
Abstract
Study Design:
Literature review.
Objectives:
Metastatic disease affecting the craniovertebral junction (CVJ) only accounts for 0.5% of all spine metastases. The management of these disease processes is complex, which involves multimodality radiological studies and various surgical approaches. We aimed to review the available evidence and summarize the findings in this review.
Methods:
The authors conducted search of PubMed and Google Scholar with the following search terms: metastasis, craniovertebral junction (CVJ), occipitocervical, approaches, stability, and radiotherapy. Articles were reviewed by the authors and determined for inclusion based on relevance and level of evidence.
Results:
The majority of relevant research reviewed composed of literature reviews of particular aspects regarding metastatic disease affecting the craniovertebral junction, including diagnosis, surgical approach, and radiotherapy.
Conclusions:
Prompt evaluation of rotational neck pain with or without occipital neuralgia may reveal early metastatic disease within a stable CVJ. Magnetic resonance imaging appears to be the gold standard imaging modality in detecting this pathology, with nuclear bone scan playing a role in distinguishing benign and malignant processes. Unfortunately, no level 1 evidence exists for use of either radiotherapy or surgery in these cases; however, from the available literature, spinal instability and evidence of progressive neurology are relative indications for operative intervention.
Introduction
The skeletal system is the third most common site of metastasis in the body, with spine metastasis the most common within this system, 1,2 and of these the majority are found within the thoracic spine, with up to 15% of cases found with the cervical spine. 3,4 The definition of metastasis is the spread of a disease-producing agency (as cancer cells) from the initial or primary site of disease to another part of the body. 5 Common primary lesions included thyroid, lung, breast, renal, and prostate carcinoma, and the literature would suggest breast carcinoma being the most common primary site, attributing to just over a third of all cases. 6 Metastatic disease affecting the craniovertebral junction (CVJ) is less common and only accounts for 0.5% of all spine metastases. 7 The cervical spine itself can be divided anatomically into 3 regions: the occipitocervical region or craniocervical junction, the subaxial region, and the cervicothoracic junction. The occipitocervical spine encompasses the occiput to C2, and CVJ tumors are defined by anatomic involvement of the occipital condyles and/or atlantoaxial spine. The median survival rate of patients with spinal metastasis is 10 months. 8 In this context, the main goals of the management of these patients is local tumor control, reducing analgesic requirement, salvage or improve neurological function, and maintain stability of the junction operatively if necessary. We present a case treated in our spinal unit as well as the available literature on this rare clinical scenario. The authors conducted search of PubMed and Google Scholar with the following search terms: metastasis, craniovertebral junction (CVJ), occipitocervical, approaches, stability, and radiotherapy. Articles were reviewed by the authors and determined for inclusion based on relevance to topic of review and level of evidence. Institutional review board approval was not sought for this study, as patients were not recruited for the study.
Methods
To construct this review article, the authors conducted search of PubMed, Google Scholar, and the Cochrane database, with the following search terms: metastasis, craniovertebral junction (CVJ), occipitocervical, approaches, stability, and radiotherapy. The combined number of articles in the completed search was 165.
The inclusion criteria were the following, Articles pertaining to clinical presentation of pathology Articles pertaining to management of pathology Surgical approaches to CVJ An article in English
The exclusion criteria were the following: Case reports Article pertaining to subaxial metastatic disease of cervical spine Not an article in English
Ultimately through his process, 44 articles were included in this review.
Clinical Presentation and Investigations
The most common presenting complaint in this cohort of patients is cervical spine pain, more specifically mechanical pain and occipital neuralgia, which presents as headaches in the suboccipital region and retroauricular areas, 9 It has been noted by Bilsky et al 10 that rotational pain is present in 90% of patients with CVJ involvement. Of note, myelopathy is an uncommon presenting complaint, and it is only present in 0% to 22% of cases. 11 Sixty years of age is the mean age of presentation of patients with upper cervical spine metastasis. 12 The first imaging modality typically used to evaluate neck pain is a plain radiograph of the cervical spine, to assess the alignment. It is not sensitive in revealing metastatic lesions in bone as over half of the patients will have normal findings on the radiograph. 13 Computed tomography (CT) is useful in this setting, first, in quantifying the volume of lytic bone related to the metastatic tumor, and second, characterizing suboccipital keel, which is important for preoperative planning. 12 The gold standard imaging modality in characterizing cervical spine tumors is magnetic resonance imaging (MRI), for both soft tissue and bone tumors. 12 Nuclear medicine can be employed to help distinguish between begin and metastatic tumors, which is particularly useful if the MRI findings are equivocal. Laufer et al 14 have shown that benign and malignant pathologies can be differentiated by using 18FDG positron emission tomography scans. Lesions with standardized uptake values generated by this scan of over 2 warrant further investigation for a metastatic source, and those with a SUV under could be followed for advancement with serial MRIs.
CT-guided biopsy has been utilized to derive tissue from the CVJ but are considered technically challenging, with transoral biopsy routes avoided due to seeding concerns. Typically, the other metastatic lesions are more amenable to biopsy as a case with a solitary metastasis to the cervical spine is rare. 15 Knowledge of the histology of the tumor is important as it can prompt preoperative embolization and reduces potential intraoperative bleeding. Candidate histologies typically reserved for this treatment include metastasis originating from renal cell carcinoma, thyroid, and hepatocellular carcinoma respectively. 15
Decision Making: Radiation or Surgery
Bilsky et al 10 preformed a retrospective review of a prospectively maintained spine database. Thirty-three patients were identified from the database that had metastatic tumor involving the atlantoaxial spine. Of these 25 underwent external beam radiation therapy (EBRT) and were selected based on normal or near-normal alignment with radiosensitive tumors. Eight patients underwent operative intervention with indications including atlantoaxial displacement more than 5 mm or angulation exceeding 11° with displacement more than 3.5 mm, and persistent pain after nonoperative therapy. The difference in median survival rate between the groups in this study has been attributed to selection bias related to disease burden and medical fitness to undergo operative intervention. The median survival rate for the group undergoing operative intervention was 16 months compared with 5 months for receiving EBRT alone. Stereotactic radiosurgery (SRS) can achieve high-energy radiation to isolated lesions in the vertebral body and it has shown favorable results when compared with EBRT in cervical spinal metastatic disease, not uniquely located at the CVJ. The local control rates appear to be significantly higher. 16 -20 It has been shown in 9 patients with metastatic disease to CVJ that SRS is a feasible option, if patients are selected with similar criteria employed by Bilsky et al. 10 Tuchman et al 20 showed a median survival of 4 months with none of this cohort requiring subsequent surgery. In the pursuit of evidence for decision making in cervical spine with metastatic disease, Fehlings et al 21 preformed a literature review. They found no level 1 evidence, but general guidelines for clinical management. With reference to the CVJ, metastatic disease involving the CVJ positively influences the decision to surgically stabilize the spine, with the posterior approach being favored, with radiation therapy selected for stable cervical spines. Azad et al 22 preformed a retrospective review of 25 patients with a mean SINS (Spinal Instability Neoplastic Score) of 7.3, with metastatic disease affecting the CVJ. In this cohort, the most common primary tumors were breast and non–small cell carcinoma. All patient in this cohort received SRS, with no tumor determined to be unstable based on the SINS, and no patient treated with either radiotherapy or surgery prior to SRS. In this cohort only 2 patients subsequently required post-SRS surgery to stabilize the cervical spine.
Determining Stability of CVJ and Importance of Vascular Anatomy
In determining spinal stability, the Denis 3-column system has been employed, with involvement of 2 columns indicating instability. 23 In recent times, the SINS has been validated with a sensitivity rate of 96% and specificity of 80%. It derives a score form of 6 components: location, the presence of pain, radiographic alignment, posterolateral involvement of spinal elements, degree of vertebral body collapse, and bone lesion morphology. 24
Embarking on any surgical approach in this anatomical region warrants careful consideration of vascular anatomy. Vertebral artery injury is catastrophic iatrogenic complication of cervical spine surgery, as it may cause cerebrovascular accidents. Gluf et al 25 retrospectively reviewed 191 consecutive patients who underwent atlantoaxial transarticular screw fixation, for a spectrum of pathology affecting the CVJ. In this series, 5 patients suffered vertebral artery injury. In a similar retrospective study, Wright et al 26 concluded that the overall risk of vertebral artery injury was 4.1%, with risk of neurological sequelae 0.2%, during C1 and C2 transarticular screw placement. Peng et al 27 conducted a literature review of the factors related to vertebral injury. Pertaining to anterior cervical approaches, lateral dissection puts the vertebral artery at most risk, with the authors suggesting constant reference to the midline prudent. With the posterior approach, safe screw placement is critical to avoid vertebral artery injury, with preoperative imaging of vascular structure, either by CT angiogram or MRI, is important in a considered surgical approach. Variability in the anatomy of the vertebral artery can be described as both extraosseous and intraosseous. Extraosseous anatomical anomalies of the vertebral artery include fenestration and persistent first intersegmental artery. With fenestration, the vertebral artery gives 2 branches following its exit from the C2 transverse foramen, with one branch entering the C1 foramen and the second entering the spinal canal between C1 and C2. In the case of the persistent first intersegmental artery the vertebral artery enters the posterior arch of C1, from the C2 transverse foramen directly. Yamazaki et al 28 conducted a retrospective study looking at 100 consecutive patients who underwent CVJ instrumentation surgery and had vertebral arteries 3-dimensional computed tomographic angiography (3D CTA) preformed preoperatively to establish the existence of potential anatomical anomalies. They report a rate of 10% extraosseous anomalies, 2% were fenestrated and 8% were persistent first intersegmental artery, which were more common in patients with atlantoaxial subluxation and congenital pathology of the CVJ. Anomaly of intraosseous vertebral artery was noted in 31% of cases (see Figures 1 and 2).
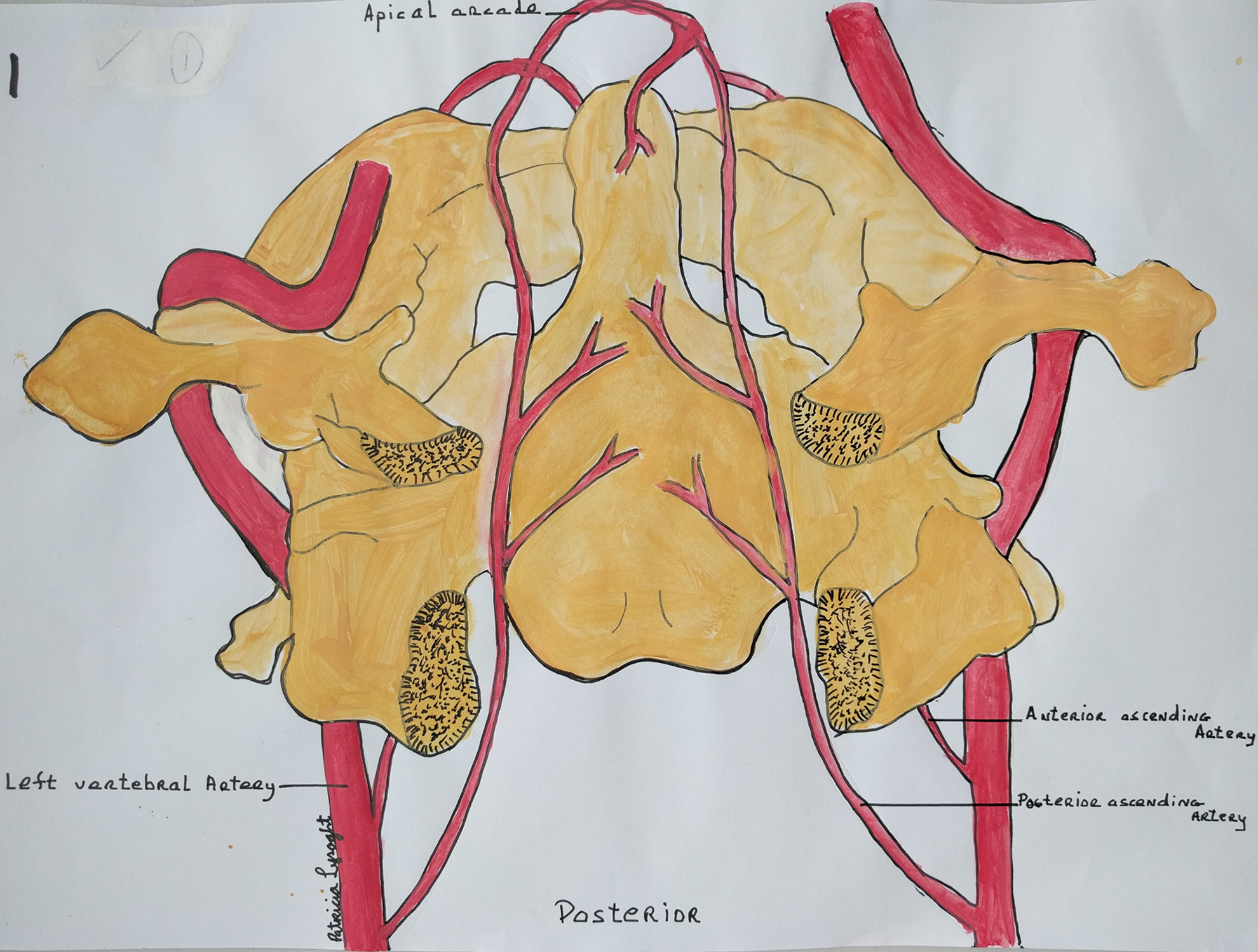
Posterior view of Atlas (C1) and Axis (C2) with related vascular structures.
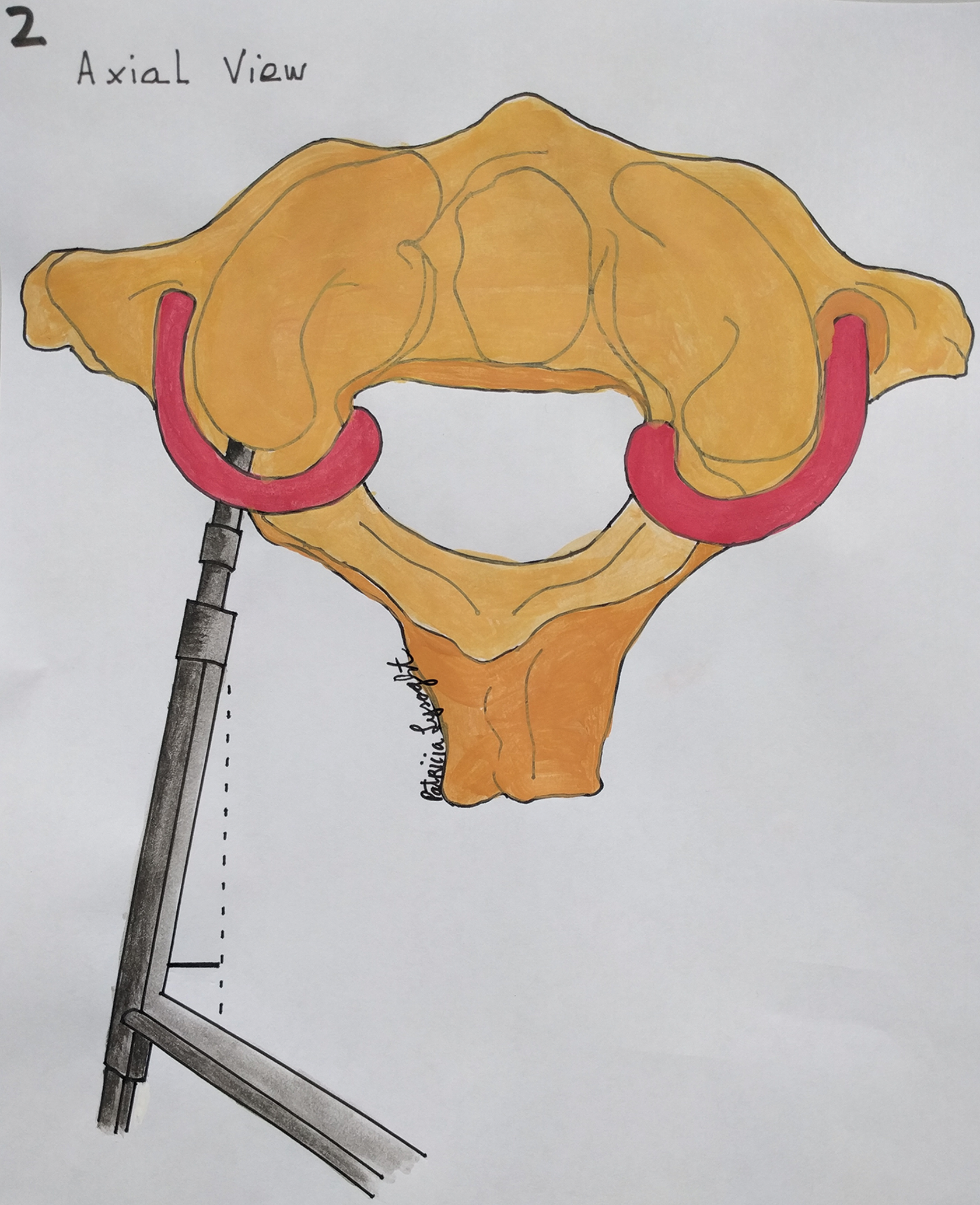
Axial view of (C1) displaying proximity of pedicel screw placement to vertebral artery.
Indications for Surgery
In determining the degree of surgery required for a given patient with metastatic disease of the CVJ, the modified Tokuhashi score can prove helpful. 24 The score has 6 components encompassing performance status, neurological status, and burden of metastatic disease. With a low score on the modified Tokuhashi, palliative surgery or radiotherapy can be considered. Of note vertebroplasty has been employed successfully in pathologic cervical compression fractures of the upper cervical spine. 29,30 Ultimately, the risk and benefit of an operative intervention should be discussed with each patient prior to any potential surgery.
Surgical Approaches
Once the decision to proceed with surgery has been reached, the approach to the metastatic lesion at the CVJ must be considered, including the stability of the CVJ and the expected degree of bony resection, Studies have shown that resection of 50% or more of the occipital condyle produces instability. 31,32 All approaches to the CVJ demand characterization of the vertebral arteries preoperatively, and vertebral artery angiograms and duplexes are commonly requested. Intraoperative monitoring of sensory evoked potentials, motor function, and cranial nerve function may be useful in selected cases. 33,34 As Fehlings et al 21 have discussed, the posterior approach appears to be the most frequently selected approach. This allows access to the posterior elements of the CVJ and is extensile to allow for access for instrumentation. Other approaches include transoral and posterior lateral.
The Transoral Approach 35
A major goal of this approach is the correction of irreducible anterior compression at the cervicomedullary junction. 36,37 Of importance in this approach is the management of dental hygiene as to reduce potential sources of infection due to dental caries. In terms of positioning the patient, it is typically preformed with the patient awake to determine any alterations in neurological status. The patient is placed supine with a horseshoe support to help hold the head in extension, with fiberoptic intubation typically elected in this scenario. This approach allows an exposure of 2 cm laterally and bilateral from midline from the clivus to the C3 body. A 2-layer closure of both the pharyngeal mucosa and musculature is advocated as this area is susceptible to dehiscence. 38 Following resection of the lesion, stability of the CVJ can be addressed through this approach using the transoral atlantoaxial reduction plate systems. 39 Disadvantages of this approach include a deep working distance and restrained operative view, and greater exposure in this approach can be achieved via La Fort I or transmandibular osteotomies.
The Posterolateral Approach 40
This approach allows good exposure of the anterior and lateral lesion at the CVJ, and particularly suited for lesions with high vascularity. It can be performed in the prone position with the head in a Mayfield frame, but other positions have been described. The skin incision begins at the mastoid and ascends superiorly and continues inferior to the superior nuchal line before descending the midline to C4. It can be extended caudally and cephalad as required. Of note, if instrumentation is required, bilateral exposure is a requirement.
Occipitocervical Fixation
This may be required in patients with radiographic instability of the CVJ. The treatment goals in this scenario are reduction, immobilization, and instrumented fixation. 40 Complications of occipitocervical fixation include cerebellar trauma from occipital screw placement, meningitis, vertebral artery injury, and direct trauma to neurological tissues including the spinal cord. The evidence for the selection of fixation constructs at CVJ is clear with cranial and cervical screw fixation constructs superior to wire or cable constructs. 41,42 The screw fixation constructs preformed better on pain relief, correction of malalignment, and achieved high fusion rates of 94% to 97%. Complication rates in a recent series range from 12% to 30%. 43,44
Craniocervical Junction Tumors in Children
Tumors of the craniocervical junction, including malignant tumors, are thankfully rare in the pediatric population. This clinical issue may enter the scope of practice of the readership, and as such it warrants inclusion in this review. The pediatric population typically presents benign pathology in this anatomical region. Menezes, 45 in a series from a single institution, of 38 pediatric patients below the age of 16 years who underwent operative intervention, reports the most common pathology at this level as chordoma, followed by fibrous dysplasia and aneurysmal bone cysts. In this group the pain in the distribution of the C2 dermatome was the most frequent presentation, occurring over two thirds of this cohort, with a third presenting with cranial nerve palsies. Chordomas are radio-resistant and hence require surgical resection. Factors considered important in developing a treatment plan include child age, potential for growth, craniovertebral stability, and benign of malignant pathology. 46
Discussion
In dealing with this rare clinical entity, making use of all available evidence can help decision making in the clinical setting. Patients with this pathology typically present with occipital neuralgia, which presents as headaches in the suboccipital region and retroauricular areas, 9 with rotational pain present in 90% of patients with CVJ involvement. 10 Of note, myelopathy is an uncommon presenting complaint. Plain radiographs are not sensitive in revealing metastatic lesions in bone, as over half of patients will have normal findings on the radiograph. MRI appears to be the gold standard imaging modality in characterizing cervical spine tumors, for both soft tissue and bone tumors. 12 Decision making in this cohort of patients can prove difficult. Fehlings et al 21 preformed a literature review in 2009 and found no level 1 evidence but provided guidelines advocating for posterior approach in surgical candidates and radiotherapy for patients with stable CVJ. Azad et al 22 preformed a retrospective review of 25 patients with a mean SINS of 7.3, with metastatic disease affecting the CVJ, and found acceptable results for these patient when treated with SRS. In contrast, the retrospective review by Bilsky et al 10 showed a long median survival rate for the group undergoing operative intervention of 16 months compared to 5 months for receiving EBRT alone. Once surgical intervention is required, 3 described approaches are most frequently employed: posterior, posteriolateral, and transoral. The posterolateral approach allows good exposure of the anterior and lateral lesions and is suited for lesions with high vascularity. 40 The transoral route is useful for the correction of irreducible anterior compression at the cervicomedullary junction 36,37 but has the disadvantage of an deep working distance. Pertaining to implant selection, cervical screw fixation constructs are superior to wire or cable constructs, 41,42 with these fixation constructs preforming better on pain relief, correction of malalignment, and achieved high fusion rates of 94% to 97%. A significant complication rate, ranging from 12% to 30%, is attached to these surgeries. 43,44
Conclusion
The CVJ is a complex anatomical structure comprising 4 synovial joints and accounts for 50% of all head and neck movements. Despite only 0.5% of all metastatic disease to the spine occurring at the CVJ, it presents a challenging clinical scenario. Prompt evaluation of rotational neck pain 10 with or without occipital neuralgia may reveal early metastatic disease within a stable CVJ. MRI appears to be the gold standard imaging modality in this pathology with nuclear bone scan playing a role in distinguishing benign and malignant processes, where CT-guided biopsy might prove difficult in execution. Unfortunately, no level 1 evidence exists for use of either radiotherapy or surgery in these cases; however, from the available literature, spinal instability and evidence of progressive neurology are relative indications for operative intervention. Instrumented fixation constructs for the stabilization of the CVJ appears to be superior to wire or cable constructs in this setting. Pathologies in the pediatric population present a rarely encountered but uniquely challenging clinical scenario.
Footnotes
Acknowledgments
The authors would like to acknowledge the contribution of Patricia O’Sullivan for her illustration in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.