteria were used for eligibility; (i) studies that included patients with a diagnosis of rheumatoid arthritis undergoing spine surgery compared to a control group of patients without RA undergoing spine surgery. (ii) Studies that reported any complications or made an assessment regarding complications for patients with RA directly compared to patients without RA and (iii) studies in English language and with available full text. Reviews and studies that did not present specific information about spine surgery were excluded from our analysis. In addition; (i) studies that included patients with diagnosis of rheumatoid arthritis prior to spine surgery, (ii) studies that provided details regarding antirheumatic medication use prior to surgery (name, dose, timing) and (iii) studies that reported any complications or made an assessment regarding complications if no complications present were included for a separate systematic review on perioperative medication use.
Data Extraction and Processing
The following information was collected for included studies; (i) information on author name and study year, (ii) average age, gender, and follow-up (iii) number of patients specific to RA and Non-RA cohorts, (iv) location, type and specific levels of the spine surgery, (v) operative parameters including blood loss and operative time, (vi) any complications seen in patients undergoing spine surgery including wound infection, (vii) reoperation at the same level, and (viii) diagnosis of adjacent segment disease. For the systematic review of perioperative medication use, information on (i) author name and study year, (ii) study design, (iii) number of patients (total and spine-specific numbers if other procedures are included), (iv) location and specific levels of the spine surgery, (v) name and the dose of the medication used in rheumatoid arthritis treatment, (vi) whether the medication was stopped and restarted perioperatively and (vii) any complications seen in patients undergoing spine surgery were collected.
Statistical Analysis
Mean differences (MDs) were used to summarize continuous variables and the categorical outcomes were presented using risk ratios (RRs) with 95% confidence intervals (CI). The outcomes of interest were compared between patients undergoing spine surgery with and without RA diagnosis. Heterogeneity was represented with Higgins I-square (I2). A random effects model was used when meta-analyses indicated greater than 50% heterogeneity. Pooled estimates and effect sizes were represented by forest plots. Statistical analyses were conducted using R 4.0.5. (R Foundation for Statistical Computing). P values <.05 were considered significant.
Level of Evidence
Levels of evidence were assessed by use of the Oxford Centre for Evidence-Based Medicine Levels of Evidence. 11 It was assessed by 2 authors in parallel with arbitration by a third author in cases of disagreement.
Results
Search Results and Study Characteristics
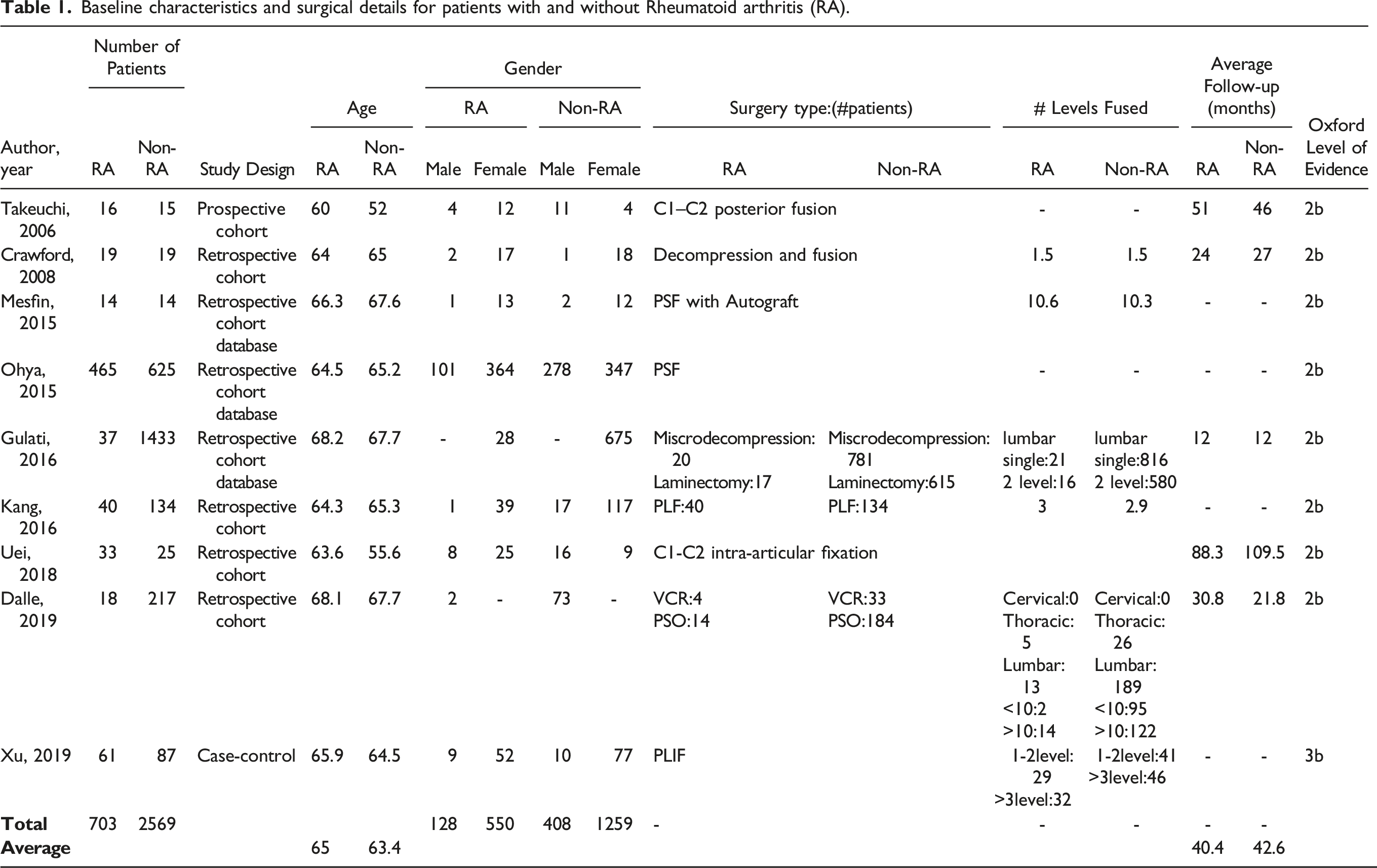
An initial search of the electronic databases revealed 2016 studies which were filtered further to 391 relevant articles. From these, 9 full-text articles were included in the qualitative assessment. PRISMA flowchart for included studies. Baseline characteristics and surgical details for patients with and without Rheumatoid arthritis (RA).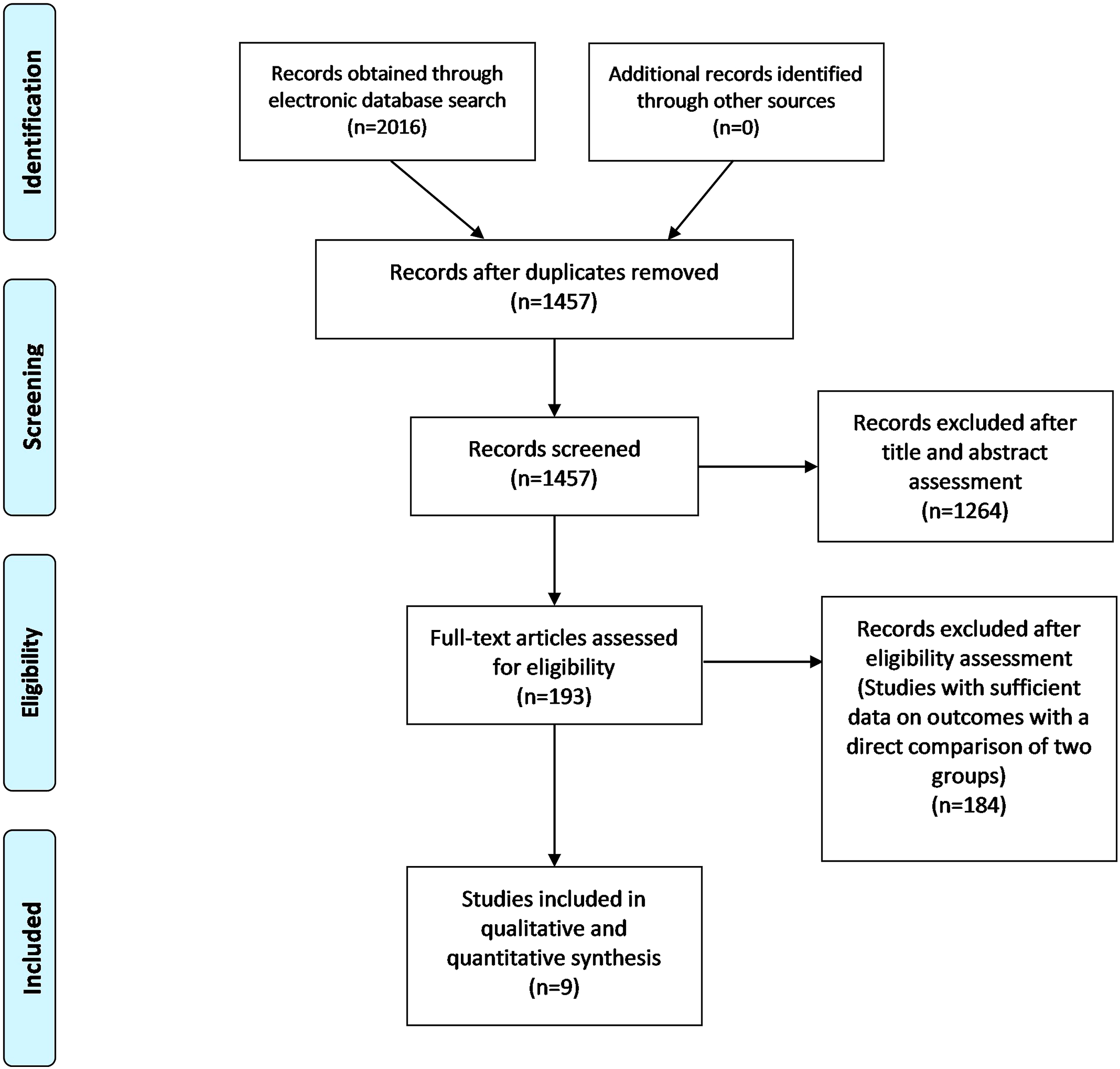
Perioperative Details
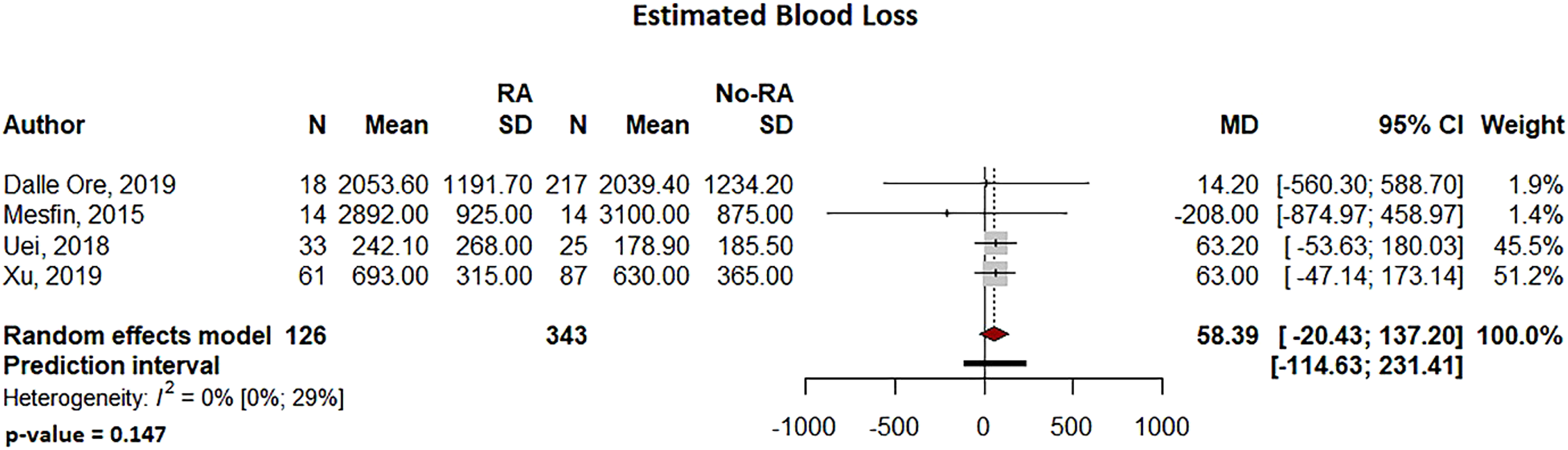
In the RA and non-RA groups, operative time (95% CI: −28.78 to 17.5, P = .633, Figure 2) and estimated blood loss (95% CI: −20.43 to 137.30, P = .147, Figure 3) were not significantly different Forest plot comparing operative time for patients undergoing spine surgery with and without RA. Forest plot comparing the estimated blood loss for patients undergoing spine surgery with and without RA. Forest plot comparing the hospital length of stay for patients undergoing spine surgery with and without RA.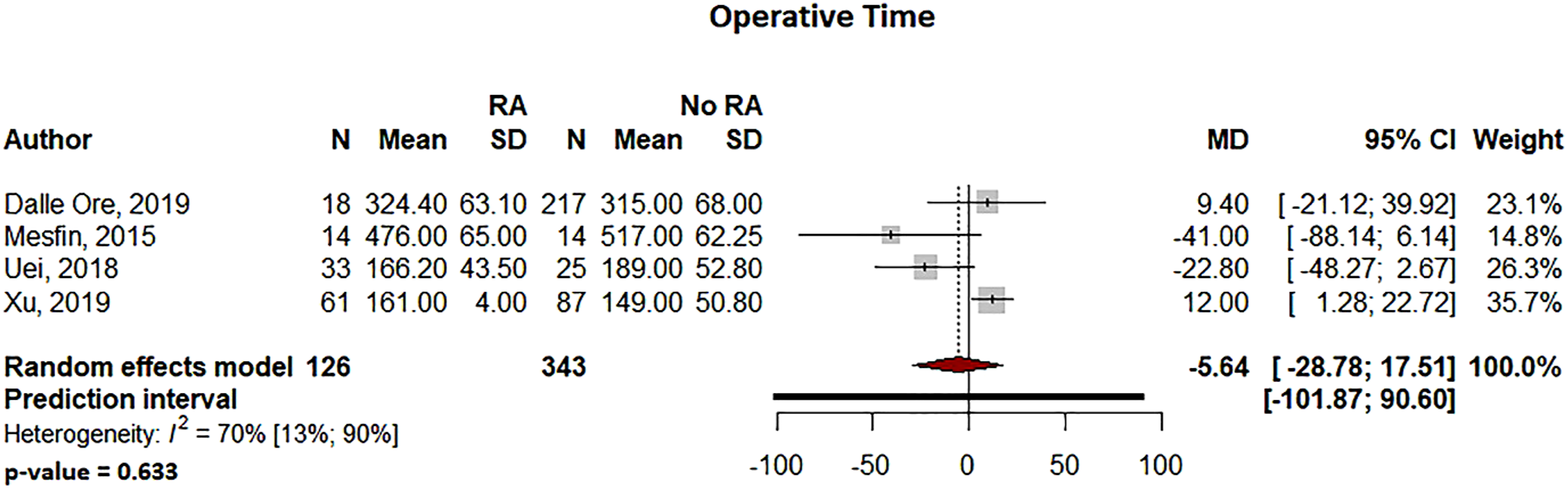
Infection and Complication Rates
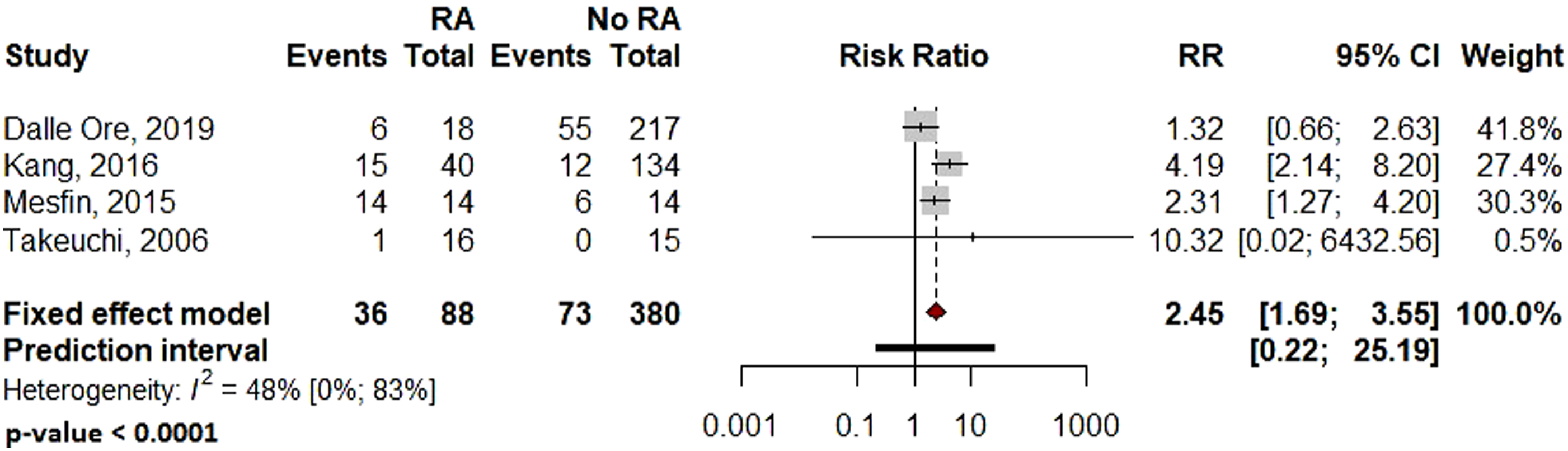
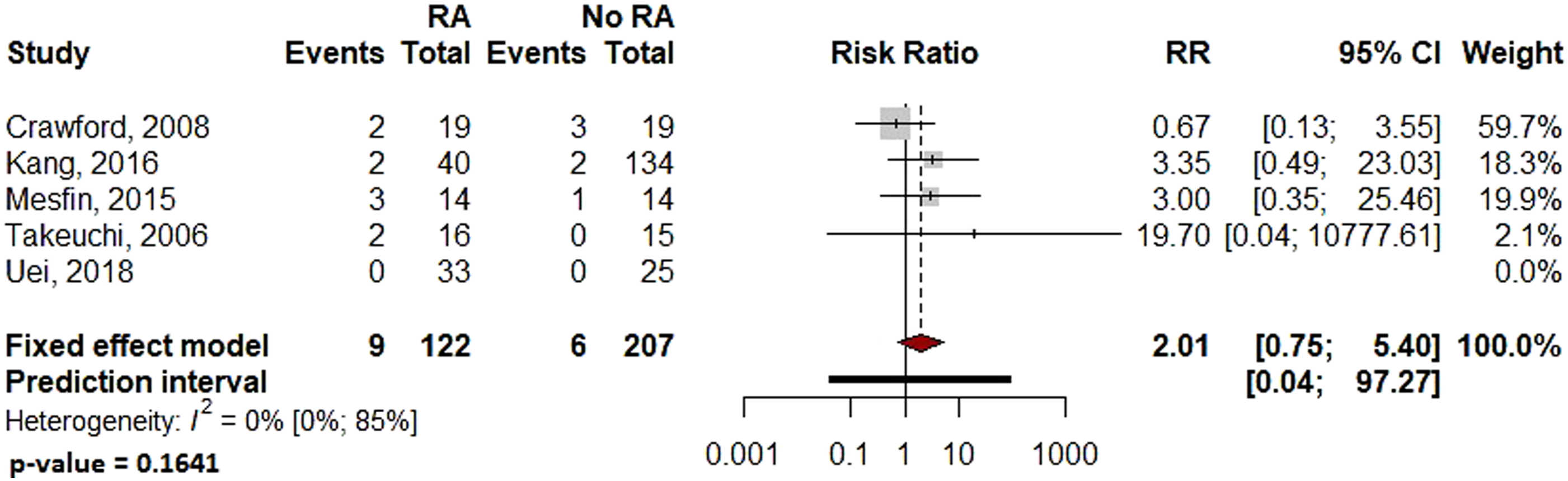
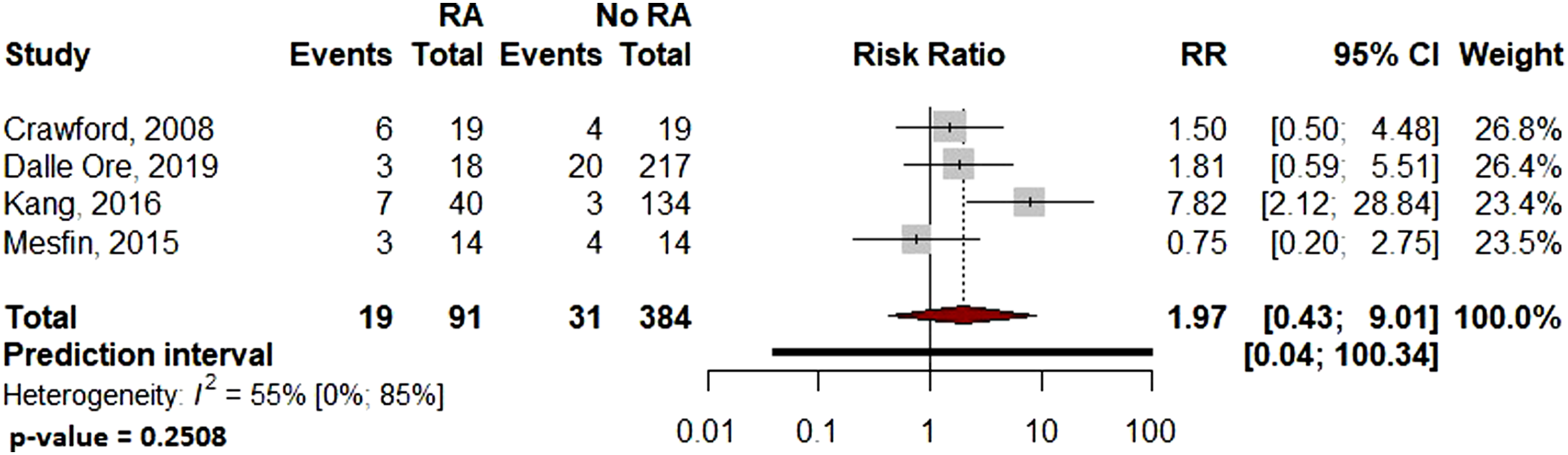
Pooled analysis showed significantly more surgical site infections in the RA group than the Non-RA group, with a relative risk of 2.29 (95% CI: 1.08–4.84, P = .036 Forest plot comparing the surgical site related infection rates for patients undergoing spine surgery with and without RA. Forest plot comparing the overall complications for patients undergoing spine surgery with and without RA. Forest plot comparing the implant-related complication rates for patients undergoing spine surgery with and without RA. Forest plot comparing the reoperation rates for patients undergoing spine surgery with and without RA. Forest plot comparing pseudoarthrosis for patients undergoing spine surgery with and without RA. Forest plot comparing diagnosis of adjacent segment disease for patients undergoing spine surgery with and without RA.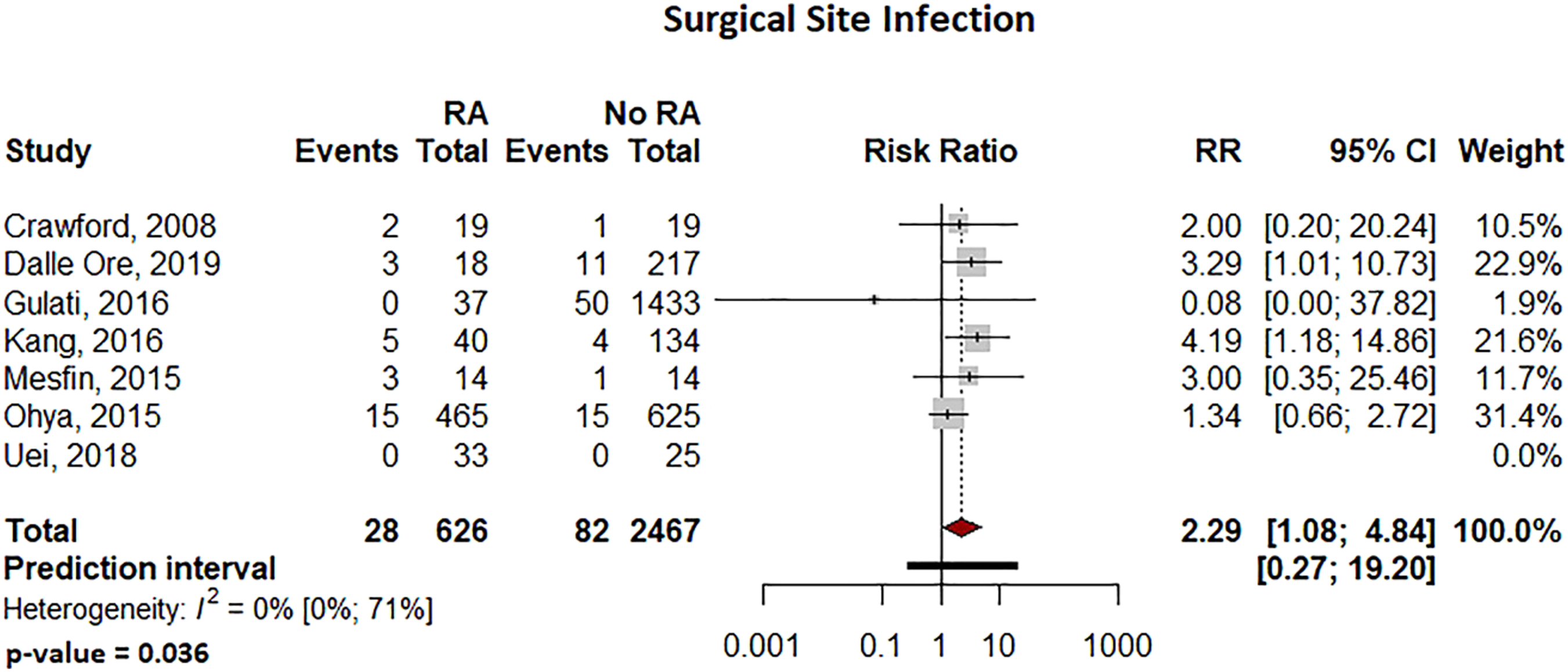
Due to the varied nature or absence of reporting in the included studies, several variables of interest could not be reliably examined or compared, including: distinction between deep and superficial infection, the distinction between medical and surgical complications, and patient reported outcome measures.
Perioperative Antirheumatic Medication Management
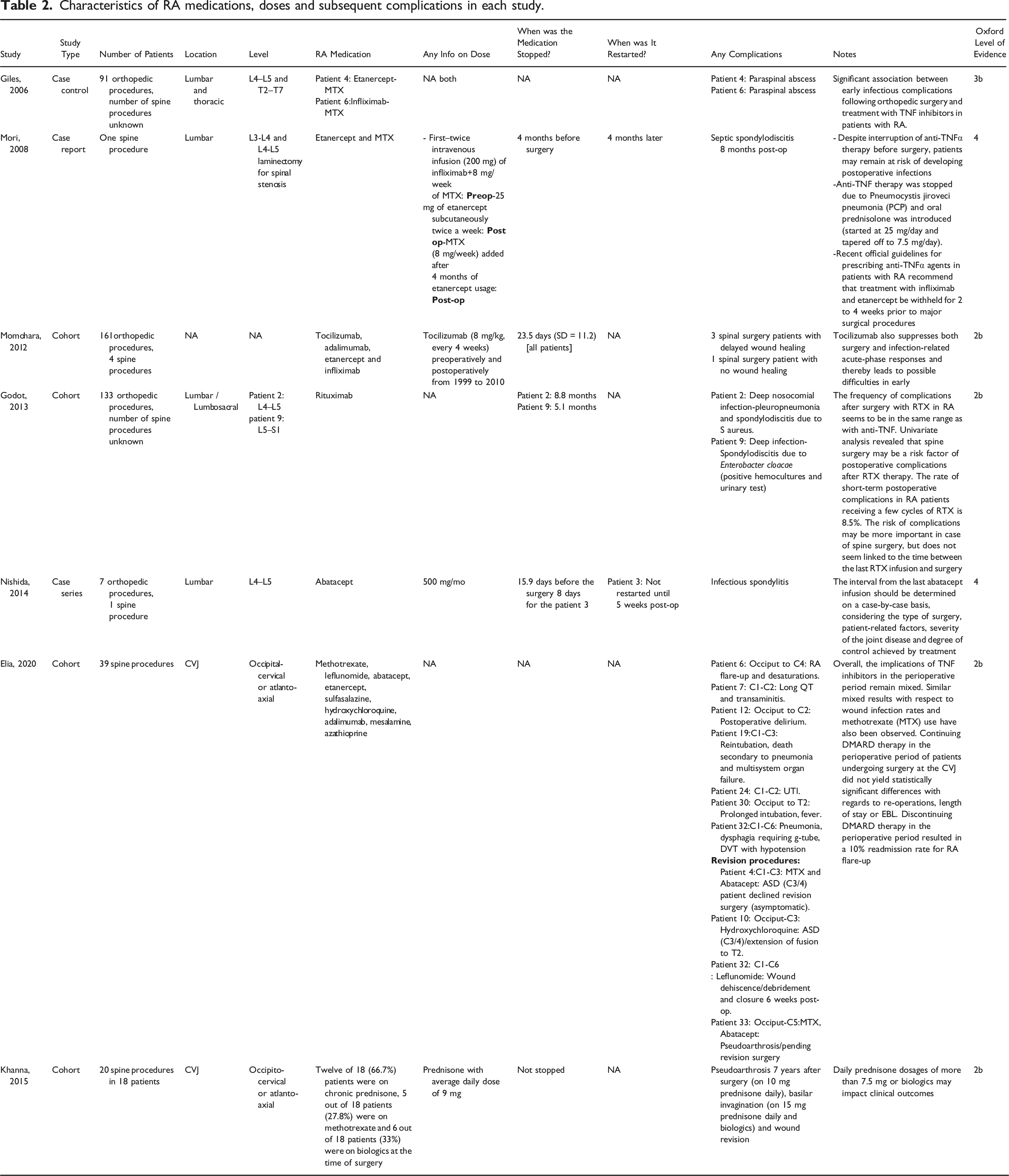
Characteristics of RA medications, doses and subsequent complications in each study.
Guidelines and Recommendations From Surgical Literature
Few studies specifically investigate perioperative RA medication management for patients undergoing spine surgery, though there are some investigations and clinical guidelines for orthopedic surgery or other surgical fields in general. In 2011, Suzuki et al. conducted a survey of orthopedic surgeons on perioperative management of RA medications and have reported the general practice patterns regarding the use of methotrexate, tacrolimus, infliximab, etanercept, adalimumab and tocilizumab perioperatively for all procedures. 24 Time to stop these medications ranges from 9.7 days (methotrexate) to 26.4 days (infliximab). Regarding to time to restart, the earliest medications to be readministered were methotrexate (10.4 days) and tacrolimus (10.5), and the latest medication to be readministered was infliximab (24.8 days). 24
Different types of non-biologic DMARDs.
Discussion
The primary purpose of this review was to evaluate the differences in peri- and postoperative outcomes with RA diagnosis among patients undergoing spine surgery and guide management of the medical treatments for rheumatoid arthritis in the perioperative period for spine surgery. The included studies compared RA and non-RA patients with respect to clinical outcomes, though the variable reporting of these outcomes did limit the quantitative analysis. The qualitative review of medication management revealed additional variability.
Spine surgery for patients with RA is indicated for myelopathy, radiculopathy, instability, or deformity.26-30 Existing literature has shown differences in surgical outcomes for patients previously diagnosed with RA, often affected by the complication profile seen in RA.3,6,31 Studies reporting on spine-specific outcomes in RA patients have shown some mixed results. In a retrospective review included in this study, Crawford et al. found no statistically significant difference in RA versus non-RA patients in complications or outcomes after lumbar fusion. 8 Dalle Ore et al. reviewed major thoracolumbar deformity correction operations and compared patients with and without RA, finding no differences in overall surgical complications but an increase in wound healing complications with the use of prednisone. 12 In a similar patient population of adult scoliosis patients, Mesfin et al. noted increased complication and reoperation rates of RA compared to non-RA patients. 3 Koyama et al. retrospectively reviewed 47 RA patients undergoing spinal fusion surgery with concomitant use of biologic and non-biologic DMARDs, finding an overall 15% surgical site infection, though not correlated with the use of methotrexate, prednisone, biologic DMARDs or other operative factors. 32 Kang in a retrospective matched cohort comparison of RA and non-RA posterolateral lumbar fusion patients found higher complication rates, including infection, nonunion, implant failure, and overall reoperation in those patients with RA. 5 Horowitz performed a database review of Medicare patients with RA undergoing 1- or 2-level ACDF, finding increased medical, surgical, and infectious complications when compared to those without RA, although information on the perioperative medical treatment of these patients was unavailable. 6 Valuable details regarding perioperative medical management, such as the dosing or timing of weaning or cessation, however, were not available in any of the above studies. While some studies have shown higher rates of infection in RA patients, details of perioperative medical management are often not well reported, and the causative factors remain unclear.
Zhang et al. in a previous systematic review assessed the effect of RA on infection and complications after spine surgery, finding significantly greater rates of complications in the RA cohort. 33 However, the review included 6 studies 2 of which included information from databases and pose a risk of overlapping patients. Moreover, only complications and infections were included in the study. The present review included 9 independent studies and assessed a broader spectrum of parameters, including estimated blood loss, operative time, and implant-related complications in addition to the rates of overall complications and infection.
The increased risk of postoperative complications, including infections and wound breakdown, previously has been attributed to increased comorbidities in patients undergoing spine surgery. Several studies have found increased postoperative complication rates in patients with comorbidities including BMI, smoking, and diabetes, while others have demonstrated that increased operative times are associated with worse postoperative outcomes.34-36 In this review, there was no significant difference in operative time between RA and non-RA patients and overall comorbid burden was unable to be compared.
In this review, implant-related complications were significantly associated with the RA group. A multicenter prospective study by Soroceanu assessed 245 patients on the incidence, risk factors, and impact of implanted related complications and quality of life measures after adult spinal deformity correction, identified nearly a third of their cohorts experienced this complication with over half of them needing reoperation after 2 years. 37 Seki investigated the differences in rates of adjacent to segment disease (ASD) and clinical outcomes in RA patients undergoing lumbar decompression. Results from this study showed a significantly increased rate of ASD in RA patients undergoing lumbar fusion. 28
Existing literature provides some direct and indirect clues to the safety of continuing certain medications in and around the time of spine surgery. Unfortunately, some studies have produced contradictory results. There is evidence that perioperative continuation of prednisone,12,38,39 hydroxychloroquine, 38 leflunomide, 40 and DMARDs18,19,41,42 increase the risk of infection; however, other studies have shown no increase of infection with prednisone,22,32 methotrexate 38 or those same or different DMARDs.32,42,43
Due to long-term corticosteroid use, many patients with RA may also carry increased risk of osteoporosis, present in up to 30% in some populations. 44 Theoretical risks also exist for decreased healing capacity of bone due to chronic inflammation or prednisone use. 45 Vertebral fractures and implant-related issues stemming from osteoporosis are noted in several studies.5,46,47 Excluding infection or wound problems, other complications appear similar in some studies8,12 but increased in RA populations in others.3,5 Regarding clinical outcomes, most studies show that spinal surgery provides predictable improvements in outcome measures for patients with RA, similar to those patients without RA diagnosis.5,8,12 Progression of rheumatic pathology in the spine is noted in several studies, which may affect longer-term outcomes,5,30 including those specific to spine.40,41
Newer antirheumatic medications appear to be decreasing the burden of spinal disease over time26,48; however, medical treatments both old and new are not without risk. Terashima reported on a 10-year prospective cohort study enrolling RA patients without initial cervical instability, noting that corticosteroid use correlated with development of more severe cervical pathology. 27 Despite the high quality and long-term follow-up of this study, it is unknown whether prednisone treatment indicates a more severe disease burden or if treatment is associated with this poorer outcome.
Limitations
Several limitations exist in this systematic review. First, included studies were retrospective in nature, as a result, the influence of selection and recall biases cannot be fully withheld. Second, there was significant heterogeneity across studies. The types of operations were different, and the types of reported complications also varied greatly across studies; therefore, understanding the details surrounding individual complications was not possible. Significant heterogeneity also existed between studies for the reporting of operative parameters like EBL and length of surgery for the respective operative types. Finally, several studies reported on preoperative use of anti-RA medications, however, this was inconsistent across studies. Moreover, frequency of use and specific medications or dosing was often not reported.
Conclusion
Rheumatologic disease continues to afflict patients with spinal pathology, and patients often require surgical treatment despite recent advances in medication regimens
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.