
Abstract
Objective
To investigate the different clinical characteristics of minimally invasive transforaminal lumbar interbody fusion on treatment of lumbar spondylolisthesis combined with severe narrowing of the intervertebral space or simple grade II lumbar spondylolisthesis.
Methods
Thirty-eight patients were divided into groups A (16 cases combined with severe intervertebral space narrowing) or B (22 cases of simple grade II lumbar spondylolisthesis without intervertebral space narrowing). Differences in preoperative preparation, operation time, blood loss, tool selection, decompression, reduction, pedicle screw, cage size selection, and other aspects were compared. The Visual Analogue Scale (VAS) and Japanese Orthopaedic Association (JOA) scores were used to assess the effect of treatment.
Results
The operation time was significantly longer, blood loss was greater, the anatomical reduction rate was lower, and cage size was smaller in group A than in group B. Furthermore, special tools were required for treating the lumbar intervertebral space and the pedicle screws were different between the groups. JOA and VAS scores were similar between the groups
Conclusions
Cases of severe intervertebral space narrowing need to be fully released, with bilateral decompression, and special intervertebral processing tools need to be prepared. Long pedicle screws are conducive to connecting the rod and reducing slippage.
Keywords
Introduction
Lumbar spondylolisthesis is a common degenerative disease in spinal surgery. Symptoms of patients with lumbar spondylolisthesis are mainly derived from nerve root compression and some patients require surgery for decompression. Conventional open lumbar surgery performed via the posterior approach is associated with significant soft tissue morbidity, which can adversely affect patients’ outcomes. 1 Since minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) was first reported in 2003, an increasing amount of spinal surgeons have adopted this approach to treat lumbar spondylolisthesis.2–5 This approach has advantages and clinical outcomes are encouraging compared with traditional open lumbar operations.2–5 Lumbar spondylolisthesis combined with severe narrowing of the intervertebral space is a complex degenerative spinal disease that is accompanied by a long operation time and a lot of blood loss. The present study aimed to examine the characteristics of this disease when treated by MIS-TLIF.
Materials and methods
This study was conducted in accordance with the declaration of Helsinki. This study was performed with approval from the Ethics Committee of China-Japan Union Hospital of Jilin University. Written informed consent was obtained from the participants.
Clinical data and observation indices
Patients who were diagnosed with grade II (Meyerding Grading System) lumbar spondylolisthesis at the L4/5 and L5/S1 levels from July 2009 to June 2013 were included in the present study. Thirty-eight patients with lumbar spondylolisthesis who were treated by MIS-TLIF were divided into groups A and B. Group A included cases of grade II lumbar spondylolisthesis combined with severe narrowing of the intervertebral space (Figure 1) in which the intervertebral height was <2 mm, as measured by a computed tomography (CT) scan or X-ray. Group B included cases of simple grade II lumbar spondylolisthesis without narrowing of the intervertebral space. All patients in both groups underwent MIS-TLIF, which was performed by the same two surgeons who preferred a minimally invasive approach under the Mast Quadrant System (Medtronic, Minneapolis, MN, USA). Differences in preoperative preparation, operation time, blood loss, tool selection, decompression, reduction, type of pedicle screw, cage size selection, and other aspects were compared. Furthermore, the Visual Analog Scale (VAS) and Japanese Orthopaedic Association (JOA) scores were used to assess the treatment effect. All patients were followed up for more than 1 year.

Preoperative (left) and postoperative (right) X-rays of lumbar spondylolisthesis with severe narrowing of the intervertebral space.
Operation
Lumbar spondylolisthesis was treated at the L4/5 levels. The procedures for group A were as follows. Patients were placed in the prone position on the operation table and intraoperative fluoroscopy was used to identify the operative level. The Wiltse approach was adopted on the uninjured side. Paramedian, longitudinal, 3- to 4-cm incisions were made on the lateral borders of the facet joints of the spinal level, as visualized on fluoroscopy. The skin and subcutaneous tissues were cut by layers. The surgeon entered through the gap between the multifidus and longissimus, installed the quadrant channel to the intervertebral space at the levels of L4/5, and the joint facets were exposed under the quadrant channel. Fibrous tissue was then removed, the insertion point and insert positioning pin were determined, and pin bone wax was temporarily closed. Part of the L5 facet, L4 facet, and L4 lamina were removed and prepared for intervertebral bone grafting. The ligamentum flavum was visualized and removed in a piecemeal fashion, and both the exiting and traversing nerve roots were decompressed and protected. Because of L4 forward slip and narrowing of the intervertebral space, precisely defining the intervertebral space was difficult (Figure 2). A thin bone knife was used to determine the inferior border of L4 and open the fibrous ring to handle the L4/5 intervertebral space (Figure 2). Different sizes of disc space shavers were adopted to perform complete discectomy, and a ring curette was used to remove the cartilaginous endplate (Figure 2). Long-arm pedicle screws were inserted into the L4 and L5 levels. L5 was used for the fixing screw, while L4 was used for the active screw (Figure 3). Fluoroscopy confirmed whether the position of the screw was good and not connected to the bar, and whether the gauze packed the surface. The same method was used for the affected side. Furthermore, a mixture of autografts from the facet joint in the disc space was anteriorly placed. A polyether ether ketone interbody cage (large, 8 × 26 mm) was packed with the autografts and inserted into the disc space, and fluoroscopy was used to ensure satisfactory placement. Once interbody fusion was performed, pedicle screws were placed into the L4 and L5 levels. Compression was applied before final tightening, all wounds were copiously irrigated, and the wounds were closed in layers. A pulling rod finished the reduction and fixation, and a drainage tube was assembled to suture the wound.

Preoperative (left) and postoperative (right) X-rays of lumbar spondylolisthesis without severe narrowing of the intervertebral space.

A normal pedicle screw (left) and a long pedicle screw (right). Long pedicle screws were used for good reduction of spondylolisthesis. The left panel shows a normal pedicle screw and the right panel shows a long pedicle screw.
The procedures for group B were as follows. Similar to the approach in group A, decompression was first performed, but comprehensive soft tissue release was not carried out. The intervertebral space and implanted autologous bone were then dealt with as described for group A. An appropriately sized cage (usually 9 × 26 mm) filled with autologous bone was placed, reduction and fixation were performed, the drainage tube was installed, and the suture was cut. The healthy side did not undergo decompression. After X-ray positioning, pedicle screws were placed through percutaneous puncture fixation.
Statistical analysis
Parametric data are presented as mean ± standard deviation. The t-test and χ2 test were used to assess statistical significance between the groups for each follow-up using SPSS 13.0 software (SPSS Inc., Chicago, IL, USA). A P value of <0.05 was considered statistically significant.
Results
Group A included 16 cases (L4/5, 10 cases; L5/S1, 6 cases) and group B included 22 cases (L4/5, 14 cases; L5/S1, 8 cases; Figure 1). The mean age of patients in group A was 57.81 ± 10.13 years and that in group B was 59.73 ± 9.26 years. These two groups had a similar age and sex distribution, vertebral level, and disease history (Table 1). All patients in group A were bilaterally decompressed, while all patients in group B were unilaterally decompressed. Patients in group A required a significantly longer operation time (P<0.001), had more blood loss (P<0.001), and used a smaller cage size (P<0.05), but the anatomical reduction rate was lower (P<0.05) compared with those in group B (Table 2). Furthermore, there was a need for special tools that were indispensable for treating the lumbar intervertebral space in Group A. The VAS and JOA scores were not significantly different between the two groups (Table 3).
Patient data.

Values are mean ± standard deviation or number. There were no significant differences in variables between the two groups.
Comparison of perioperative indices of groups A and B.
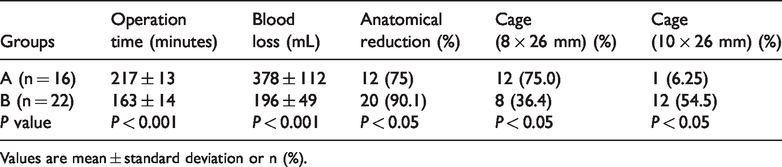
Values are mean ± standard deviation or n (%).
VAS and JOA scores preoperatively and at the final FU.

Values are mean ± standard deviation. VAS: Visual Analogue Scale; JOA: Japanese Orthopaedic Association; FU: follow-up.
Discussion
Less than grade II lumbar spondylolisthesis is one of the indications of MIS-TLIF, 2 regardless of degenerative spondylolisthesis and a fissure in the isthmus with spondylolisthesis.3,4 MIS-TLIF has a number of advantages, such as less blood loss, less soft tissue trauma, less related complications, and early off-bed activity, compared with the traditional posterior approach for open lumbar surgery. MIS-TLIF is continuously becoming more popular among spinal surgeons.5–7 Generally, less than grade II lumbar spondylolisthesis treated by MIS-TLIF only requires unilateral decompression. This leads to blood loss of <100 mL and enables reductions to be easily performed. Furthermore, several studies have reported that treatment costs for MIS-TLIF are lower compared with traditional posterior lumbar interbody fusion surgery.8–10 However, in our study, the operation time was significantly longer, blood loss was greater, and the reduction rate was lower in group A (lumbar spondylolisthesis combined with severe narrowing of the intervertebral space) compared with group B (simple lumbar spondylolisthesis) (Table 2). These findings suggest that surgeons should be fully prepared in the preoperation period. Furthermore, lumbar spondylolisthesis combined with severe narrowing of the intervertebral space is more difficult to treat compared with simple conditions.
Lumbar spondylolisthesis combined with severe narrowing of the intervertebral space requires bilateral decompression, the operation time is always prolonged, and intraoperative bleeding may be longer than usual. Therefore, preoperative positive blood preparation is essential. Furthermore, there is difficulty for routine tools to enter a narrow intervertebral space (Figure 2). Therefore, a special thin bone knife and tools for treating the intervertebral disc are essential (Figure 2). During the operation, this type of problem is always encountered, the intervertebral space is hard to confirm, and tools are usually incorrectly inserted into the upper vertebrae because of the narrow space and vertebral forward slip (Figure 2). However, C-arm X-ray fluoroscopy can favorably solve this issue. Good reduction can be obtained through long-arm pedicle screws, when the sides of the facets are resected, the soft tissue is fully released, and the intervertebral space is sufficiently braced (Figure 2). A universal distal screw is not favorable. For osteoporotic patients, nerve root release is a priority, rather than anatomical reduction, because pulling reduction is difficult to perform (Figure 4). In consideration of narrowing of the intervertebral space, a smaller cage was chosen for patients in group A. This was because the bone graft was relatively small and autologous bone could be implanted in the intervertebral space. Patients in group A required a longer operation time and had more blood loss because of bilateral decompression. In group B, anatomical reduction was achieved under unilateral decompression and a reduction in pulling out of pedicle screws, in which the operation time and blood loss were greatly improved. The JOA and VAS scores were similar between the two groups. This indicated that the MIS-TLIF operation had an excellent therapeutic effect on these two types of lumbar spondylolisthesis.

Treatment procedures of the intervertebral space in lumbar spondylolisthesis with severe narrowing of the intervertebral space. (a) The intervertebral space was narrow. A thin tool was used to find this space. (b and c) After the intervertebral space was found, a special tool was used to deal with the disc. Attention was paid so that this tool did not enter the body of the vertebra near the intervertebral space.
The intervertebral spaces for patients in group A were narrow, and the reduction rate was low, which also caused the intervertebral foramina to be narrow and the bilateral exit nerve roots to be compressed. Therefore, bilateral decompression was required. The decompression method is mainly determined by the degree of spinal stenosis. However, commonly, lumbar spondylolisthesis combined with severe narrowing of the intervertebral space has severe spinal stenosis compared with that without severe narrowing of the intervertebral space. Previous studies have shown that bilateral decompression has better clinical outcome scores than unilateral decompression.11,12 Full decompression is the primary condition for eliminating clinical symptoms. Ample release is the premise of intervertebral space distraction and a guarantee of a reduction in spondylolisthesis. A long pedicle screw is favorable in the vertebral slip reduction process.13,14 Although MIS-TLIF requires a relatively long-term learning curve,15,16 this operation has many clinical advantages for treating lumbar spondylolisthesis. Many studies have shown that technical proficiency in MIS-TLIF is achieved after 44 surgeries, and patients benefit from a shorter operative duration and radiation, less pain, and more relief in their back, legs, and neurogenic symptoms. 17 The MIS-TLIF approach is a technically difficult procedure for practicing spinal surgeons regarding intra- and perioperative parameters of surgical time, estimated blood loss, intravenous fluid, and duration of anesthesia. Operative time and proficiency improve with proficiency of this minimally invasive technique. 15 MIS-TLIF has a good effect in treating the two types of lumbar spondylolisthesis, but the operation of lumbar spondylolisthesis with severe narrowing of the intervertebral space remains complicated, and is different from simple spondylolisthesis. All cases of severe intervertebral space narrowing need to be fully released and bilaterally decompressed, and there is a need to prepare special intervertebral processing tools and use long pedicle screws, which are conducive for connecting rods and reducing slippage.