
Abstract
Study Design
Narrative review
Objectives
Multiple classifications have been proposed for sacral fractures since the last century. While initial classifications focussed on vertical and transverse fractures, the recent fracture classifications encompass all injury patterns. In 1990, Isler classified unilateral vertical sacral fractures based on its potential influence on lumbo-sacral joint (LSJ) stability.
Methods
We re-visited the original description of Isler’s classification of sacral fractures and subsequent studies that have cited it. We will further describe basic LSJ anatomy, evolution of sacral classification systems and the use of Isler’s classification system as it relates to LSJ instability and chronic low back pain.
Results
Isler described a subset of unilateral vertical sacral fractures where the fracture line exited medial or through the L5-S1 facet joint, based on radiographic review of 193 sacral fractures (incidence -3.5%). He stated that such a fracture should be recognised as it can impede hemi-pelvis reduction and can result in late LSJ instability. The article has been cited in 106 studies and only a few studies have described the incidence of this variant. Nevertheless, the injury is considered as an indication for surgical fixation.
Conclusion
A review of various classifications indicates that sacral fractures have three important bio-mechanical implications, namely, pelvic ring continuity (vertical fractures), spino-pelvic alignment (high transverse fractures) and lumbo-sacral joint integrity (Isler’s fractures). Though there is a universal recognition of Isler’s fractures and its impact on LSJ integrity, there is a lack of clinical and bio-mechanical evidence regarding the concept of instability caused by a unilateral Isler fracture.
Introduction
Sacral fractures have been classified by several authors over the last century.1-4 Initial classifications by Tile and Young-Burgess grouped them as part of pelvic fractures.1,2 Classifications by Denis, Roy-Camille and Isler have stood the test of time, even though they had focussed only on subset of sacral fractures.3-5 A comprehensive, all-encompassing classification has been promulgated by the AO Spine knowledge forum recently and has shown substantial inter-observer and excellent intra-observer reliability. 6
The Isler’s classification of sacral fractures is a highly focussed classification, which aims to identify patients at risk of lumbo-sacral instability. 5 It stands apart from other classifications of sacral fractures since it specifically documented a unique injury pattern and described the principles of its management in a landmark article. Based on a radiographic study involving 193 patients of pelvic fractures, Isler identified this unique injury-unilateral vertical sacral fractures that exit medial to the L5-S1 facet and classified into three subtypes. He noted that such injuries can impede successful reduction of hemi-pelvis and may predispose patients to lumbo-sacral joint instability and degeneration later. Since its original description, the classification has gained practical application in clinical practice. But despite its global acceptance, there is scarce literature on this topic and very few articles have studied the incidence and management of Isler’s fractures in the last three decades.
Sacral fractures have bio-mechanical implications with relation to the pelvic ring, spino-pelvic alignment and lumbo-sacral joint (Figure 1). While initial studies focussed on managing sacral fractures from a pelvic ring perspective,2,7 the recognition of high transverse U-, H-shaped fractures shifted the attention to spino-pelvic continuity.8-10 Despite Isler’s recognition of lumbo-sacral joint injury in a specific subset of sacral fractures, few studies have evaluated the role of sacral fractures with regards to lumbo-sacral instability.11,12 In this narrative review, we have reviewed the basic anatomy of the lumbo-sacral junction and sacrum, the evolution of various classifications of sacral fractures, specific detailing of Isler’s classification and a review of studies that have evaluated this classification. Three different bio-mechanical perspectives of sacral fractures, A: Pelvic ring discontinuity: 3D reconstructed CT image shows a fracture of the right superior and inferior pubic rami, and right sacral vertical fracture with subtle vertical displacement, B,C: Spino-pelvic disruption: coronal (B) and sagittal (C) CT images show bilateral vertical sacral fractures (U-shaped) causing fracture displacement, and discontinuity between the spine and the pelvis, D–F: Isler’s fractures causing lumbo-sacral joint injury: Antero-posterior pelvis radiograph (D) shows an intact pelvic ring and spino-pelvic continuity (incidental left inter-trochanteric fracture is noted), axial (E) and coronal (F) CT images show vertical sacral fracture on the left side where the fracture line exits medially through the S1 facet.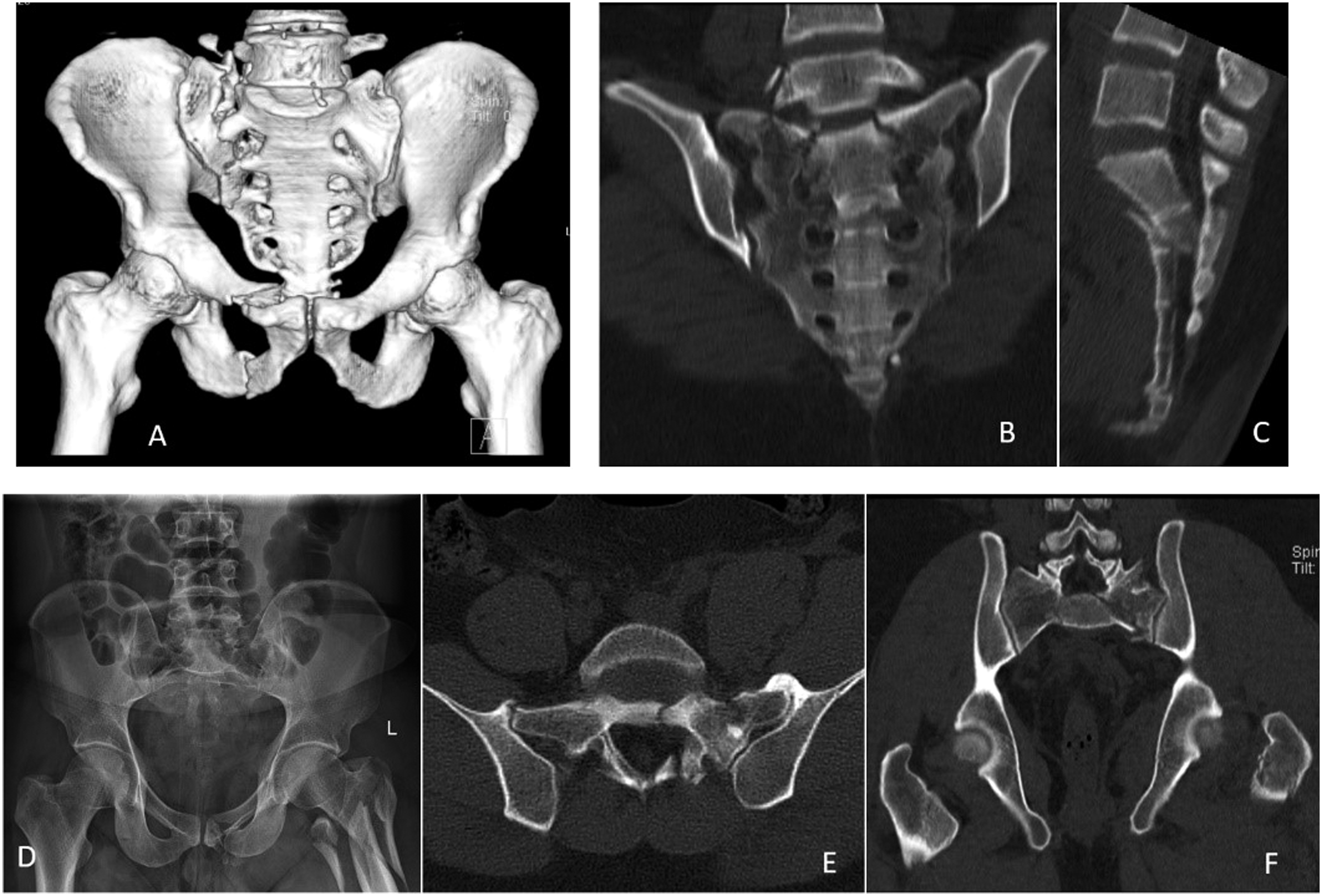
Anatomy of Sacrum and Lumbo-Sacral Junction
The sacral bone is an important connecting link between the spine and the pelvis. Its name is derived from the Latin word os sacrum meaning sacred bone, since the organs of procreation are housed beneath this bone. The five individual sacral bones unite to form the solid curvaceous kyphotic sacrum.13,14 It has a wide central canal for the S1 to S5 nerve roots to pass through, that supply innervation to the bladder, bowel, sexual function and the cutaneous nerve supply over the buttock. Anatomically, it is wedged like a keystone between the two iliac bones on either side, to which it is connected by its irregular articular margins and bolstered by heavy ligaments.
The sacrum articulates with the rest of the spinal column through the broad L5-S1 intervertebral disc anteriorly, and the facet joints posteriorly. Through these joint articulation and ligamentous attachments, it transmits axial loads to the lower limbs while sitting and ambulation. The L5-S1 facet joints are formed between the inferior articular processes of the L5 vertebra and superior articular processes of S1 vertebra. The facets of S1 are positioned facing postero-medially at an angle of about 45 to 60 degrees 15 and they interlock with the anterolaterally placed inferior facet of L5 vertebrae. The facet joints are broad and stabilised by a thick capsule. Though the lumbo-sacral joint has an acute inclination in the sagittal plane, the robust L5-S1 disc and the facet joints placed in a frontal plane orientation resist anterior translation.
Apart from these joints, there are several ligamentous connections between the sacrum and L5 vertebra including the supra- and inter-spinous ligaments, ligamentum flavum and the ilio-lumbar and lateral sacral ligaments. The first three are the standard posterior ligamentous complex of any spinal motion segment. The Iliolumbar ligament is an important stabiliser of the lumbo-sacral joint. It is a strong ligament that arises from the apex of the transverse process of L5 vertebra and radiates infero-laterally to attach to the iliac crest. The lateral lumbosacral ligament arises from the lower margin of the transverse process of L5 vertebra and passes obliquely inferiorly to attach on the ala of the sacrum. It blends with the anterior sacro-iliac ligament at its insertion on the sacrum. Other supportive ligamentous structures of the lumbo-sacral-pelvic complex include the anterior and posterior longitudinal ligaments that blend along the anterior and posterior surface of the vertebral bodies, respectively, the sacro-tuberous and sacro-spinous ligaments, and the anterior and posterior sacro-iliac ligaments that bolster the sacro-iliac joints.
Sacral Fractures
Rodrigues-Pinto R et al. stated that sacral fractures occur in association with some form of pelvic fracture in 80% to 90% of cases.
16
These injuries are notorious for being ‘overlooked’ because of its deep location and the frequent presence of polytrauma and absence of neurological deficit. Hence, they are frequently missed on initial assessment and present late in up to 30% of cases.
14
Plain radiographs of the pelvis, which are the initial investigation for evaluating sacral fractures, can miss sacral fractures easily because of the complex sacral anatomy, overlying bowel gas shadows and atypical fracture patterns of sacrum
3
(Figure 2). CT (minimum of <5 mm slices) is the investigative modality of choice not only for diagnosis but also to define the exact fracture patterns and surgical planning.11,17 Routine use of CT abdomen and pelvis has significantly increased the detection of these injuries.18,19 Sacral fractures are often missed in radiographs. In the AP radiograph (A), a sacral fracture cannot be identified. But the 3D reconstructed posterior CT view (B) clearly shows a vertical sacral fracture.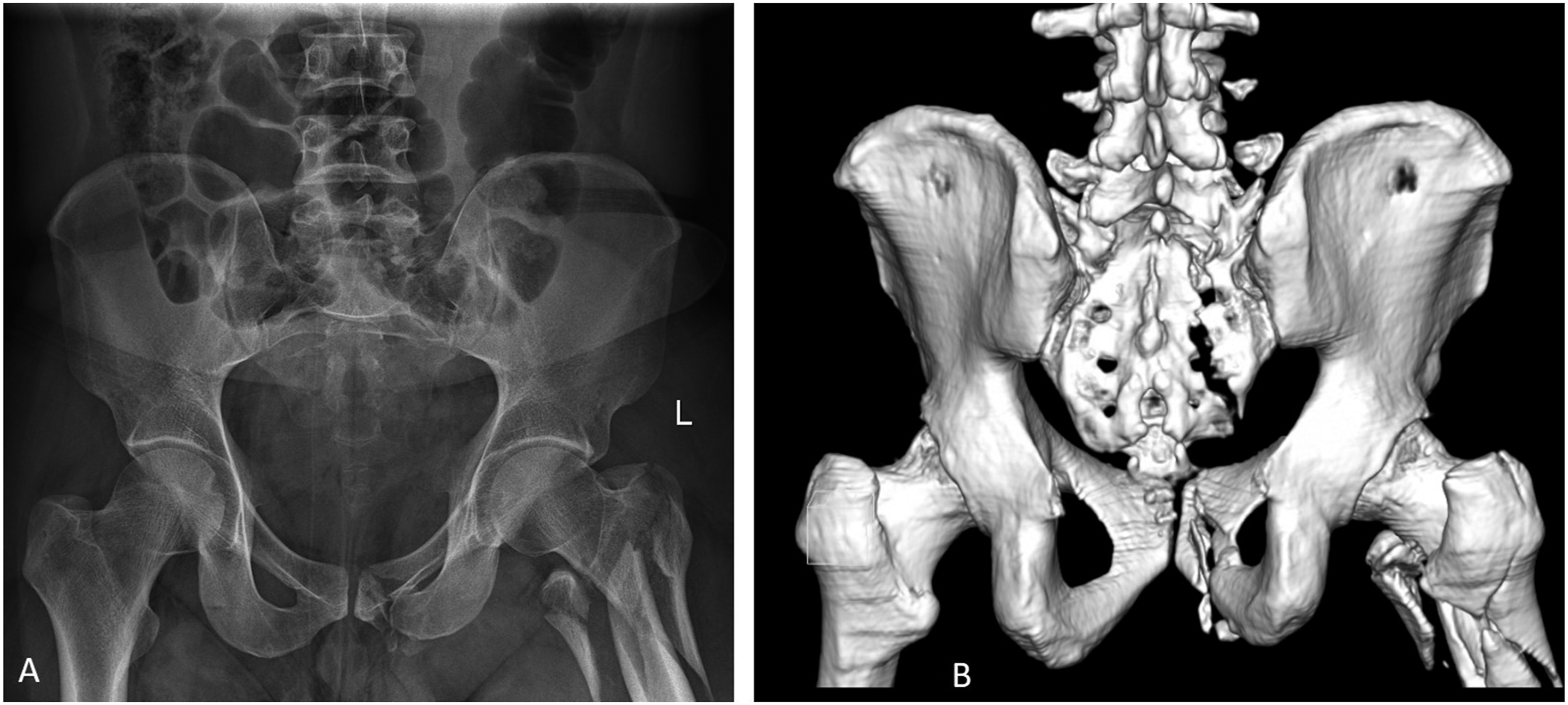
Sacral Fracture Classification
Broadly speaking, sacral fractures can be grouped into longitudinal, transverse and combined types. Isolated longitudinal fractures involve the lateral ala of the sacrum, either medial or lateral to the sacral foramina. Isolated transverse fractures occur below the level of sacro-iliac joint. Combined types involve both horizontal and vertical components.
Sacral fracture classification has evolved over many years. In 1939, Medelman morphologically classified sacral fractures into longitudinal, oblique and horizontal types based on radiographs.
7
This, and later classifications by Bonnin,
20
Fountain,
21
Schmidek
22
and Sabiston-Wing’s
23
did not gain much popularity because of their lack of clinical relevance and treatment guidelines. Denis et al (1988) provided one of the practical and clinically relevant classifications based on 223 sacral fractures.
3
They classified vertical sacral fractures into three different zones – through the ala and lateral part of sacrum (Zone 1), through the sacral neuroforamina (Zone 2) and central sacral canal (Zone 3) and denoted increasing risks of neurological injury (Figure 3(a)). Although Denis classification retains its popularity, its limitation lies in its simplicity. Often sacral fractures are transverse and bilateral, which are not included in this classification. Roy Camille et al (1985) classified transverse sacral fractures based on the displacement and angulation of the fracture fragments: - a simple angular/flexion deformity (type 1), an angular/flexion deformity with translation (type 2) and a complete translation without overlap of fracture fragments (type 3) (Figure 3(b)). Eponymously described as the Suicide Jumper’s fracture, only transverse fractures of the sacrum were described in this classification.
4
Strange-Vognsen and Lebech added a fourth type with comminution of the S1 vertebral body due to axial loading.
24
A: Denis classification – types I, II and III based on the location of the vertical sacral fracture line, B: Roy Camille transverse fractures types 1 to 4. Type 1 is a simple angular/flexion deformity, type 2 is an angular/flexion deformity with translation, type 3 is a complete translation without overlap of fracture fragments and type 4 is associated with comminution of the S1 vertebral body. C: Spino-pelvic dissociations – The sacral fracture is complex with inter-connected vertical and horizontal components which results in displacement of the central sacral fracture fragment along with the spine, from the rest of the sacrum. Based on the direction of fracture lines, they are classified as U-, H-, Lambda-shaped.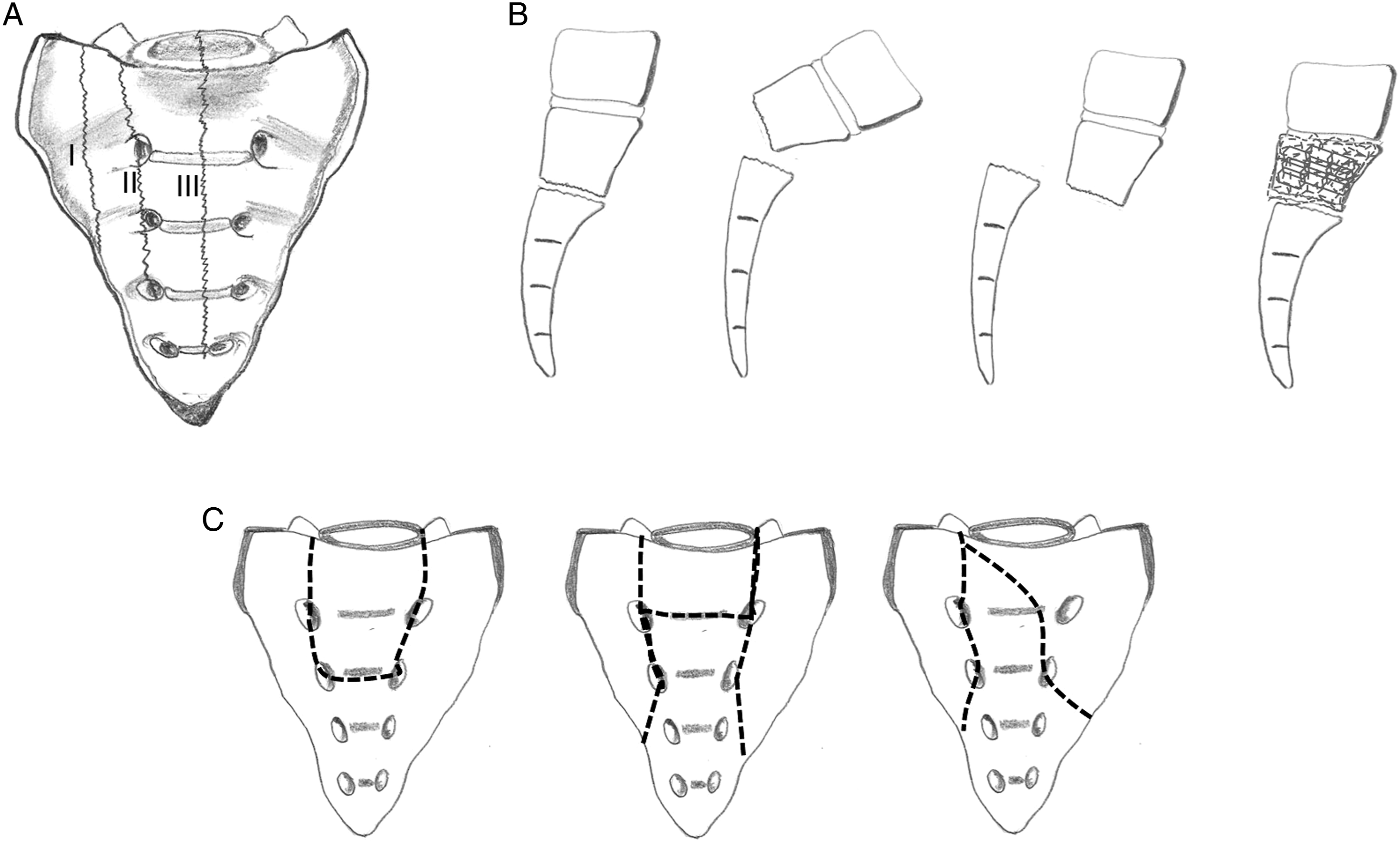
With increased use of CT, it was appreciated that traumatic transverse and longitudinal sacral fractures often occur in combination. The longitudinal fracture lines occurred on either side of sacrum and followed a straight vertical or oblique pattern.8,25 When these two longitudinal fractures were connected by a transverse fracture line, it resulted in complete separation of the pelvis from the lumbar spine, called as ‘spino-pelvic dissociation’ (Figure 3(c)). Spino-pelvic dissociation is an important entity to recognise because these fractures are almost uniformly unstable with a median sacral fragment attached to the spine and lateral sacrum attached to the pelvis. Several fracture patterns have been described, including H-shaped, U-shaped, T-shaped and lambda-shaped patterns. Lehmann et al proposed the lumbo-sacral injury classification system in 2012 modelled after similar classification systems for the sub-axial cervical injury and the thoracolumbar injury. 26 It is a scoring system with scores given based on three categories: morphology, posterior ligament complex and neurologic status. It provides a guide to treat the fracture based on the total points scored.
Isler’s Classification Based on Lumbo-Sacral Joint Instability:
From a bio-mechanical point of view, sacral fractures can be evaluated from three perspectives – disruption of posterior pelvic ring, spino-pelvic dissociation and lumbo-sacral joint injury.
Pelvic Ring Discontinuity
Unilateral vertical fractures with displacement can affect posterior pelvic ring continuity. This is associated with anterior pelvic ring disruptions and the sacral fracture can either open or displace vertically. The evaluation and management are considered in terms of retaining or regaining continuity of the pelvic ring.
Spino-Pelvic Dissociation
U-, H-, T- or lambda-shaped sacral fractures cause spino-pelvic dissociation. The median part of the broken sacrum retains its attachment with the vertebral column while the remaining sacrum with its attached hemi-pelvis on either side is completely ‘dissociated’ from the spine. This needs a different surgical approach towards fixing the lumbar spine to the pelvis using spino-pelvic constructs.
Lumbo-Sacral Joint Instability
The third perspective is to understand how a sacral fracture can potentially affect the lumbo-sacral stability. This can happen in unilateral sacral fractures where the fracture line courses medial or through the L5 S1 facet joint causing facet injury, subluxation and sometimes facet dislocation. In these injuries, there is no dissociation of the spine from the pelvis. The contralateral facet joint along with the rest of the sacrum retains its attachment to the pelvis.
The concept of Lumbo-sacral joint instability (LSJI) due to a sacral fracture was first described by Isler. 5 He believed that a fracture line that exits vertically medial or through the L5 S1 facet joint affects the integrity of L5-S1 joint. The possibility of this injury occurred to him after he encountered a locked L5-S1 facet in a patient with displaced hemi-pelvis which prevented reduction of the instability. Isler published his manuscript in 1990 based on an evaluation of 193 pelvic fractures treated between 1973–1987. It was a radiographic study and all the patients had conventional AP radiograph of the pelvis. CT scan of the pelvis was available in 52 cases. Isler noted that in 12 cases (incidence – 3.5%), the vertical fracture line coursed medial or through the L5-S1 facet joint.
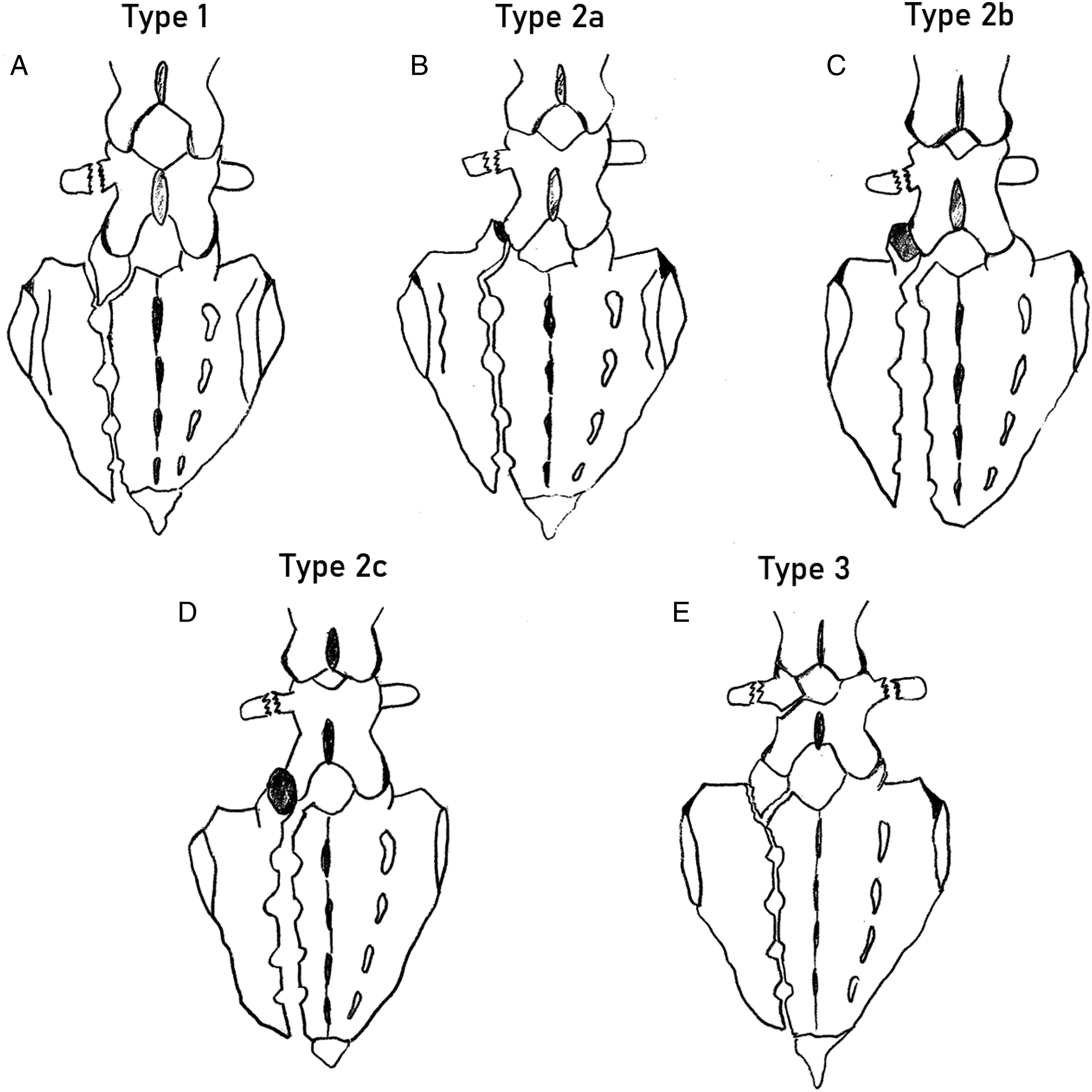
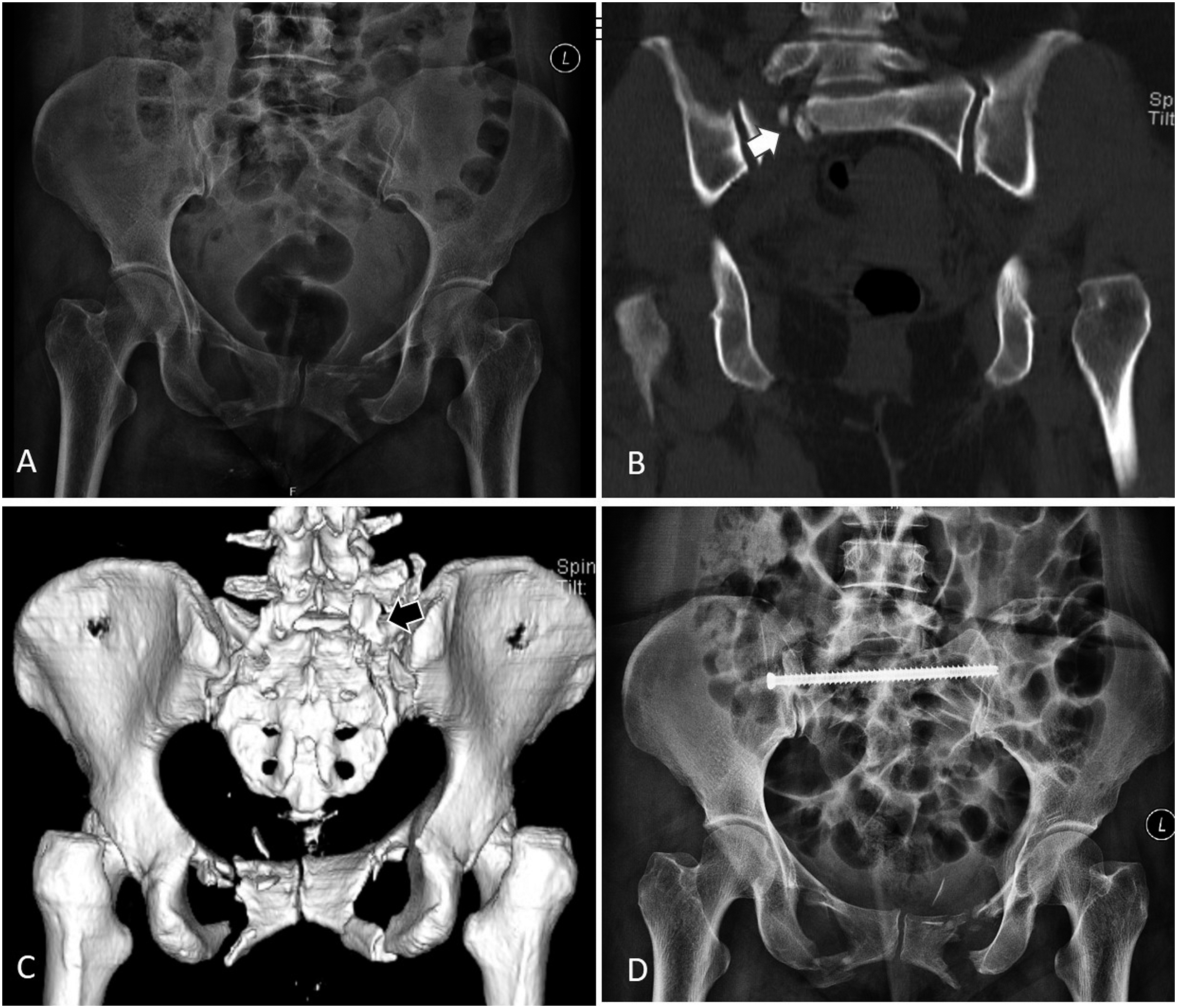
He classified the LSJI into three sub-types based on the patterns of fracture line (Figure 4), 1. Type 1: Extra articular fractures – associated with fracture of S1 or L5 facet (n = 2). Here the fracture line was accompanied by a fracture of one of the facets of L5-S1 facet joint. 2. Type 2: Articular fractures (n = 6): The fracture line passed through the L5-S1 joint. a. Fracture dislocation – fracture through S1 facet b. Subluxation – fracture line medial to the facet associated with joint subluxation. c. Locked dislocation (Figure 5) – fracture line medial to the facet associated with anterior dislocation of the S1 facet over the L5 facet. 3. Type 3: Complex injuries (n = 4), where the fracture line coursing medial to the facet was accompanied by multiple fractures of articular process, pars interarticularis of L5, lamina and the pedicles. Schematic representation of Isler’s sub-types of sacral fractures. A: Type 1 – the vertical sacral fracture is accompanied by a fracture of one of the facets of L5-S1 facet joint. Here a fracture of the S1 facet is shown. B: Type 2a – The fracture line passes through the S1 facet. C: Type 2b – fracture line passes medial to the facet but associated with L5-S1 facet joint subluxation. D: The fracture line passes medial to the facet and associated with anterior dislocation of the L5 facet over the S1 facet. E: Type 3 are complex injuries, where the fracture line coursing medial to the facet is accompanied by multiple fractures of articular process, pars interarticularis of L5, lamina and the pedicles. This 50-year-old patient sustained a pelvis injury in an accident. A – AP Radiograph shows a fracture of the anterior pelvic ring, B, C – Coronal CT and 3D reconstruction posterior images show a Type 2 C Isler fracture. The vertical fracture line is exiting medial to the L5-S1 facet and the facet is dislocated completely. D: The fracture has been reduced through a posterior approach, and fixed with trans-iliac screws.
The article has a unique standing in the evolution of sacral fracture classification. The Isler’s classification posited for the first time that a vertical fracture line traversing lateral to the pelvis is unrelated to lumbo-sacral stability, whereas the line affecting the facet integrity through a fracture or subluxation can result in LSJI. He stressed that recognising L5-SI locked dislocation would necessitate an open reduction for proper reduction of the sacral fracture. In his article, only 24% of the fractures could be evaluated by a CT scan and he reckoned that the incidence of LSJI could be higher if all fractures were evaluated with CT. Hence, he underscored the value of performing CT scan in all posterior ring injuries. Finally, he concluded that traumatic degeneration of the lumbo-sacral facet joints may be an important cause of lumbo-sacral pain after pelvic ring injuries. Interestingly, there is no suggestion of mandatory need for surgical fixation or a description of its technique in his original publication.
Reviews on Isler’s Article
The article has been cited in 107 articles since then. Excluding articles in non-English languages (n = 36) and textbook chapters, English language publications citing the article were studied. The exact reproduction of lumbo-sacral lesions as described in Isler’s classification was sparse in these articles, and the most of the articles have just cited it as part of the various classifications of sacral fractures.
In one of the key articles published in 1997, Isler’s data was verified by Oransky and Gasparini. 12 The authors studied 71 pelvic fractures with rotatory instability and vertical shear instability and noted that 13 patients had LSJI. They confirmed the presence of all the three different types of Isler’s LSJI and also noted a fourth type of injury in three patients (lesions of the annulus fibrosus of the L5-S1 disc). This new sub-type has not been confirmed in any of the other studies in literature.
In 1997, Leone et al studied 73 unstable pelvic fractures with CT and radiographs and noted a sacral fracture in 42 patients. 11 LSJI described by Isler was noted in 14 patients, including all the three sub-types. The fourth subtype noted by Oransky was not observed. The authors reiterated the observations of Isler but noted a slightly higher incidence of LSJI (6% vs 19%), which they attributed to the performance of CT in all patients.
Does LSJI Cause Low Back Pain Later?
Few bio-mechanical studies have indicated that facet resection at the lumbo-sacral joint can cause instability.27,28 However, Isler’s fractures do not result in complete instability of the L5-S1 joint. Chronic low back pain after sacral fracture is a documented entity and factors including alterations in pelvic incidence, injured sacral facets, post-traumatic lateral curvature of spine, discal injury and alterations in lumbar lordosis have been described as possible risk factors.29–31 LSJI due to Isler sacral fracture types could be one of the possible causes and needs further evaluation in longitudinal studies. Cano-Luis et al have evaluated post-traumatic pelvic asymmetry and described a unique classification to evaluate and manage these post-traumatic sequalae. 32 In their classification, the authors have noted a type of rotational instability of L5/S1 that occurs due to the non-union of the articular facet of L5/S1 as seen in Isler 2 sacral fractures. The authors advised curettage and posterior surgical fixation. This is the only study to have documented a true LSJI after a sacral fracture as predicted by Isler.
Despite the limited follow-up studies performed on this topic, there is a widespread acceptance among the spinal and trauma surgeons that fractures that exit medial to the L5 S1 joint are potentially unstable injuries. In a survey conducted by the AO Spine trauma knowledge forum, 474 surgeons when asked with the question, ‘Do you think the integrity of the L5–S1 facet is adequately considered if a unilateral vertical fracture where the ipsilateral superior S1 facet is discontinuous with the medial portion of the sacrum is considered differently from a fracture where the ipsilateral superior S1 facet is in continuity with the medial portion of the sacrum?’, 4 out of 5 respondents agreed to it. This was independent of the treating surgeon’s years of practice and experience in treating sacral fractures. 33 This indicates that many surgeons believe that Isler’s type of sacral fractures need to be treated differently than standard sacral vertical fractures.
Conclusion
Sacral fractures are unique injuries and its treatment has traditionally been decided based on the extent of co-existent pelvic injury and spino-pelvic alignment. However, a smaller percentage of sacral fractures that affect the stability of the lumbo-sacral joint has been recognised as a separate entity 30 years ago by Isler. Though disruption of the L5-S1 facet joint and the passage of fracture line through the disc space can cause LSJI, there is a lack of evidence regarding the concept of instability caused by a unilateral Isler fracture. Though a few studies have reproduced the presence of these fractures in their studies, a clear guideline for surgical indication and approach, and long-term follow-up studies comparing operative and non-operative treatment (Figure 6) are lacking for this subset of sacral fractures. Conservatively treated Isler’s Type 2a fracture. (A): AP radiograph shows a bilateral pubic rami fracture. (B, C): 3D reconstructed anterior and posterior views of the pelvis show a vertical fracture of the sacrum where the fracture line traverses the S1 facet. The patient was treated conservatively with rest for 2 weeks and then gradual mobilisation. Follow-up radiograph at 4 months (D) shows no displacement of the fracture and good healing.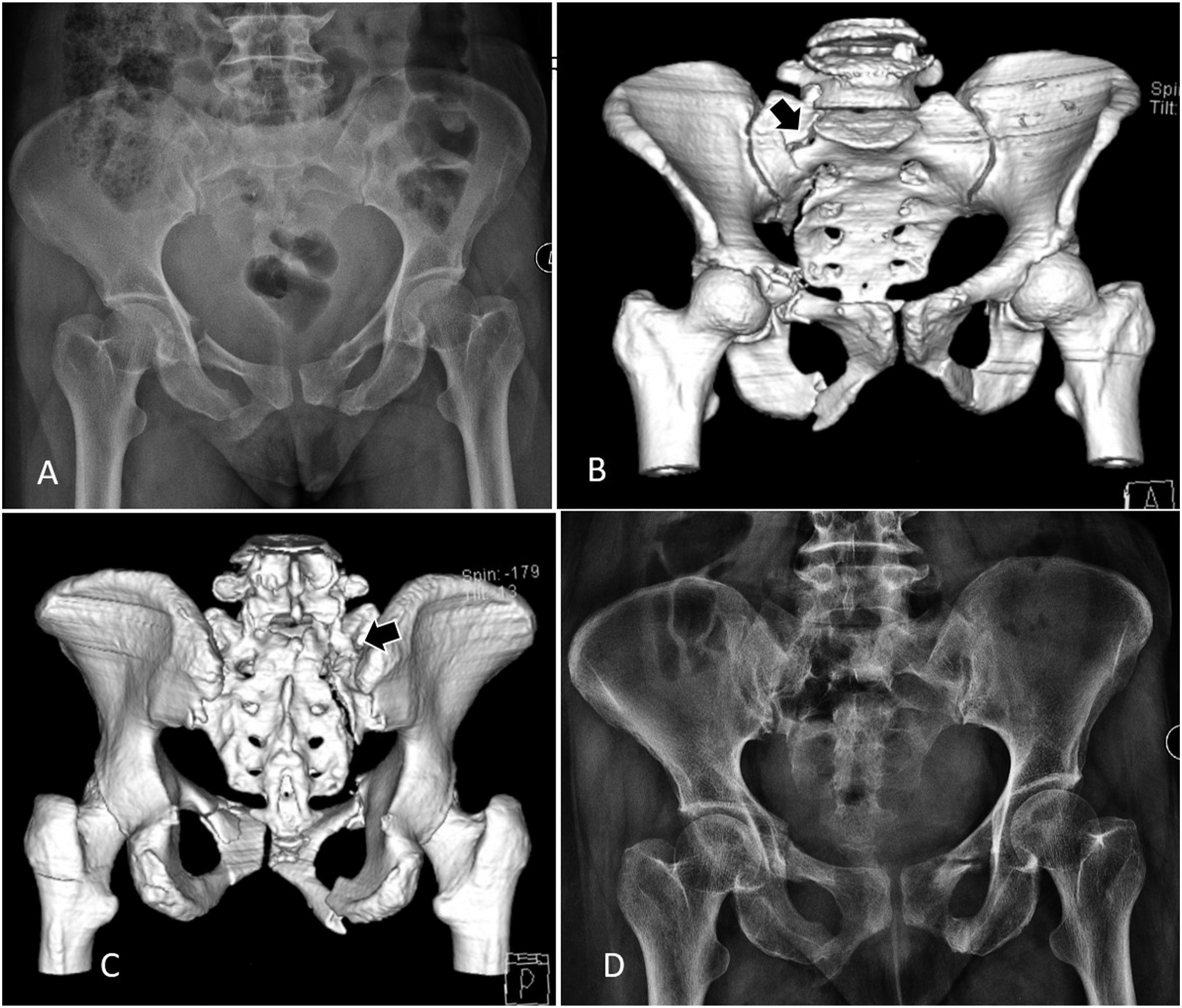
Footnotes
Acknowledgments
This study was organized and funded by AO Spine International through the AO Spine Knowledge Forum Trauma, a focused group of international spinal trauma experts acting on behalf of AO Spine. AO Spine is a clinical division of the AO Foundation which is an independent medically-guided non-profit organization. Study support was provided directly through the AO Spine Research Department.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.