
Abstract
Controversy exists as to the most effective management option for elderly patients with type II odontoid fractures. The purpose of this study is to evaluate outcomes associated with rigid cervical collar and posterior fusion surgery. Patients with ≥ 50% odontoid displacement were treated with posterior fusion surgery including C1–2 (PSF group, n = 25, average age = 80 years). Patients with < 50% odontoid displacement were treated with a rigid cervical collar for 12 weeks (collar group, n = 33, average age = 83 years). These inhomogeneous groups were followed for an average of 14 months. Fracture healing rates were higher in the operative group (28% versus 6%). Neck Disability Index scores were slightly lower in the nonoperative group (13 versus 18.3, p = 0.23). Analogue pain scores were also slightly lower in the nonoperative group (1.3 versus 1.9, p = 0.26). The mortality rate was 12.5% in the collar group and 20% in the operative group. Complications were higher in the operative group (24% versus 6%). Rates of type II odontoid facture healing and stability appear to be higher in geriatric patients treated with posterior fusion surgery. Fracture healing and stability did not correlate with improved outcomes with respect to levels of pain, function, and satisfaction. Mortality and complication rates are lower in those patients with lesser-displaced fractures who are treated with a cervical collar and early mobilization.
Odontoid fractures are the most common of all spinal fractures for patients older than 70 years of age. These fractures typically present significant challenges as geriatric patients often have multiple clinical comorbidities that may adversely affect fracture management. Numerous studies have demonstrated high rates of mortality with these injuries in elderly patients regardless of intervention. 1 , 2 , 3 , 4
Treatment options for displaced odontoid fractures may be conservative or surgical. Alternatives include the use of a cervical collar, halo vest, posterior C1–2 fusion with rigid fixation, and odontoid screw fixation. Presently, there is no consensus regarding which method is most efficacious. External immobilization with a collar has had inconsistent reported results. 5 , 6 , 7 , 8 Halo vest immobilization in the elderly is associated with significant complications, increased morbidity, and high rates of nonunion. 3 In addition, elderly patients having surgery for type II odontoid fractures have a higher risk of complications including mortality. 9
Management of geriatric patients with odontoid fracture should be focused on rapid mobilization of the patient in a collar or after surgical stabilization. Many spinal trauma specialists feel the halo vest should be avoided in this population. 10 The existing literature remains unclear as to the most effective management option for geriatric type II odontoid fractures and significant controversy still exists. Furthermore, outcomes for those patients who do not achieve fusion or fracture healing after treatment remain unclear. The morbidity of odontoid nonunion in this population is also not well defined.
The purpose of this study is to evaluate fracture healing rates, functional outcomes, complications, and mortality associated with rigid cervical collar and posterior fusion surgery for the management of geriatric type II odontoid fractures.
Methods
Institutional Research Review Board approval was obtained for this study. From 2003 to 2011, 58 consecutive patients over age 65 years with acute type II odontoid fractures were treated by the same fellowship-trained spinal surgeon (R.W.M.) at a level 1 trauma center. Odontoid fracture displacement was measured on the initial injury computed tomography scan sagittal images. Patients with 50% or greater odontoid displacement were treated with posterior fusion surgery including C1–2 (PSF group, n = 25, average age = 80 years). Patients with less than 50% odontoid displacement were treated with a rigid cervical collar for 12 weeks (collar group, n = 33, average age = 83 years).
Hospital and outpatient chart reviews were performed evaluating patient comorbidities, treatment complications, and mortality rates. At the time of ultimate follow-up, patients had open mouth, flexion, and extension radiographs to assess fracture stability and healing. Additionally, functional outcomes were assessed using Neck Disability Index (NDI), analogue pain, and satisfaction questionnaire scores at the time of ultimate follow-up.
Study parameters included fracture healing, fracture stability, treatment complications, mortality, and functional outcome comparison between the collar and PSF groups. Additionally, functional outcomes (NDI, pain, and satisfaction scores) were compared between those patients who developed hypermobile nonunion and those patients who had stable fracture union.
Results
Thirty-three patients were identified as having less than 50% odontoid displacement on initial imaging studies and were treated with a Miami J-type rigid cervical orthosis (collar group). None of these patients presented with a neurological deficit. Sixteen were men and 17 were women. The average age of the patients was 83 years with a range from 65 to 91 years. Each patient was identified as having significant medical comorbidities. The average number of comorbidities for the patients treated with cervical collar immobilization was 4.3 with a range from 1 to 10 comorbidities (Table 1). Patients were instructed to wear their Miami J cervical collar 24 hours day for a period of 12 weeks. They were also provided with a second cervical liner for showering. Routine follow-up visits were performed at the 2-week, 6-week, and 3-month postinjury periods. Twenty-eight patients (85%) were available for additional clinical follow-up beyond the 3-month postinjury period. In the PSF group, mean follow-up was 13.7 (0.25 to 48) months. Patients in the collar group were followed for an average of 13.9 (2 to 48) months. There was no prescribed limitation on physical activity for any patient who developed mobile odontoid nonunion in the postoperative period.
Patients and treatments
Abbreviations: AAA, abdominal aortic aneurysm; afib, atrial fibrillation; AVR, aortic valve regurgitation; BPH, benign prostate hyperplasia; Ca, cancer; CABG, coronary artery bypass graft; CAD, coronary artery disease; CHF, congestive heart failure; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CSF, cerebrospinal fluid; CVA, cerebrovascular accident; DMT2, diabetes mellitus type II; DVT, deep venous thrombosis; GERD, gatroesophageal reflex disease; HLD, hyperlipidemia; HTN, hypertension; Hx, History; MI, myocardial ischemia; OA, osteoarthritis; PAC, premature atrial contractions; PSF, posterior spinal fusion; PUD, peptic ulcer disease; R, right; RA, rheumatoid arthritis; S/P, status post; SVT, supraventricular tachycardia; TURP, transurethral radical prosthetectomy; UTI, urinary tract infection; XRT, radiation therapy.
Twenty-five patients had initial fracture displacement greater than or equal to 50% (Fig. 1) and were treated with instrumented posterior fusion including C1–2 (PSF group). Fifteen were men and 10 were women. The average age of the patients was 80 years with a range of 65 to 90 years. Comorbidities for the PSF group averaged 5.4 with a range of 1 to 10 (Table 1). Two patients presented with neurological deficit (American Spinal Injury Association classification B), and one patient had a noncontiguous spinal injury (C6 fracture). All 25 patients had posterior fusion surgery including C1–2 performed by the same surgeon (R.W.M.). The surgical technique for posterior C1–2 fusion consisted of the use of bilateral C1 lateral mass screws and C2 fixation using either C2 pedicle or translaminar fixation. C1 lateral mass and joint exposure was facilitated by intentional sacrifice of the bilateral C2 nerve roots along with decortication and local autogenous bone grafting of the bilateral C1–2 joints. Nine of the patients had additional fixation below the level of C2 due to either dysplastic C2 pedicular anatomy or severe osteoporosis. None of the 25 patients had iliac crest bone graft harvesting. Operative time, estimated blood loss, hospital stay length, and preoperative complications were recorded for each patient. Patients were evaluated for routine clinical follow-up at 2 weeks, 6 weeks, and 3 months. Nineteen patients (76%) were available for longer-term follow-up greater than 3 months after injury.
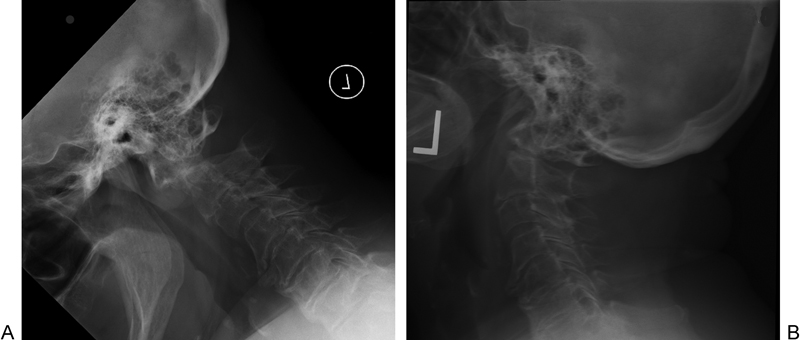
Midsagittal initial injury computed tomography images demonstrating (A) <50% odontoid displacement and (B) > 50% odontoid displacement.
Fourteen of the 25 patients in the PSF group had isolated C1–2 posterior fusion using bilateral C1 lateral mass and either C2 pedicle or translaminar bilateral fixation. Eleven patients in the PSF group had C1–2 posterior fusion including at least one additional level of spinal fixation. Surgical time for all 25 patients in the PSF group averaged 109 minutes with a range from 56 to 229 minutes. Estimated blood loss averaged 319 mL with a range of 100 to 700 mL. The average hospital stay length for the PSF group was 7.1 days (range 2 to 20 days).
The average follow-up time was 14 months for all patients with a range of 3 to 48 months. Eighty-percent of all elderly study patients have at least 6 months of follow-up.
Both the collar group and the PSF group had similar average follow-up times (versus months). Age and number of comorbidities were also similar in both the PSF group and the collar group (age 80 and 5.4 comorbidities versus age 83 and 4.3 comorbidities).
Mortality
Mortality rates were 12.5% (4/33) in the collar group and 20% (5/25) in the PSF group (Table 2). One-year mortality was also higher in the operative group (20% versus 6%). Two perioperative deaths occurred in the PSF group. Both of the patients in the PSF group who died in the immediate postoperative period had at least six defined medical comorbidities and had death related to medical comorbidity. Two of the 33 patients in the collar group died during the initial 3-month treatment period and another two patients died ∼23 months after injury. The cause of death was investigated and death certificates were viewed for all four of the patients in the collar group. One of the four deaths in the collar group was attributed to blunt head trauma and three were listed as death occurring from natural cause.
Patient outcomes
Abbreviation: PSF, posterior fusion surgery.
Complications
Complications were more common in the PSF group (Table 2). Six of the 25 (24%) patients in the PSF group had complication during the treatment period. PSF group complications included one patient with a cerebrospinal fluid leak, one patient requiring immediate postoperative tracheostomy for airway obstruction, two patients with prolonged swallowing difficulty greater than 3 months after surgery (Fig. 2), and the two perioperative deaths. Only one patient in this series had occipital-cervical fixation, and this patient developed postoperative airway obstruction requiring emergent tracheostomy. Collar group complications were limited to two patients who developed significant skin breakdown in the neck region from prolonged full-time cervical collar wear (6%).
Barium swallow lateral image demonstrating esophageal narrowing in a patient treated with posterior fusion surgery who had prolonged swallowing difficulty greater than 3 months after surgery.
Odontoid Fracture Healing
Fracture healing was determined by evaluating the neutral lateral and open mouth radiographs for evidence of bridging bone across the odontoid fracture site. Significant limitation exists in the determination of definitive C1–2 bony fusion on these images, and in the absence of computed tomography, the authors specifically chose not to include radiographic evidence of C1–2 posterior fusion as study parameter in this report. Radiographic fusion rates were low in both groups. Evidence of radiographic fracture healing rates was observed in seven of the 25 PSF group patients (28%) and only two of the 33 collar group patients (6%).
Nonunion of the fracture site was observed in 43 of the 52 study patients who completed at least 3 months of fracture treatment (83%). Rates of odontoid fracture nonunion were 65% (13/20 patients) in the PSF group and 94% (30/32 patients) in the collar group.
Nonunion was further classified as stable or mobile depending on the presence of any detectible odontoid fracture site motion on the ultimate patient follow-up flexion–extension lateral radiographs. None of the 13 patients in the PSF group with odontoid nonunion had evidence of mobile odontoid nonunion (Fig. 3). Twenty of the 30 patients in the collar group (67%) who had odontoid fracture nonunion demonstrated mobile odontoid nonunion on flexion and extension lateral radiographs at the time of ultimate follow-up. The average mobility of the nonunion was 2.5 mm with a range from 1 to 12 mm (Fig. 4, Table 1). No patient with mobile odontoid nonunion developed clinical myelopathy or spinal cord injury during the follow-up period.
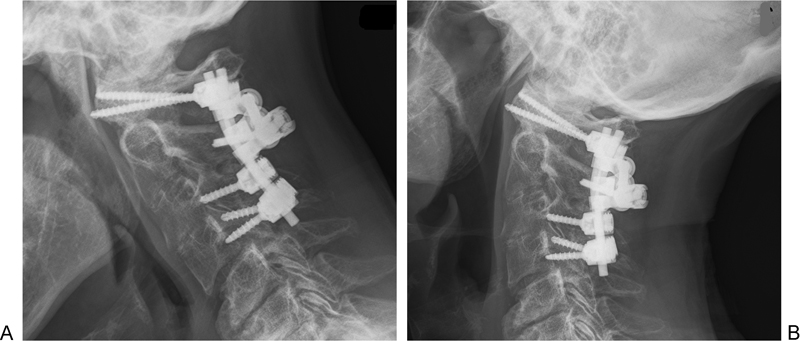
Flexion and extension lateral radiographs of a patient treated with posterior fusion surgery with stable odontoid nonunion.
Flexion and extension lateral radiographs of a collar patient with mobile odontoid nonunion.
Functional Outcomes
Neck Disability Index
NDI scores were used to assess functional outcomes for patients in each group. The NDI is scored using a point scale that ranges from 0 to 50. Each patient's raw score is doubled to achieve a percent score. Using this scoring system, a score of 10 to 28% (that is, 5 to 14 points) is considered to constitute mild disability; 30 to 48% is moderate; 50 to 68% is severe; and ≥ 72% is complete disability. The average NDI score for patients in the nonoperative group was 13 with a range of 0 to 28 points. NDI scores in the PSF group averaged 18.1 with a range of 0 to 48 points. The 5.1-point difference between average NDI scores in the PSF and collar groups was not statistically significant (p = 0.26, t test).
Pain Score
Pain was scored using an analogue pain scale with a range from 0 (no pain) to 10 (maximal pain). Analog pain scores at the time of ultimate follow-up indicated low levels of pain in both groups. The average pain score for the PSF group was 1.8 with a range of 0 to 7. The average pain score for the collar group was 1.3 with a range of 0 to 4. There was no statistically significant difference in pain scores between the two groups (p = 0.23, t test).
Patient Satisfaction
Patient satisfaction was evaluated using an analogue satisfaction scale with scores from 0 (no satisfaction) to 10 (maximal satisfaction). Satisfaction scores for the 52 geriatric patients were high. The average satisfaction score for PSF group patients was 8.9 with a range of 5 to 10. Satisfaction scores for the collar group averaged 9.2 with a range of 3 to 10. There was also no statistically significant difference between satisfaction scores for each group.
Mobile Odontoid Nonunion
Twenty of the 30 patients in the collar group had mobile odontoid nonunion. Mobile nonunion was not associated with lower functional outcome scores at the time of ultimate follow-up.
NDI scores for the 20 patients with mobile odontoid nonunion averaged 13.1 with a range from 0 to 25. NDI scores for the combined group of patients from both the collar group and the PSF group who achieved odontoid fracture healing or stable odontoid nonunion (n = 32) averaged 16.1 with a range of 0 to 48. There was no statistically significant difference in NDI scores between the 20 patients with hypermobile odontoid nonunion and the 32 patients who achieved odontoid healing or stabile nonunion after treatment (p = 0.34, t test).
Pain scores for the 20 patients with mobile odontoid nonunion averaged 1.2 points with a range of 0 to 5 points. The average pain score for the 32 patients with stable odontoids was 1.5 with a range of 0 to 7 points. There was no statistical significance between the pain scores (p = 0.42, paired t test).
Scores for patient satisfaction were also similar between those patients who had mobile and stabile odontoids (9.2 versus 9.0) with no statistically significant difference (p = 0.58, paired t test).
Discussion
Considerable controversy still exists with regard to the management of elderly patients with type II odontoid fractures. Unfavorable outcomes and increased complications with both operative and conservative management have been described in the literature. 3 , 8 , 11 , 12 Predisposition to unfavorable outcomes in this population is due to many factors associated with aging, medical comorbidities, and declining patient mobility. Furthermore, advanced age and fracture displacement have been associated with the failure of nonoperative treatment. 13
Reported nonunion rates with nonsurgical management of type II odontoid fractures have ranged from 35 to 85%. 2 , 14 , 15 , 16 , 17 , 18 , 19 Elderly patients do not tolerate prolonged immobilization in a halo vest, and complications and morbidity is high when the halo device is used in elderly patients. Complication rates of 66% and mortality rates of 42% have been reported with halo use in the elderly population 10 , 12 , 20 , 21 Smith et al recently reported an increased incidence of airway compromise with halo use in the elderly population. 8 Kuntz et al reported early failure of elderly patients treated with halo vests due to complications of halo vest wear including failure to thrive, respiratory failure, and inadequate fracture stabilization. Fifty percent of the patients in this study had early failure of halo management. 3 Furthermore, Apfelbaum et al showed 8 mm of motion across the dens fracture site with respiratory cycles and concluded that halo wear does not adequately immobilize the dens fracture site. 14
Operative risk has been well defined in the elderly population. Risk escalates with increasing age and medical comorbidity. Potential fatal perioperative complications including airway obstruction with respiratory compromise, myocardial infarction, and cerebrovascular accident have been described. Smith et al reported a 12.5% perioperative mortality rate along with a 62% rate of significant complications in 32 elderly patients who had surgical management of displaced odontoid fractures. 8 Schoenfeld et al reported a 21% 1-year mortality rate with operative management. 9
Reports of successful operative management of geriatric odontoid fractures have been published. Frangen et al retrospectively analyzed 27 geriatric patients with a median age of 86 years who underwent operation for isolated unstable type II odontoid fractures. 2 Twenty-two percent (six patients) died during the observation period at a median of 40 days after injury due to either cardiopulmonary failure or pneumonia. All 21 surviving patients were reevaluated an average of 3 months after trauma. All but one showed a stable fusion and had no or minor neck pain. The authors concluded that posterior stabilization of unstable odontoid fractures with transarticular screws and modified Gallie fusion in older patients can be performed safely, with good clinical results and few complications. Mortality remained high but was lower than reported after halo vest immobilization alone. They also suggested that posterior C1–2 fusion is superior to halo vest immobilization in terms of nonunion rate and mortality, and it might be the treatment of choice in this high-risk patient population.
Other retrospective studies have compared outcomes of surgical and nonsurgical management of elderly odontoid fractures. Chaudhary et al compared nine patients treated with a collar and 11 patients treated with either anterior or posterior surgery. 1 High rates of healing were reported in both groups with 66% of patients with rigid collar and 87% of the surgical patients having fracture union. At average 5-month follow-up, mortality was higher in the operative group (27% versus 11%). The authors concluded that patients treated with a nonrigid collar seem to have an overall favorable outcome, but further research is needed to compare the outcomes of surgical and nonsurgical management of geriatric odontoid fractures. Kuntz et al evaluated 12 patients treated with external immobilization and 11 patients treated with either anterior or posterior surgery. 3 Approximately 10% morbidity and mortality rates were reported in both groups. Nonsurgical management with a cervical orthosis had a 50% failure rate and was associated with one death. Surgical management had a 9% early failure rate. The results of surgical management appear to be better in this small retrospective series of patients. Smith et al in a multicenter retrospective study compared 32 patients having either anterior or posterior surgery with 40 patients who had nonsurgical treatment with either a collar or a halo device. 8 Acute in-hospital mortality was 12.5% in the operative group and 15% in the nonoperative group, and complications were higher in the operative group (65% versus 35%). Rates of fracture healing and functional outcomes were not reported in this study. A high incidence of airway complications was noted in both the operative and nonoperative groups (31% and 18%). Additional retrospective studies reporting successful surgical management of small series of patients have been published. 2 , 22 , 23
Our series of 58 consecutive elderly patients with odontoid fractures is possibly the largest series of consecutive patients treated by the same surgeon to be reported in the literature. We observed similarly high rates of preexisting comorbidities in both our operative and nonoperative patient groups (5.4 versus 4.3). The results of our series demonstrate high mortality rates with both collar and posterior surgical stabilization surgery. Even though average surgical time and blood loss was low, peri-injury mortality was higher with surgical management. Three operative patients died within 4 weeks after surgery, accounting for a 12% early mortality rate. Only 2 of the 33 patients treated with a cervical collar died within 3 months of treatment (6% acute mortality). Mortality rates in the PSF group were also somewhat higher at average 13-month follow-up (20% versus 12.5%). The rates for operative mortality in this series are similar to previously reported rates in the literature for geriatric patients with type II odontoid fractures and multiple comorbidities. However, rates for acute mortality in the collar group are among the lowest reported with conservative management of geriatric type II odontoid fractures. The low mortality rate for nonoperative patients in our study may be attributed to the earlier mobilization of these patients. Early mobilization with bed to chair was encouraged soon after collar fitting in the patients in the collar group.
Complications in the collar group in our study are also relatively low. Smith et al compared a series of 72 geriatric type II odontoid fracture patients treated with surgery of external immobilization and reported a higher incidence of complications in the operative group with 62% of the operative patients experiencing at least one significant complication. 8 Thirty-five percent of the nonoperative group experienced at least one significant complication with many being attributed to halo vest wear. In our series, major complications were noted in six patients in the PSF group (24%). Only two patients in the collar group experienced complications related to cervical collar wear (6%). The lower rate of complications with nonoperative management in our series may be related to the use of the more flexible Miami J cervical collar and the absence of patients using a halo along with the emphasis on early patient mobilization after initial cervical collar fitting.
Varying rates of odontoid fracture healing in the elderly population after both surgical treatments have been reported in the literature. Omeis et al reported a 30.7% odontoid healing rate with posterior C1–2 surgery and a 37.5% healing rate with anterior odontoid screw fixation in the elderly population. 24 Chaudhary et al reported 87% fracture union after surgical treatment and 66% union with cervical collar treatment. 1 Fracture healing in our study was low in all patients regardless of treatment type. In the operative group, only 28% of the patients demonstrated radiographic healing across the fracture site. A lower rate was demonstrated in the nonoperative group with only 6% of the patients who were treated with a collar demonstrating radiographic evidence odontoid fracture union. Nonunion rates reported in our series are among the highest reported in the existing literature for geriatric odontoid fractures.
There is a paucity of literature addressing functional outcome after the treatment of geriatric spine fractures. Our study is among the few to evaluate neck disability after surgical and nonsurgical elderly odontoid fracture management. We found functional outcomes to be similar in both the collar group and the group having posterior spinal fusion. Both groups had average NDI scores that were consistent with low levels of disability, and there was not a statistically significant difference between the NDI scores for both groups. There was, however, a slight trend toward lower NDI scores in the nonoperative group (p = 0.23, t test). Analogue pain scores were also low in both groups at the time of ultimate follow-up indicating baseline levels of low neck pain in each group—again with slight tend toward lower pain in the nonoperative group (p = 0.26, t test). Additionally, patient satisfaction was equally high in both groups indicating low levels of dissatisfaction with treatment course and outcomes.
The frequency and morbidity of odontoid fracture nonunion in the elderly population is not well defined. Because of the risk of progressive myelopathy or sudden neurological injury, many surgeons recommend operative stabilization for patients with mobile dens nonunions who are able to withstand an operation. 25 There is, however, a lack of information about the radiographic and neurological progression of dens nonunions. 26 , 27 Although a less aggressive surgical approach has been recommended by some authors for elderly or medically compromised patients with acute fractures, long-term follow-up evaluation of patients with resulting nonunions has not been adequately reported. 13 , 26 One of the few studies was published by Hart et al, who performed a retrospective review of five elderly patients treated without surgery for chronic mobile nonunions of the odontoid process. 28 None of the reported patients had less than 14 mm available for the spinal cord in either flexion or extension at the start of clinical monitoring. Patients were observed on an annual basis for 4.5 years with clinical examinations and flexion–extensions plain film radiographs. None of the patients developed myelopathic symptoms during the follow-up period, and no patient experienced more than 1-mm radiographic increase in atlantoaxial excursion. The authors suggest that this close follow-up treatment protocol may be considered for patients who are poor candidates for surgical fusion. Other limited studies have also reported satisfactory outcomes in isolated patients with dens nonunions. 25 , 26 , 29
Nonunion of the fracture site in our study was observed in 43 of the 52 patients who completed at least 3 months of fracture treatment (83%). Rates of odontoid fracture nonunion were 65% (13/20 patients) in the PSF group and 94% (30/32 patients) in the collar group. Rates of odontoid nonunion for the collar group in our study were higher than previously reported in the literature for cervical collar treatment. Additionally, 20 of the 30 patients in the collar group (67%) who had odontoid fracture nonunion demonstrated mobile odontoid nonunion averaging 2.5 mm of motion on flexion and extension lateral radiographs. Consistent with the findings of Hart et al, no patient with mobile nonunion in our study was observed to develop clinical myelopathy or spinal cord injury during the follow-up period. 28 A further investigation into the cause of death of the three patients in the collar group revealed that only one of the three expired from complications involving a fall and resultant head trauma. This is the only study patient we could identify as possibly experiencing an untoward neurological event related to the odontoid nonunion without conclusive evidence.
Limitations of our study exist in the retrospective manner of data collection and in the relatively short follow-up time in a geriatric population. Also, the patients stratified into the operative and nonoperative treatment arms in our study were not clearly homogeneous, as those patients with greater initial fracture displacement likely had more significant injury.
The results of our study did not demonstrate any evidence of lower functional outcome for those patients who had mobile odontoid nonunion. NDI scores for those patients with mobile odontoid nonunion did not differ significantly from those patients who achieved fracture healing in both groups. Also, there was no statistically significant difference between levels of neck pain reported in those patients who had mobile nonunion and those patients who had odontoid fracture healing or stabile odontoid nonunion.
Conclusion
In this series of 58 consecutive geriatric patients with type II odontoid fractures, rates of odontoid healing and stability appear to be higher in those patients who were treated with posterior fusion surgery. Fracture healing and stability did not correlate with improved outcomes with respect to levels of pain, function, and satisfaction. Mortality and complication rates were lower in those patients with lesser-displaced fractures who are treated with a cervical collar and early mobilization.
This study suggests that elderly patients who have lesser displaced fractures may be appropriately treated with a cervical collar. It also suggests that elderly patients with greater displacement have similar functional outcomes with surgical treatment. Outcomes of geriatric patients with greater-displaced odontoid fractures treated with a collar were not addressed in this study and unfortunately still remain unclear.
Disclosures
William J. Molinari III, None
Robert W. Molinari, AO Fellowship Grant for the University of Rochester Spinal Surgery fellowship
Oner A. Khera, None
William L. Gruhn, None
Footnotes
Acknowledgments
The authors wish to thank Kimberly Napoli for assistance in preparation of this manuscript.