
Abstract
Study Design
Case report.
Objective
Sacral fractures, traumatic or atraumatic, are a rather rare cause of low back pain. The majority of the cases of pregnancy-related sacral fractures are reported as a postpartum complication, and only few cases of sacral atraumatic fractures have been reported in the last trimester of the pregnancy. The aim of this study is to report a rare case of atraumatic sacral fracture in the third trimester of pregnancy.
Methods
We report the case of a 30-year-old Caucasian European woman during her 37th week (36 weeks and 4 days) of gestation, who complained during her scheduled obstetric examination of continuous low back pain with no associated history of trauma. The patient performed activities of daily living with a normal level of fatigue and reported no running or walking long distances. She was examined in our department, and a magnetic resonance imaging scan was performed that showed a vertical nondisplaced fracture in her left sacrum.
Results
The patient was treated conservatively, and analgesics were administrated according to the consensus of the orthopedic and the anesthesiology departments. No further complications were recognized in the remaining period of her pregnancy, and a healthy child was born by caesarean section.
Conclusions
Atraumatic fractures of the sacrum should be included in the differentiated diagnosis of pregnant patients with low back pain.
Introduction
Every year, a large number of patients present in the emergency department with low back pain. Fractures of the sacrum appear with a low incidence in these patients, with sacrum stress fractures even rarer. They are more commonly recognized in athletes, especially long-distance runners. 1 , 2 , 3 , 4 Many conjectures have been made regarding the pathology of these fractures, with the most relevant being weakened bone or unusual loads that the normal bone is able to withstand. 5 The high loads applied after birth are responsible for those fractures that are more common in the postpartum period. 6 , 7 , 8 , 9 Plain radiographs cannot be performed during the pregnancy; therefore, magnetic resonance imaging (MRI) is the gold standard for diagnosis. Most commonly, a vertical shear in the sacrum is recognized with osseous edema in the surrounding tissues.
In the majority of the cases, the fracture is treated conservatively with immobilization, manual therapy, hydrotherapy, and analgesics, which are used with great caution due to the drug interactions with the fetus. 10 Pain control is extremely difficult in these patients; therefore, epidural catheters are used in some cases. The purpose of this study is to report an extremely rare case of prepartum sacral stress fracture (only two prepartum sacral stress fractures are described in the literature), 7 , 10 which was treated conservatively with great effort for adequate pain control and delivery of a healthy newborn.
Case Report
A 30-year-old patient who was 36 weeks and 4 days pregnant was referred by the obstetrics for low back pain that started ∼1 week prior. She reported discomfort and pain during activities of daily living beginning 7 days before her scheduled examination by her obstetrician. The pain was exacerbated while bending or walking. Application of heat in the area, together with hydrotherapy, reduced the pain and the feeling of discomfort.
The patient reported exercising for 1 hour of swimming or 1 hour of dancing three times every week. She was a nonsmoker. She reported only the use of paracetamol for the management of the pain in her back and that she had gained 5,500 g during her pregnancy.
The examination by the obstetric physician revealed a 2,850-g healthy fetus. The patient's laboratory values were within normal limits. The abdominal ultrasonography revealed no signs of any pathology. A Doppler ultrasound was also undertaken to exclude deep vein thrombosis and was negative.
The patient reported pain at the posterior iliac spine and had positive Gaenslen and Patrick tests. The clinical examination revealed pain after applying pressure over the sacral sulcus. Pain was also reproduced with pressure over the iliosacral joint.
Due to the presence of the gestation, MRI was performed and a vertical shear in the patient's left sacrum was recognized. Osseous edema was also present around the nondisplaced fracture (Fig. 1).
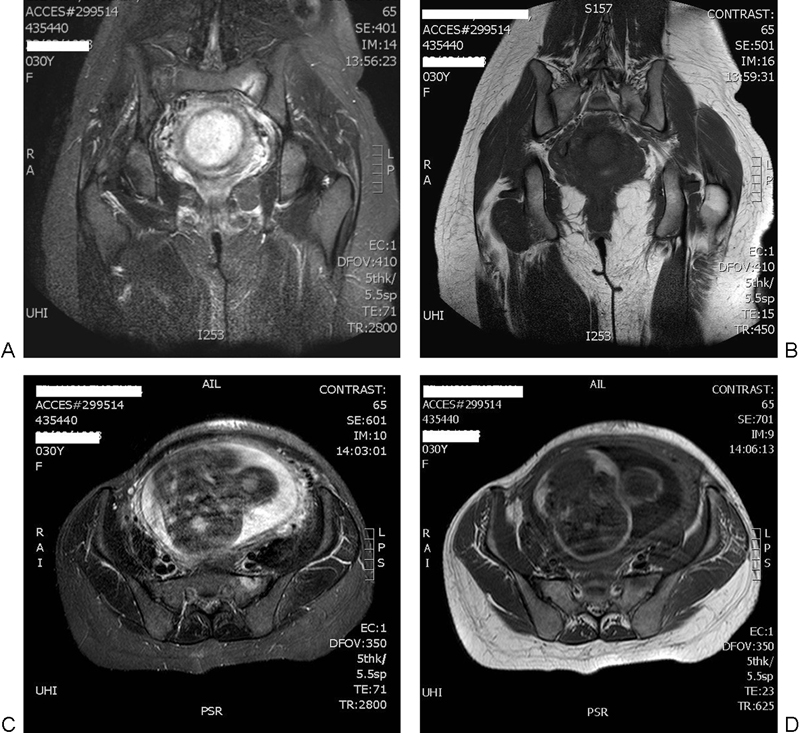
(A–D) Magnetic resonance images reveal a vertical shear fracture in the patient's left sacrum and osseous edema in the surrounding tissues.
Taking into consideration the risks of the displacement of the fracture due to the increased tension in the pelvis during a normal vaginal delivery, we recommended the delivery of the fetus by cesarean section. After the cesarean section, the patient started to mobilize with short walks under oral analgesics. Successful healing of the fracture was obtained after 4 months.
Discussion
Atraumatic fractures of the sacrum are an extremely rare medical entity, which is mostly diagnosed in runners. 3 Only nine cases of postpartum sacral stress fractures have been reported in the literature. 11 In the majority of the cases, the patient's bone density was within normal limits; therefore, the etiology of the fractures remained obscure. 11 , 12 Nevertheless, only two cases of stress sacral fracture have been reported in the prepartum period. 7 , 10
Usually, affected patients report pain in the lower back, the sacroiliac region, the buttocks, or the groin that does not resolve with common analgesics. During the clinical examination, positive Gaenslen and Patrick tests are often reported. In most of the cases, a normal bone density is found, a fact that is in accordance with the extremely low incidence of pregnancy-related osteoporosis (∼0.4 patients per 100,000 women) that is noted in the third trimester of the pregnancy. 13
Plain radiographs are often normal with positive findings in only 2 of 27 cases and should not be used due to the fact that the unborn child is exposed to unnecessary radiation. 2 MRI is the gold standard in imaging of these fractures because the fetus is not exposed to radiation and the extent of the injury is reported with great detail. The majority of the patients are found to have a vertical fracture of the sacrum with surrounding bone edema in the MRI. 1 , 2 , 5
For the evaluation of bone density of women with sacral fractures, postpartum bone density can be measured to assess for pregnancy-related osteoporosis. 13 Most often, osteoporosis is described in the third trimester of pregnancy. In most cases, bone density returns to normal limits 5 to 10 years after delivery. 13 Apart from fractures in the sacrum, fractures in the hip, the proximal femur, or the vertebral bodies have been described.
Biomechanical changes have been documented during pregnancy, which lead to the closure of the sacroiliac joint (SIJ). Several factors can be responsible for compromising the stability of the SIJ, such as altered posture and load-bearing capacity, changes in ligamentous and joint capsule tension, altered muscle length, reduced muscle strength, and poor muscular coordination, to name just a few. 14 To compensate for the increased load, most mothers will adopt an exaggerated lumbar lordosis while standing. 15 As the lumbar spine moves into greater extension, the sacrum moves into greater nutation, 16 and as a result, the compression loads acting on the SIJ when in upright postures are increased.
Treatment options of fractures during pregnancy are very limited. Drugs should be used with caution and only in cases of severe pain because of the effects on the fetus according to the stage of the pregnancy. Also, the risk of preeclampsia should be considered to achieve a successful birth delivery. 10 The most common analgesic that can be safely used in all trimesters of pregnancy is oral paracetamol. Ibuprofen has been used by anesthesiologists for pain control but under a maximum daily dose of 1,600 mg. 10 In cases of severe pain, epidural anesthesia is recommended because of the less effective systemic side effects. 10
In most cases, patients return to their prior condition after 6 weeks with conservative treatment. In all cases, a high level of clinical suspicion is required and adequate pain control must be achieved for the best results and the quick return to activities of daily living.
Conclusion
Sacral stress fractures should be considered in the differential diagnosis of patients with low back pain during pregnancy. A high degree of clinical suspicion is essential for a proper and early diagnosis, and adequate pain control should be administered for the delivery of a healthy newborn by cesarean section.
Disclosures
Dionysios K. Giannoulis, none
Panagiotis Koulouvaris, none
Evgenia Zilakou, none
Dimitrios B. Papadopoulos, none
Marios G. Lykissas, none
Alexandros N. Mavrodontidis, none
The case report by Dr. Giannoulis and colleagues and the commentary by Professor Schildhauer touch upon two important aspects:
Diagnostic and therapeutic uncertainties continuing to surround sacral fractures
Clinicians’ unease regarding management of pregnant patients
It remains a continued reality of medical systems around the world that sacral fractures continue to be missed or patients with sacral pain experience delays in diagnosis to the point of experiencing full-fledged cauda equina syndrome without intervention. Of course hindsight is always golden, but sharpening our clinician's tools for risk assessment and teaching the principles of sacral fractures to medical trainees should not be unreasonable goals for a better future. For practitioners in charge of spine care, knowledge of sacral pathology should also be a foundational expectation. We have all the necessary diagnostic tools with plain radiographs, computed tomography, MRI, and radionuclide scans; we just need to know when to ask for them and how to process their information provided and then to act on findings we receive. Better knowledge of sacral fracture classifications and their implications is also desirable. 1 AOSpine International has assembled a group of experts to try to improve on the current state of sacral fracture classifications and will hopefully soon be able to provide us with a better-validated and easy-to-use system in the not too distant future.
When caring for pregnant patients with back problems, the state of spine practitioners around the world is probably still best described as “uneasy” relative to best diagnostic and therapeutic practices. The general care approach is usually to wait and see until such time that delivery is completed and then next steps can be taken. This case report underscores the difficulties pregnant women commonly experience regarding the diagnostic and therapeutic uncertainty of our medical community. EBSJ hopes that this article and the accompanying commentary will ignite the curiosity of our scientifically minded readership in investigating problems pregnant patients with serious back disorders sometimes face.