
Abstract
Study Design:
Retrospective study.
Objectives:
We examined the impact that location of a lumbar disc herniation has on the likelihood that a patient will require surgery after at least 6 weeks of nonoperative management.
Methods:
Using ICD-10 codes M51.26 and M51.27, we identified patients at a single academic institution from 2015 to 2016 who received a diagnosis of primary lumbar radicular pain, had magnetic resonance imaging confirming a lumbar disc herniation, and underwent at least 6 weeks of nonoperative management. Patients experiencing symptoms suggesting cauda equina syndrome or progressive motor deficits were excluded.
Results:
Five hundred patients met inclusion/exclusion criteria. Twenty-nine (5.8%) had L3-L4 herniations, 245 (49.0%) had L4-L5 herniations, and 226 (45.2%) had L5-S1 herniations. Overall, 451 (90.2%) patients did not undergo surgery within 1 year of diagnosis. Nonsurgical patients had an average herniation size occupying 31.2% of the canal, compared with 31.5% in patients who underwent surgery. While herniation size, age, sex, and race failed to demonstrate a statistical association with the likelihood for surgery, location of disc herniation demonstrated a strong association. L3-L4 and L4-L5 herniations had odds ratios of 0.19 and 0.45, respectively, relative to L5-S1 herniations (P = .0047). Patients were more than twice as likely to require a surgery on an L5-S1 herniation in comparison with an L4-L5 herniation (P < .05). L3-L4 herniations rarely required surgery.
Conclusions:
Patients with caudal lumbar disc herniations were more likely to require surgery after at least 6 weeks of conservative management than those with disc herniations in the mid-lumbar spine.
Keywords
Introduction
Established treatment of lumbar disc herniation (LDH), excluding exigent conditions such as cauda equina syndrome and progressive or profound neurological deficit, entails conservative management for a minimum of 6 weeks after the initial diagnosis. 1,2 Many conservative treatment modalities have been used, including a combination of nonsteroidal anti-inflammatory drugs (NSAIDs), steroid injections, and/or physical therapy. 2,3 Regardless of the size of the disc herniation, most patients will experience considerable improvement from nonoperative treatment alone. 4 In approximately 10% of cases, however, conservative therapy may not sufficiently resolve pain symptoms; in these instances, surgical treatment is indicated. 5
Lumbar spine anatomy varies from level to level. Cranially, the discs are relatively smaller and the spinal canal is more ovoid in shape; as one moves caudally, the spinal canal takes on a more triangular shape and load bearing is increased. 6 Some studies have noted a higher rate of degenerative disc disease in the more caudal regions resulting in an increased possibility for lumbar stenosis, among other pathologies. 7 This may have an impact on the rate of resolution of symptoms following a lumbar disc herniation, and in turn, may also affect the likelihood of successful non-operative treatment, where symptoms resolve without the need for surgery.
To our knowledge, the association between lumbar disc herniation location, as a function of spinal level, and the likelihood that a given patient will fail nonoperative management has not previously been studied. In this article, we seek to identify if such a relationship exists. Given the variance in anatomy across the lumbar spine, described above, we predict that the frequency that patients with an LDH fail conservative management will be progressively higher in more caudally located lumbar disc herniations.
Materials and Methods
This retrospective study analyzed patients at a single academic institution from 2015 through 2016. All patients who received a diagnosis of primary lumbar radicular pain with magnetic resonance imaging (MRI) documentation of a lumbar disc herniation and who also had documented completion of at least 6 weeks of nonoperative management were eligible for inclusion in the study. Conservative management was defined as at least 2 of the following treatment modalities for a minimum of 6 weeks: NSAIDs, gabapentin, pregabalin, or pain medication; epidural or transforaminal steroid injection; and physical therapy. Patients were identified using the ICD-10 (International Classification of Diseases, 10th Revision) code M51.26 (other intervertebral disc displacement, lumbar region) and M51.27 (other intervertebral disc displacement, lumbosacral region). Specifically, only those herniations occurring between L3-L4, L4-L5, or L5-S1, were included in this study, as herniations occurring at other vertebral levels were regarded as being atypical. 8 If a patient demonstrated multiple disc herniations, only the location where the herniation was largest was considered for purposes of analysis. All patients were at least 18 years of age.
Exclusion criteria consisted of any previous lumbar surgery (regardless of level), or lumbar surgery for any indication other than LDH. Only herniations leading to central or lateral stenosis were studied; foraminal herniations were excluded. All patients in this study had “soft” lumbar disc herniations. “Hard” disc herniations involving bony fragmentation, spurs, or endplate material were excluded. To avoid potential inclusion of patients with degenerative changes and not true disc herniations, any patients with a bulge smaller than 2 mm in the anterior-posterior dimension were excluded from the study. For this same reason, ICD-10 codes, M51.36 (other intervertebral disc degeneration, lumbar region) and M51.37 (other intervertebral disc degeneration, lumbosacral region), were not included in our initial search criteria. Finally, patients receiving emergency surgery due to a diagnosis of cauda equina syndrome were excluded from analysis.
Once inclusion and exclusion criteria for a given patient were met, medical records and data regarding the date of MRI and initial diagnosis were noted. Radiology reports were analyzed. Axial imaging on the MRI was evaluated to determine the image which contained the maximal amount of canal compromise due to the disc herniation. The spinal level of the herniated disc was noted and, if accessible, was measured using AGFA-IMPACS, a software program developed by AGFA-Gevart N.V. (based in Mortsel, Belgium). This application enables the measurement of both area and the distance between two user-defined points with a strong degree of precision, allowing the user to choose various points of an irregularly shaped object. Figure 1a and b provides sample images that contain measurements of a patient’s disc herniation and canal area, respectively. Should a patient have a disc herniation extending beyond one level, the larger herniation (measured on the basis of cross-sectional area) was utilized in our analysis.
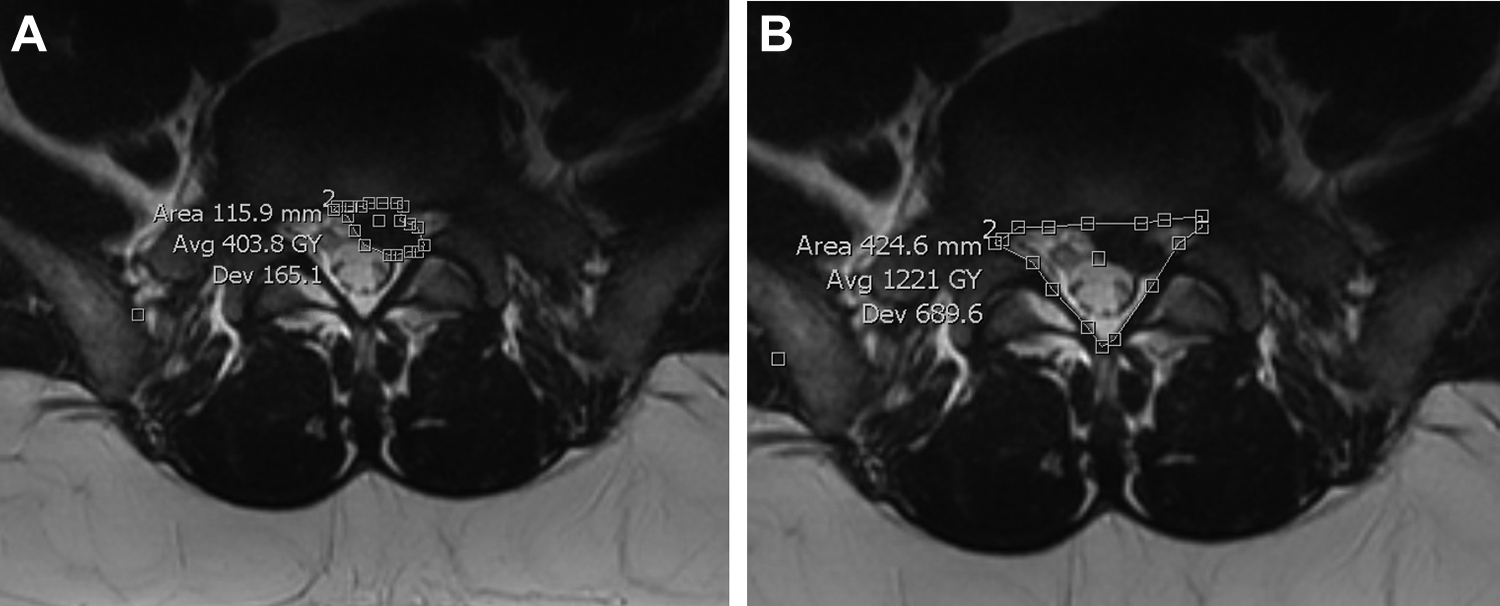
(a, left) A sample measurement of a patient’s disc herniation. (b, right) A sample measurement of that same patient’s canal area.
Within the axial view of an MRI, the following measurements were made on AGFA-IMPACS for a given disc herniation: the anterior-posterior length of both the canal and the herniated disc, the average width of the disc within the canal, the total canal area, and the total disc area. For anterior-posterior measurements the longest possible measurement was utilized, that is, where the canal or disc measured is at its maximum length while parallel to the sagittal plane. Mid-width measurements were made from the midpoint of the herniation along the anterior-posterior axis. These measurements are similar to those made in a study by Carragee and Kim, 9 as depicted in Figure 2. Area was measured using as many points as the user felt were necessary in order to trace a reasonable outline of a given canal or disc herniation. Finally, a logistic regression controlling for age, gender, race, and disc herniation size (as a percentage of canal area) was conducted to determine whether the location correlated with the likelihood that a patient received surgery after failing to improve with non-operative care. To further elucidate the impact of herniation location on the likelihood for surgery, a chi-square test was conducted.
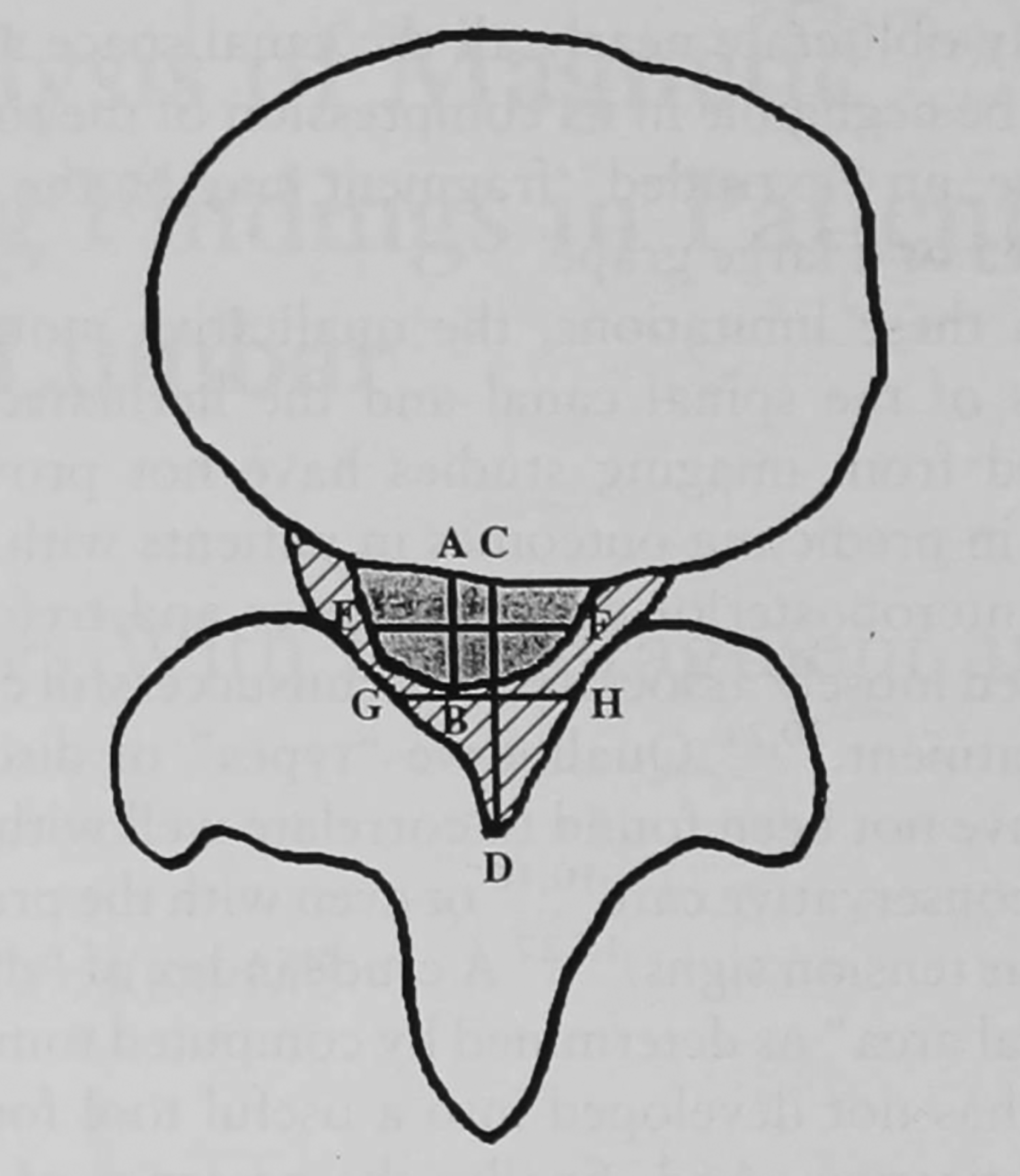
Schematic of a disc herniation as seen on magnetic resonance imaging. The shaded area represents the disc herniation. The shaded area and the hashed area in combination represent the canal area. Segment AB is the anterior-posterior length of the disc. Segment CD is the anterior-posterior measurement of the canal. Segments EF and GH represent the mid-width of the disc and canal, respectively. This image was adopted with permission from the study by Carragee and Kim. 9
Results
Five hundred patients met the inclusion and exclusion criteria for this study. Of these, 368 patients had accessible MRI scans from which axial imaging measurements (anteroposterior length, canal area, etc) could be made. The other 132 patients had MRI scans that could not be accessed via AGFA-IMPACS and therefore a precise herniation size could not be determined. However, all other parameters, including herniation location and patient demographics, were recorded and included in analysis.
Twenty-nine patients (5.8%) had an L3-L4 herniation, 245 (49.0%) had an L4-L5 herniation, and the remaining 226 patients (45.2%) had an L5-S1 herniation. No patients demonstrated disc herniation(s) spanning multiple spinal levels. Among the 500 patients in this study, 49 (9.8%) ultimately required surgery for their disc herniation within 1 year of diagnosis, after failing at least 6 weeks of nonoperative management. Table 1 provides disc herniation and demographic data, comparing patients who required surgery with those who were successfully treated via conservative management. As depicted, the surgical and nonsurgical patient populations were comparable across age, gender, and race distribution.
A Comparison Between Patients Who Required Surgery for Treatment of Lumbar Disc Herniation and Those Who Did Not.a
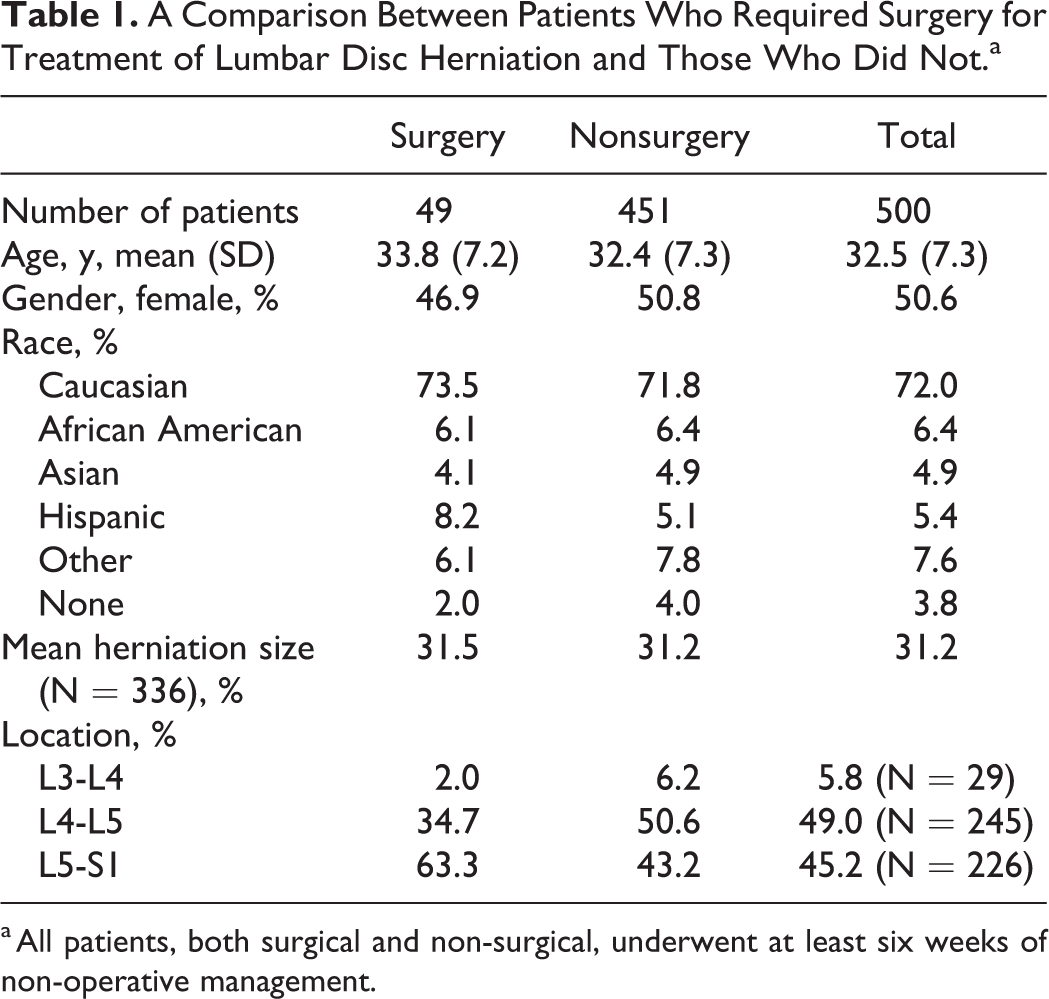
a All patients, both surgical and non-surgical, underwent at least six weeks of non-operative management.
L5-S1 disc herniations were the most commonly operated on, comprising nearly two-thirds of all surgeries, despite representing fewer than half of all herniations in this study. Conversely, L3-L4 disc herniations, which occurred in roughly 1 out of 17 patients from our sample, represented only 2% of all surgeries. Finally, L4-L5 herniations accounted for slightly more than one-third of all discectomies and occurred in nearly half of patients.
For the 368 patients for whom MRI imaging was available in AGFA-IMPACS, disc and canal areas were measured. The average size of lumbar disc herniation, evaluated as a percentage of disc size to canal area, was similar across both surgical and nonsurgical groups, regardless of location. Figure 3 highlights the similarity in disc herniation size across L4-L5 herniations and L5-S1 herniations. Data on L3-L4 herniations is not provided since only 1 out of the 29 patients in this study with an L3-L4 disc herniation required surgery.
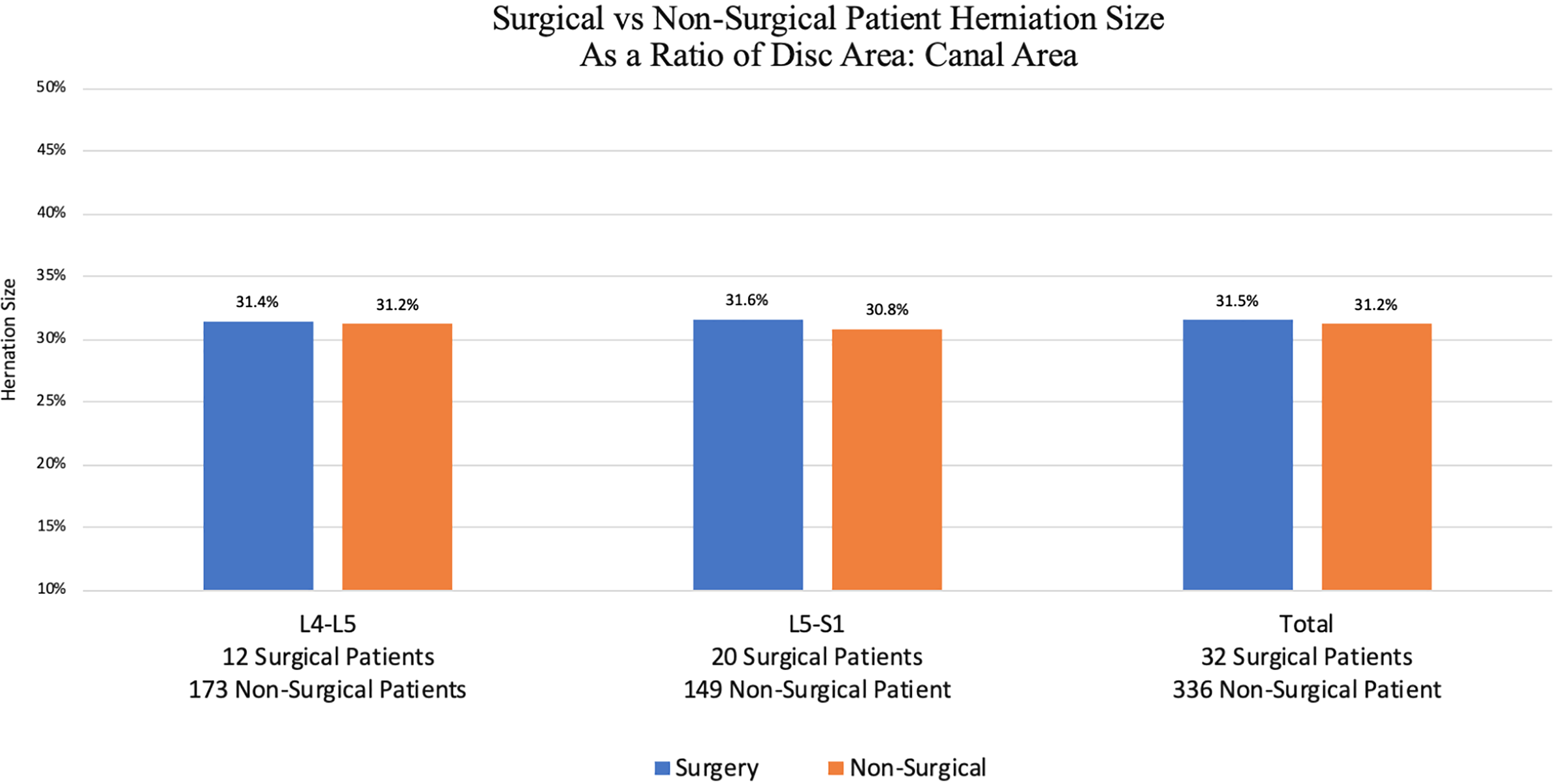
A stratified comparison (based on lumbar spine location) of disc herniation sizes between patients who ultimately required surgery versus those who were successfully managed through conservative treatment.
Table 2 depicts the results of a logistic regression analysis that considers the impact of race, gender, sex, location of herniation, and size of the disc herniation with regard to the likelihood that patients would improve with non-operative treatment. With the exception of the location of the lumbar disc herniation, none of these variables were statistically significant predictors of failed nonoperative management. Using L5-S1 as a reference, L4-L5 herniations had a statistically significant odds ratio of 0.45, indicating that disc herniations at L4-L5 are less likely to require surgery. A chi-square test that considers the relative anatomic locations of the L3-L4, L4-L5, L5-S1 disc spaces generated a P value of .004 741. This implies that the location of a disc herniation is statistically correlated with the likelihood for surgery; the more caudal the herniation, the more likely a patient is to undergo surgery as a result of failure to sufficiently improve after 6 weeks of conservative management.
A Logistic Regression Assessing the Impact of Race, Gender, Sex, and the Size/Location of a Herniation on the Likelihood That a Patient Will Require Surgery After 6 Weeks of Conservative Management.a
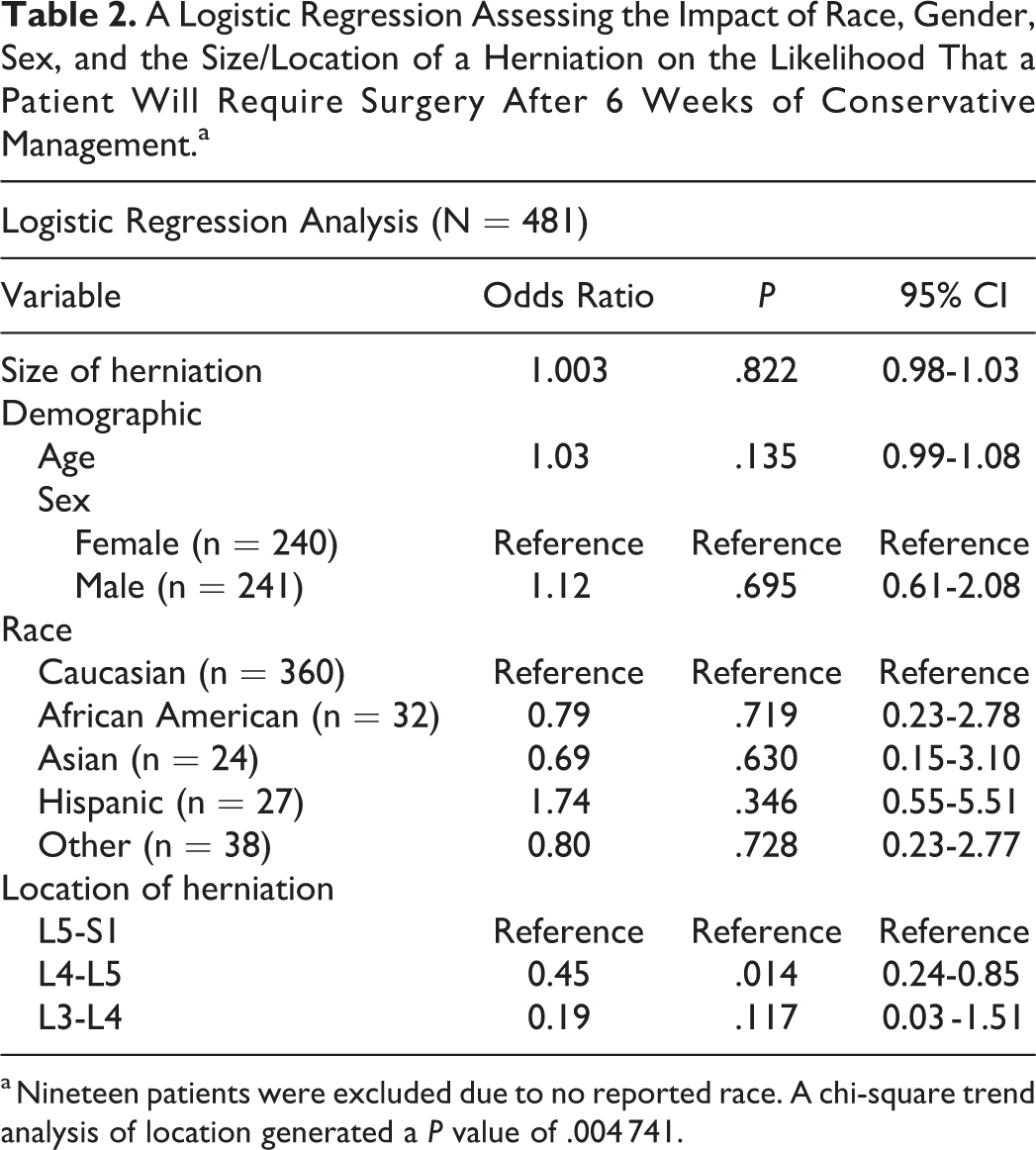
a Nineteen patients were excluded due to no reported race. A chi-square trend analysis of location generated a P value of .004 741.
Discussion
When exploring the effect of LDH location on the likelihood that a patient will require surgery, it is important to ensure all patients are receiving the standard of care. Per orthopedic literature, for all patients not suffering from exigent conditions such as cauda equina syndrome or profound/progressive neurological deficits, an initial attempt at conservative management of LDH for a minimum of six weeks is appropriate. 1,2 According to Gugliotta et al, 5 90% of lumbar disc herniations will resolve through this modality without the need for surgery. In this study, the overall surgical rate of 9.8% was consistent with this finding and paralleled what is cited or recommended in other studies. 5,10,11
Per Deyo and Mirza, 12 spine surgery rates in the United States are the highest in the world, nearly 5 times that of England or Scotland. Cribb et al 13 suggest that this may be due to a chronic fear of potentially missing a diagnosis of cauda equina in the setting of large, “fearsome” disc herniations. That said, as Benson et al 4 claim, even massive herniations can successfully be treated conservatively and do not reflect the likelihood for surgery after failed non-operative management. Unfortunately, in practice, this conservative approach may not always be followed. As Table 2 shows, the size of the herniation did not have any significant impact on the likelihood a patient underwent surgery, generating an odds ratio of 1.003 with a P value of .822.
In this study, the size of a disc herniation was evaluated as a percentage of spinal canal area that was occupied by the disc. This methodology is consistent with that of other studies, 14,15 though not the only way disc herniations have historically been measured. 16,17 Using herniation size relative to spinal canal area, instead of the 6 mm anteroposterior threshold proposed by Carragee and Kim 9 in a frequently cited study, allowed us to account for variations in canal area both across multiple patients and within a single spinal column. Lumbar discs and spinal canals increase in size as one moves caudally. 18 Therefore, in theory, a herniation of 5 mm in the L3-L4 region, for example, may represent a more clinically significant displacement of nucleus pulposus than a 5 mm extrusion in the L5-S1 region, where a higher volume of nucleus pulposus is present; interestingly, this was not what we found clinically.
With the standard of care and size of lumbar herniation accounted for, we considered other reasons that may explain the increased likelihood for failed conservative management of more caudally located disc herniations. In 1984, Guinto et al 19 first discussed the spontaneous regression of lumbar disc herniations. Clinicians have since offered various explanations for this phenomenon. Theories range from retraction of posterior longitudinal ligament tension to resorption by macrophage phagocytosis or lymphatic draining and dehydration. 20 -22 However, none of these explain why, according to our data, L5-S1 herniations specifically, are more likely to require surgery than lumbar disc herniations located more cranially.
Spinal anatomy may offer an explanation. Per Orita et al, 23 lumbar stenosis and other pathology is most common at the L5-S1 level for a variety of reasons. Discs that are more caudal bear additional loading relative to those above. Nerve roots are larger more caudally, where there is a higher incidence of disc degeneration, spondylosis, and subluxation. 23,24 This may enhance the likelihood that a patient’s symptoms could persist after 6 weeks of conservative management, leading a clinician to consider surgical decompression. In addition, lower nerve roots travel a more oblique path through the canal increasing the risk of stenosis and compression. 25 Finally, the spinal canal changes shape from ovoid to triangular as one moves caudally 6 ; the latter could be less ideal in the setting of LDH, where the nucleus pulposus typically extrudes from the relatively weaker posterolateral portion of the disc. 26 Bozkurt et al 6 found that postoperatively, patients with a triangular-shaped canal experienced higher satisfaction and a decrease in visual analogue pain scale after surgical decompression relative to more ovoid shaped canals. This finding may be indicative of the greater severity of symptoms in triangular canals relative to ovoid ones prior to surgery.
From a pathophysiology standpoint, healing from a disc herniation may be adversely affected in more caudal regions of the lumbar spine. Saal et al 20 stated that, “when material from the nuclear pulposus, separated from the nutrient supply of the disc, is exposed to the vascular supply of the epidural space, resorption begins.” Inflammatory responses promote phagocytosis of the extruded material and progressive desiccation ensues. 27 However, in the presence of stenosis, more common to caudal regions of the lumbar spine, Saal and Saal 11 warn that desiccation can be impeded. Stenosis can cause an interrupted or diminished blood supply, resulting in a delayed resorption of offending material and prolonged compression by the herniated nucleus pulposus. Enduring inflammation enhances the extruded discs ability to maintain high water content and delay healing. 28
While the precise reason for an increased incidence of failed conservative management of caudally located LDHs is not known and requires further exploration, this finding bears clinical relevance. Perhaps more caudal herniations require a greater amount of time for proper healing to take place, given the difference in anatomy and increased incidence of pathology such as lumbar stenosis. Moreover, as Saal and Saal 11 state, failure of passive nonoperative treatment alone is not sufficient for the decision to operate; the decision for surgery should be made on the basis of a patient’s relative functional improvement over time while undergoing active rehabilitation rather than simply on imaging studies. Furthermore, though some studies claim that the optimal time for operating on a LDH is roughly 6 to 8 weeks after the initial diagnosis, 29 others have shown that maximal improvement may not occur until 12 weeks. 11 Perhaps exploration of a slightly different timeline for conservative management of lumbar disc herniations, on the basis of location, is worth considering based on our findings. Studies from other centers would be useful in validating this possibility. Or, it may simply be the case that, regardless of the exact mechanism or pathophysiology, herniations are progressively more likely to require surgery as one moves caudally through the lumbar spine.
Limitations of this study include patient loss to follow-up. It is entirely possible that some of the patients in this study sought a second opinion after attempting 6 weeks of conservative management prescribed by clinicians at our academic medical center. They may have received surgery at another site without our knowledge, thus skewing the actual surgical rates recorded in our data. We did our best to control for this by ensuring thorough medical and surgical histories were taken on return to our hospital. Other factors that may have affected primary outcome measures include insurance status, socioeconomic status, workers’ compensation, a given surgeon’s proclivity to operate, and any lawsuits/litigations relating to the injury. Data relating to many of these factors can be understandably difficult to control for.
Another limitation was our inability to obtain follow-up MRIs after the initial one. Though many patients reported resolution of symptoms after several weeks of conservative management, having imaging studies to monitor the resolution of the lumbar disc herniation may have been helpful in explaining why more cranial LDHs appear to heal more effectively than those located more caudally. In most instances, insurance companies would not cover follow-up MRIs, as resolution of symptoms obviates the need for another imaging study. It is also possible that follow-up longer than the 1-year time frame used in this study might reveal additional patients that eventually opted for surgery to relieve symptoms.
In future studies, it may be helpful to stratify herniations not just by disc level but also type. In this study, we simply included herniations leading to central or lateral stenosis while excluding foraminal stenosis. We did not, however, distinguish between broad based versus focal or contained versus sequestered versus extruded. These parameters may help explain, in part, some of our observations and allow for greater insight into the underlying pathophysiology. Nonetheless, given the large sample size of 500 patients and our statistically significant finding, we believe that the location of a lumbar disc herniation is indeed correlated with the likelihood for surgery in the future after 6 weeks of conservative management. We found that the more caudal the LDH, the more likely a patient will ultimately require surgery. Nevertheless, most patients, even those with L5-S1 herniations, will benefit from nonoperative treatment and ultimately exhibit a resolution of symptoms without the need for surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.