
Abstract
Study Design
Systematic review.
Clinical Questions
(1) What is the comparative efficacy of unilateral instrumentation compared with bilateral instrumentation in spine surgery? (2) What is the safety of unilateral instrumentation compared with bilateral instrumentation in spine surgery?
Methods
Electronic databases and reference lists of key articles were searched up to September 30, 2014, to identify studies reporting the comparative efficacy and safety of unilateral versus bilateral instrumentation in spine surgery. Studies including recombinant human bone morphogenetic protein 2 as adjunct therapy and those with follow-up of less than 2 years were excluded.
Results
Ten randomized controlled trials met the inclusion criteria: five compared unilateral with bilateral instrumentation using open transforaminal or posterior lumbar interbody fusion (TLIF/PLIF), one used open posterolateral fusion, and four used minimally invasive TLIF/PLIF. There were no significant differences between unilateral and bilateral screw instrumentation with respect to nonunion, low back or leg pain scores, Oswestry Disability Index, reoperation, or complications.
Conclusions
The existing literature does not identify significant differences in clinical outcomes, union rates, and complications when unilateral instrumentation is used for degenerative pathologic conditions in the lumbar spine. The majority of published reports involve single-level lumbar unilateral instrumentation.
Study Rationale and Context
Unilateral instrumentation has been advocated as an alternative to bilateral instrumentation for spine fusion. The advantages touted include avoidance of soft tissue disruption on the contralateral side, reduced operation time, and lower implant costs. 1 , 2 , 3 However, the results of some studies suggest that unilateral instrumentation may result in nonunion, metal failure, pseudarthrosis, or cage migration due to the decreased strength or inherent asymmetry of this system. 1 , 4 Whether unilateral instrumentation is as efficacious and safe as bilateral instrumentation for spine fusion is debated.
Clinical Questions
What is the comparative efficacy of unilateral instrumentation compared with bilateral instrumentation in spine surgery?
What is the safety of unilateral instrumentation compared with bilateral instrumentation in spine surgery?
Materials and Methods
Results
We identified 10 randomized controlled trials that met the inclusion criteria, which form the basis for this report (Fig. 1). All were lumbar fusions for degenerative spinal disorders. A list of excluded studies can be found in the online supplementary material.
Five studies compared unilateral with bilateral instrumentation using open transforaminal or posterior lumbar interbody fusion (TLIF/PLIF), 6 , 7 , 8 , 9 , 10 one study used open posterolateral fusion, 3 and four used minimally invasive TLIF/PLIF 11 , 12 , 13 , 14 (Table 1).
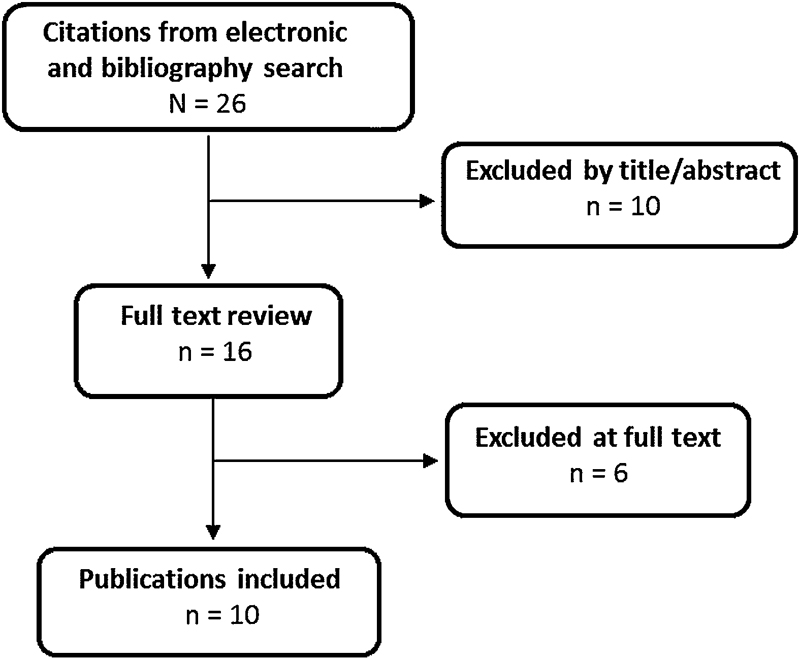
Flowchart showing results of literature search.
Demographics and characteristic of included studies
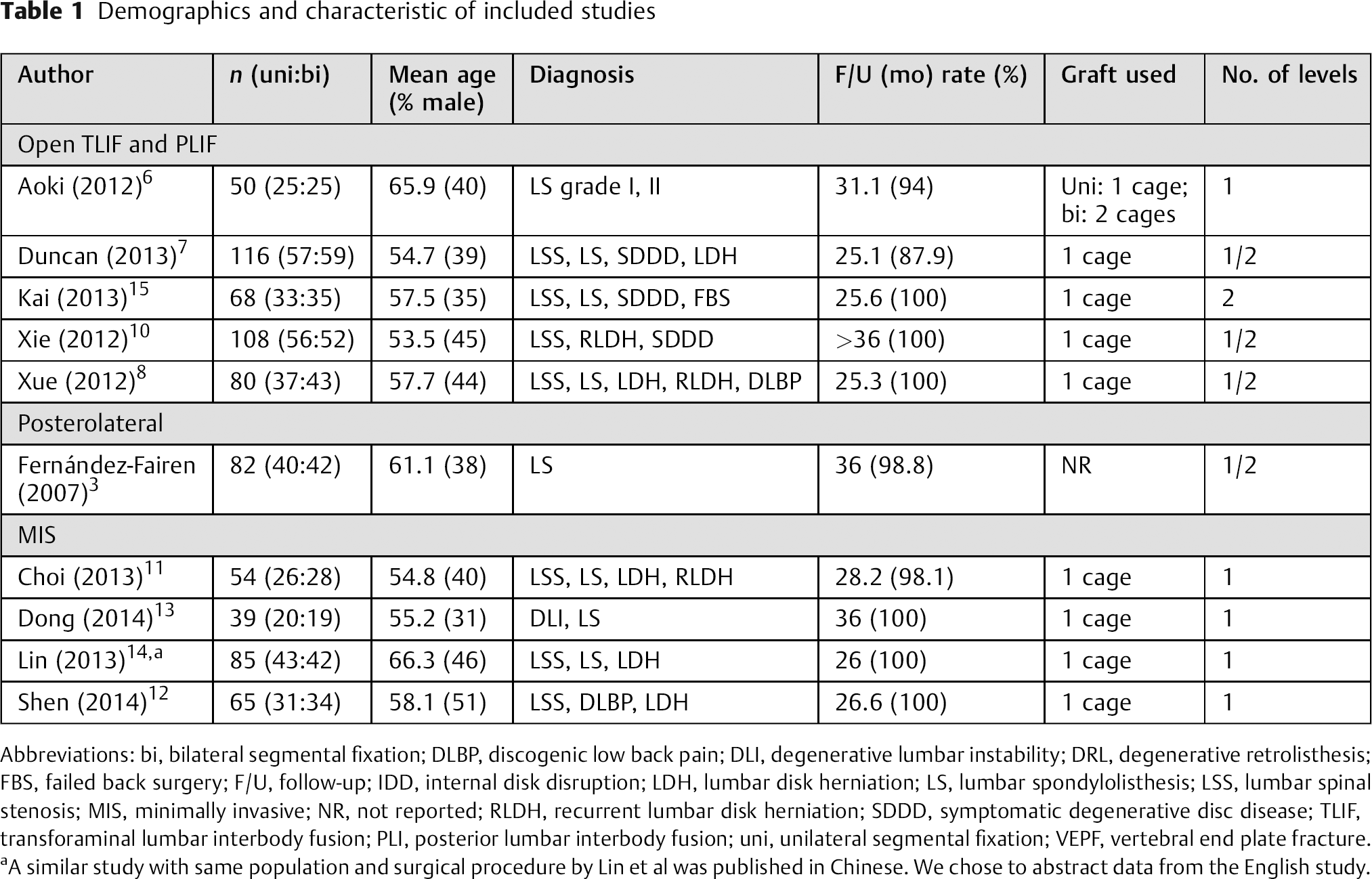
Abbreviations: bi, bilateral segmental fixation; DLBP, discogenic low back pain; DLI, degenerative lumbar instability; DRL, degenerative retrolisthesis; FBS, failed back surgery; F/U, follow-up; IDD, internal disk disruption; LDH, lumbar disk herniation; LS, lumbar spondylolisthesis; LSS, lumbar spinal stenosis; MIS, minimally invasive; NR, not reported; RLDH, recurrent lumbar disk herniation; SDDD, symptomatic degenerative disc disease; TLIF, transforaminal lumbar interbody fusion; PLI, posterior lumbar interbody fusion; uni, unilateral segmental fixation; VEPF, vertebral end plate fracture.
A similar study with same population and surgical procedure by Lin et al was published in Chinese. We chose to abstract data from the English study.
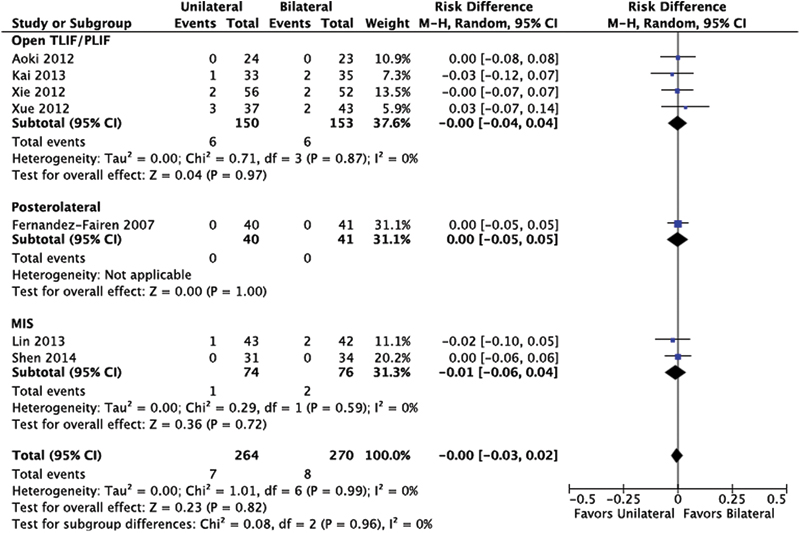
Nonunion
n = 8 studies.
There is no statistical difference of nonunion between unilateral and bilateral instrumentation, pooled risk difference, 0.01 (95% confidence interval [CI]: −0.01, 0.04). The results were similar across surgical procedure (open TLIF/PLIF, posterolateral, or minimally invasive [MIS]; Fig. 2).
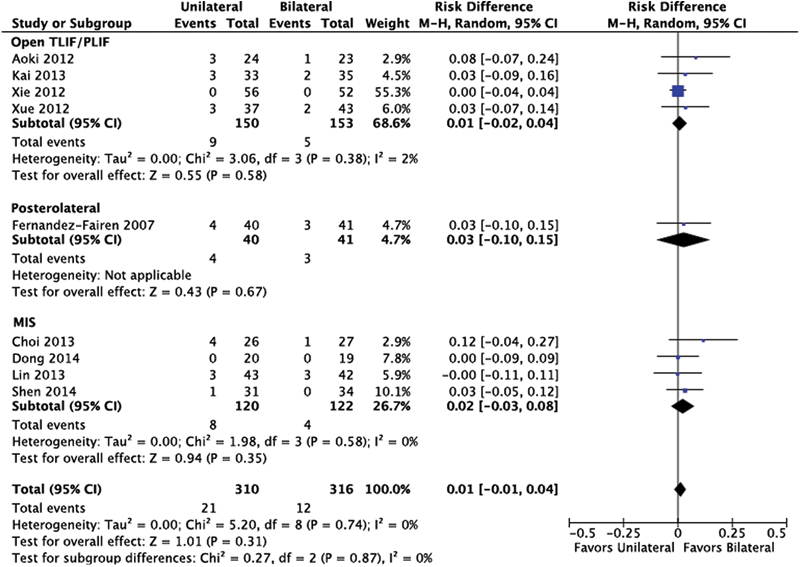
Nonunion. Abbreviations: CI, confidence interval; MIS, minimally invasive; M–H, Mantel-Haenszel; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion.
Patient-Reported and Clinical Outcomes
Low back pain (LBP), 10-point visual analog scale (VAS):
n = 7 studies.
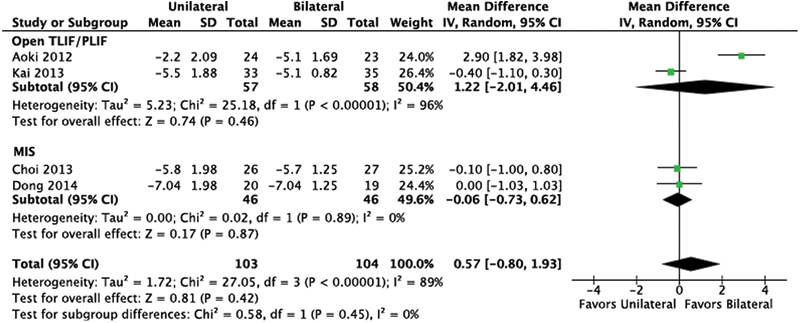
In studies where the surgical procedure was an open TLIF/PLIF, the VAS LBP score statistically favored bilateral instrumentation, though the difference was not considered clinically meaningful; mean difference (MD) between changed score was 0.71 (95% CI: 0.06, 1.36; Fig. 3). In studies using MIS, there was no statistical difference between unilateral and bilateral instrumentation.
Leg pain, 10-point VAS:
n = 4 studies.
No statistical difference between the procedures was found when doing open TLIF/PLIF or MIS (Fig. 4).
Oswestry Disability Index (ODI):
n = 5 studies.
There was no statistical difference in mean ODI scores between unilateral and bilateral screw instrumentation (Fig. 5).
Japanese Orthopaedic Association (JOA) score:
n = 3 studies.
The JOA scores were better in the bilateral screw instrumentation group, with pooled MD of 0.85 (95% CI: 0.08, 1.61; Fig. 6).
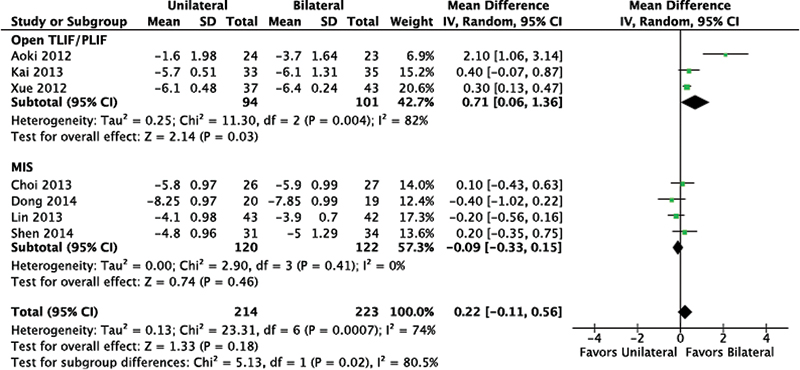
Low back pain. Abbreviations: CI, confidence interval; IV, inverse variance; MIS, minimally invasive; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion; SD, standard deviation.
Leg pain. Abbreviations: CI, confidence interval; IV, inverse variance; MIS, minimally invasive; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion; SD, standard deviation.
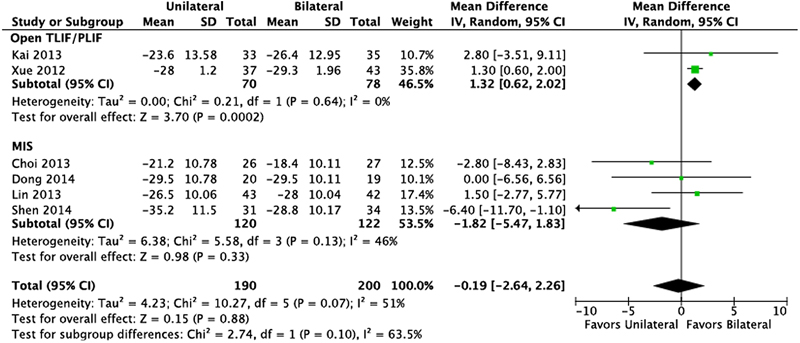
Oswestry Disability Score. Abbreviations: CI, confidence interval; IV, inverse variance; MIS, minimally invasive; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion; SD, standard deviation
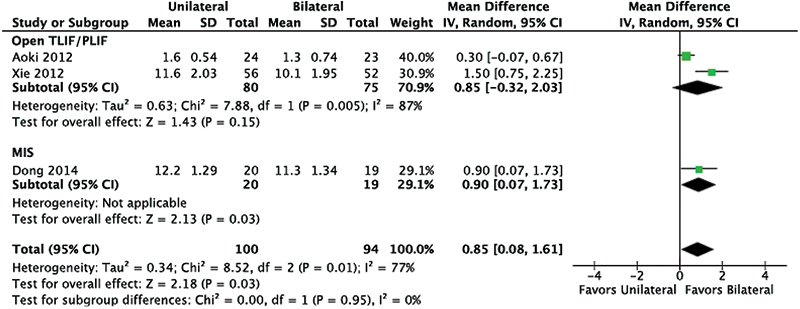
Japanese Orthopaedic Association Score. Abbreviations: CI, confidence interval; IV, inverse variance; MIS, minimally invasive; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion; SD, standard deviation.
Complications
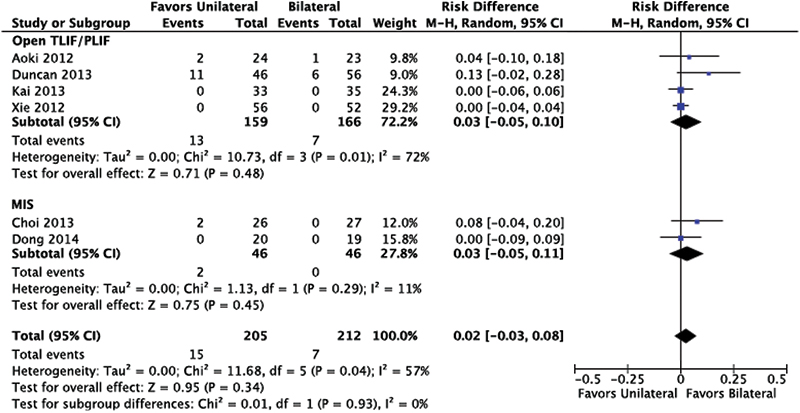
Reoperation:
n = 2 studies.
No statistical difference was found between unilateral and bilateral screw instrumentation (Fig. 7).
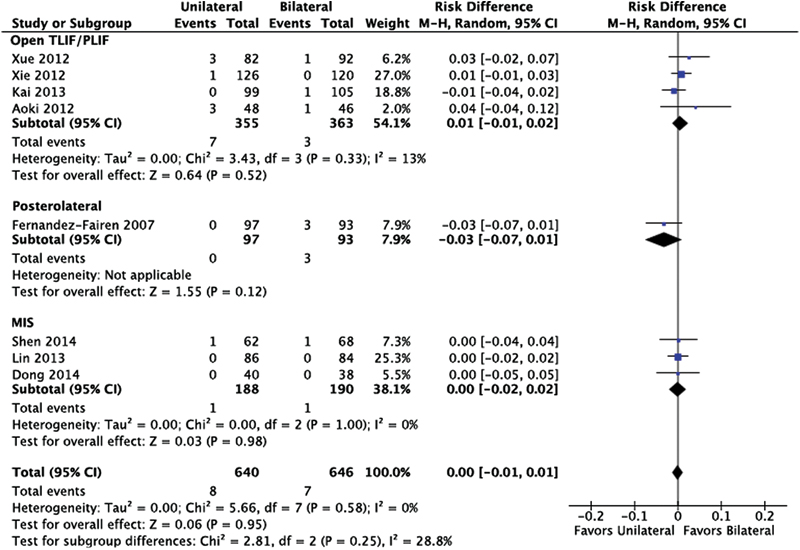
Infection:
n = 6 studies.
There was no statistical difference in the risk of infection between unilateral and bilateral screw instrumentation (Fig. 8).
Cage migration:
n = 3 studies.
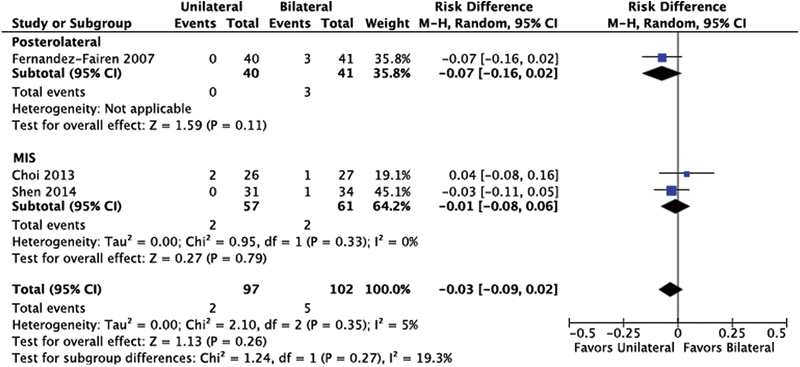
No statistical difference was found between unilateral and bilateral screw instrumentation (Fig. 9).
Screw failure:
n = 8 studies.
There was no statistical difference between unilateral and bilateral screw instrumentation (Fig. 10).
Other complications:
n = 8 studies.
There was no statistical difference between unilateral and bilateral screw instrumentation (Fig. 11). Pooled results in open TLIF/PLIF suggest a slightly lower but nonstatistically significant risk of other complications favoring the unilateral instrumentation. Those other complications include pulmonary embolism (n = 1), deep vein thrombosis (n = 1), dural sac laceration (n = 7), postoperative proximal scoliosis (n = 1), transient motor weakness (n = 2), and cerebral spinal fluid leak (n = 2).
Reoperation. Abbreviations: CI, confidence interval; MIS, minimally invasive; M–H, Mantel-Haenszel; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion.
Infection. Abbreviations: CI, confidence interval; MIS, minimally invasive; M–H, Mantel-Haenszel; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion.
Cage migration. Abbreviations: CI, confidence interval; MIS, minimally invasive; M–H, Mantel-Haenszel; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion.
Screw failure. Abbreviations: CI, confidence interval; MIS, minimally invasive; M–H, Mantel-Haenszel; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion.
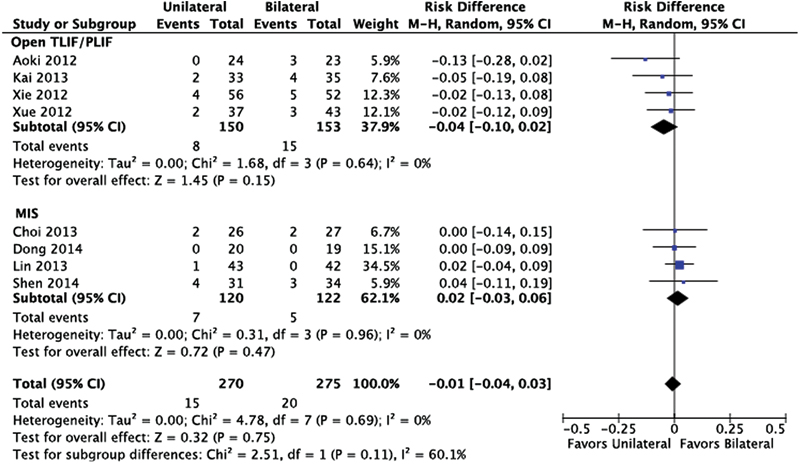
Other complications. Abbreviations: CI, confidence interval; MIS, minimally invasive; M–H, Mantel-Haenszel; TLIF/PLIF, transforaminal or posterior lumbar interbody fusion.
Evidence Summary
There was no difference in nonunion, low back or leg pain, ODI, reoperation, infection, cage migration, screw failure, or other complications comparing unilateral with bilateral screw instrumentation. The overall strength for these findings are considered low or very low (Table 2).
Strength of evidence summary
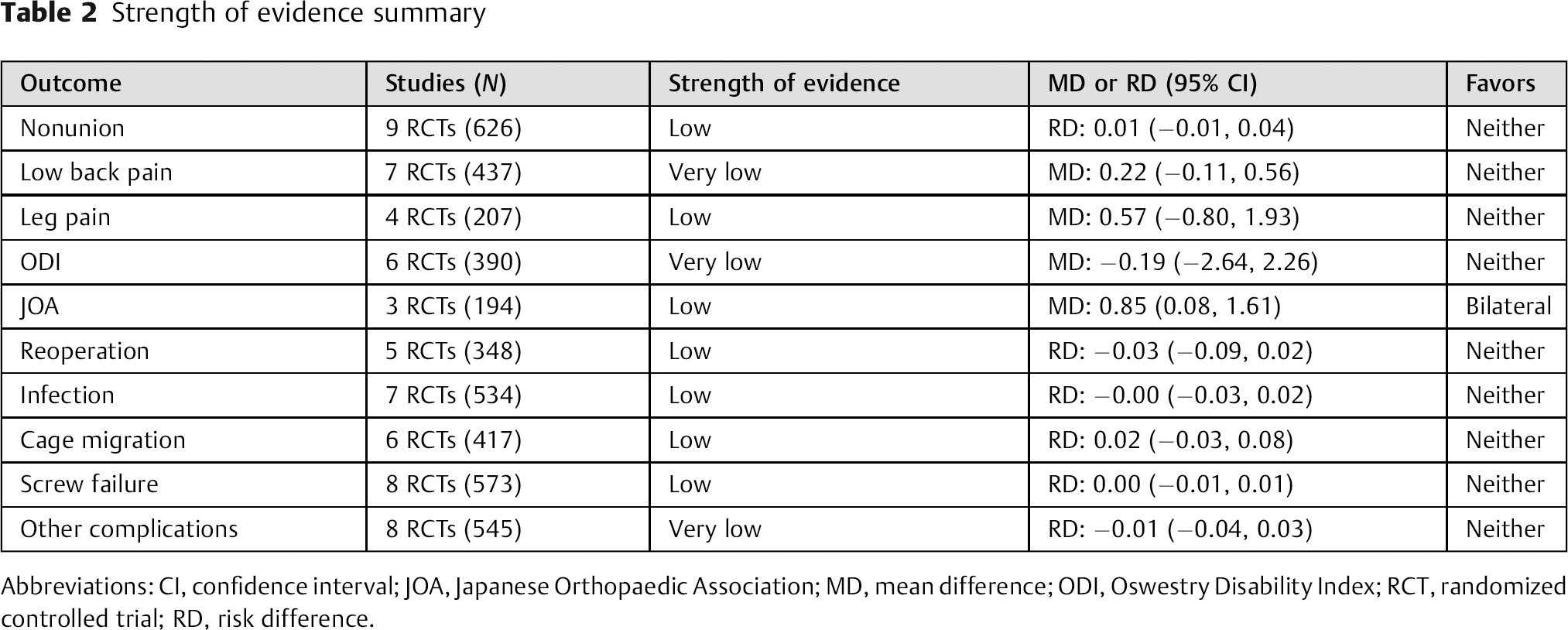
Abbreviations: CI, confidence interval; JOA, Japanese Orthopaedic Association; MD, mean difference; ODI, Oswestry Disability Index; RCT, randomized controlled trial; RD, risk difference.
Clinical Guidelines
None found.
Illustrative Case
A 69-year-old man had chronic back and bilateral leg pain. The patient's pain was refractory to conservative measures over a 2-year period. He had physical therapy, medications, and epidural steroid injections without significant long-term relief of symptoms.
The preoperative radiographs showed L4–L5 grade 1 degenerative spondylolisthesis (Fig. 12A, B). The preoperative magnetic resonance imaging demonstrated L4–L5 low-grade degenerative spondylolisthesis with severe spinal stenosis (Fig. 12C, D).
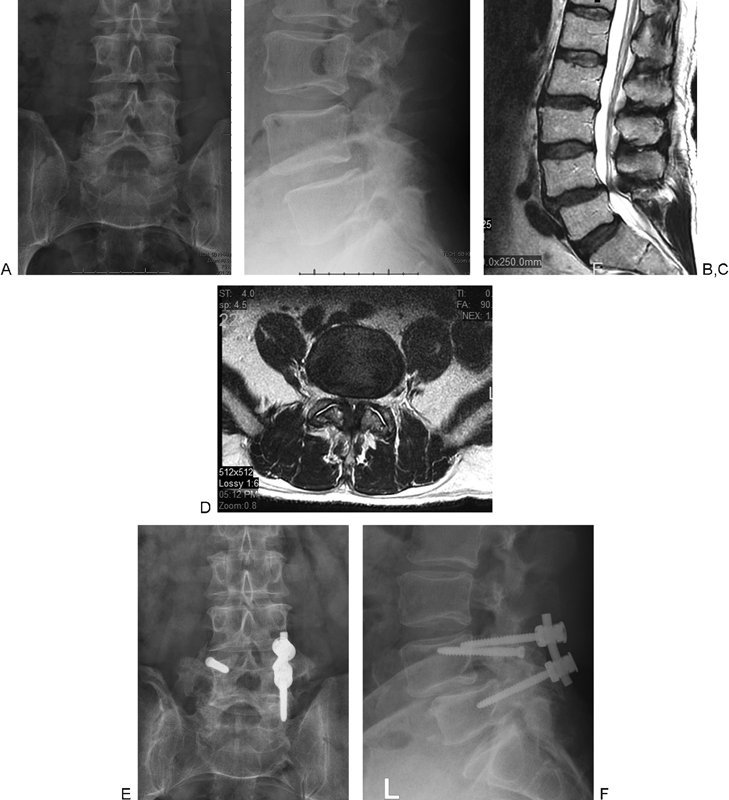
Preoperative radiographs show L4–5 grade 1 degenerative spondylolisthesis (A, B). Preoperative magnetic resonance imaging demonstrates L4–5 low-grade degenerative spondylolisthesis with severe spinal stenosis (C, D). Three-year postoperative anteroposterior and lateral radiographs demonstrating solid bilateral fusion without loosening of unilateral fixation (E, F).
The patient had L4–L5 decompression and fusion surgery. His surgical procedure was complicated by the inability to successfully place his left L5 pedicle screw. The left L4 screw was intentionally left in place, and right-sided unilateral fixation was performed along with bilateral posterolateral iliac crest bone grafting.
The 3-year postoperative anteroposterior and lateral radiographs (Fig. 12E, F) demonstrated solid bilateral fusion without loosening of unilateral fixation. There was a slight progression of the spondylolisthesis when compared with the preoperative standing radiographs. The patient reported minimal back pain and improved function at 3-year follow-up.
Discussion
Strengths:
Several randomized controlled trials assessing the treatment options allowed for meta-analysis stratified by type of surgery.
Limitations:
Important outcomes were included inconsistently among studies resulting in small sample sizes for some outcomes. The outcomes that occurred infrequently resulted in low power to detect statistical differences (see the online supplementary material).
A serious risk of bias was present in all included studies. The indication of concealed allocation was not reported in any trial; blinding of evaluators occurred rarely; and 6 of 10 studies did not compare patients at baseline to ensure similar distribution of prognostic factors.
This systematic review highlights the paucity of decent literature involving the efficacy of unilateral instrumentation in lumbar spinal surgery. A total of 10 studies met the inclusion criteria for this report. All the studies involved degenerative pathology in the lumbar spine. The vast majority of procedures were single-level fusions for degenerative disk disorder or degenerative spondylolisthesis.
Examination of the existing literature does not reveal significant differences in the patient outcomes between unilateral and bilateral fixation when performed for lumbar spinal pathology. A serious risk of bias exists in all the included studies resulting in an overall strength for these findings as either low or very low.
The reported fusion rates with either unilateral or bilateral fixation are high, without a significant difference. The rates of instrumentation failure and nonunion were similarly low.
The reported functional outcomes including ODI, VAS, and leg pain scores were not different between unilateral and bilateral fixation cases.
The existing literature does not demonstrate outcome differences for MIS patients having either unilateral or bilateral lumbar fixation.
The complication rates remain low with both unilateral and bilateral fixation for lumbar degenerative pathology.
The theoretical advantages of unilateral fixation are many and include shorter operative times and reduced blood loss. The operative costs for implants are also reduced. From a technical standpoint, unilateral fixation cases do involve the utilization of less surgical resources. The degree of diminished segmental stability achieved with unilateral fixation did not appear to lead to worse outcomes or higher complication rates for single-level degenerative cases.
We have demonstrated that there appears to be equivalency between unilateral and bilateral fixation when performed in adult patients who do not have significantly unstable lumbar conditions. It is important to emphasize that successful clinical and radiographic outcomes for unilateral fixation in patients with highly unstable lumbar conditions have not been described in this review. It is our opinion that additional prospective comparative studies are needed to better define the role of unilateral instrumentation in the treatment of lumbar spinal disorders.
Conclusions
The existing literature does not identify significant differences in clinical outcomes, union rates, and complications when unilateral instrumentation is used for degenerative pathologic conditions in the lumbar spine. The majority of published reports involve single-level lumbar unilateral instrumentation.
Disclosures
Robert W. Molinari, none
Ahmed Saleh, none
Robert Molinari, Jr., none
Jeff Hermsmeyer, none
Joseph R. Dettori, none
All reviewers unanimously congratulate the authors in selecting a topic that questions conventional wisdom—more specifically, the need to use bilateral versus unilateral segmental fixation in form of pedicle screw/rod constructs to achieve fusion for single-level (monosegmental) arthrodesis procedures. The question of how much pedicle screw fixation is really needed to achieve a solid fusion in a stable single segment lumbar spine has been associated with divisive arguments from both sides, along with poignant arguments made from both sides. Shorter surgery, lower hardware insertion-related complication rates, and reduced implant costs are certainly strong arguments in favor of unilateral fixation for lumbar fusion. But where does one draw the line to the counterargument that unilateral instrumentation may be favored out of an economic gains motivation?
This enclosed systematic review offers an unprecedented overview on this topic and the findings—not surprisingly—are less than conclusive. The authors stressed two important factors: (1) the sample sizes were very small, thus opening the door for a type II error, and (2) due to the data reporting, Molinari et al were unable to provide a power calculation. The other consideration lies in the apparent and substantial selection bias commonly practiced in the source studies. In addition to the factors mentioned in the article, lumbar segmental stability and deformity correction, iatrogenic destabilization or variations in bone density were variables not really addressed by the source publications, thus adding more confounding factors to attempts at a definitive comparison. The use of recombinant bone substitutes in MIS constructs may add further confusion as the dosing and application strategy can influence healing results. That said, the available comparison data for the most part does not suggest any substantial difference in patient safety or reported outcomes, thus opening the door for further discussion. This leaves us as clinicians with an important question that remains to be answered. For the clinical setting of a fusion to be performed in an inherently stable single degenerative lumbar spine segment, is a unilateral instrumentation an acceptable primary stabilization strategy or should we use the information gleaned from the preceding systematic review as an assurance that unilateral segmental instrumentation is sufficient in patients where bilateral instrumentation has for some reason not worked out? This important differentiation at this time is not resolvable. EBSJ invites further commentary from its global readership.
On a side note, the example chosen as an illustrative case was critiqued by our reviewers for several reasons. The case denotes an “accidental unilateral fixation”—one where a planned bilateral instrumentation was abandoned due to technical difficulties. The underlying pathology (an unstable-appearing degenerative spondylolisthesis) would clearly not be an ideal situation for unilateral fixation by any of the inclusion criteria of the studies used for this comparison. The report that the patient fused despite unilateral fixation also underscores the potential for bias in results reporting. It can be very challenging to establish a firm fusion in the lumbar spine in the presence of posterolateral fusions without interbody grafts and in the absence of hardware failure. In this patient, the spondylolisthesis clearly slipped more compared with the preoperative images, thus calling into question the assurance that an uneventful fusion resulted from the unilateral instrumentation. The symptom relief of the patient may have been mainly influenced by an effective stenosis decompression, and the back pain relief may have been secondary to that circumstance alone and may have nothing to do with a fusion or instrumentation. EBSJ would also like to point out that it does not endorse leaving an isolated screw without fixation purpose behind.
Finally, the reviewers recommended the readership take a look at the Web-based supplemental materials due to their depth and quality. EBSJ thanks the authors for their hard work on this topic.
Footnotes
Acknowledgments
Analytic support for this work was provided by Spectrum Research, Inc. with funding from AOSpine. Special thanks to Mark Junge for his assistance in producing the figures for the meta-analysis.