
Abstract
Mid-fibular stress fractures are rare in the pediatric population and frequently present a diagnostic dilemma due to their subtle clinical presentation. In young, active children, the localized pain and associated periosteal reaction can closely mimic aggressive pathologies, such as primary bone malignancies or osteomyelitis, often leading to unnecessary parental anxiety and invasive diagnostic procedures. We report the case of a 4-year-old boy presenting with a 2-week history of an antalgic gait and localized tenderness over the left fibular shaft in the absence of acute trauma. While initial plain radiography revealed a reactive cortical lesion suspicious for malignancy, subsequent cross-sectional imaging with computed tomography and magnetic resonance imaging identified a subtle fracture line and circumferential periosteal thickening, confirming a mid-fibular stress fracture. The patient was managed conservatively with restricted weight-bearing and analgesics, with complete clinical recovery and radiographic bone remodeling documented at 2-month follow-up. This case underscores the necessity of maintaining a high index of suspicion for stress-related injuries in the pediatric population, even in the absence of a high-impact mechanism. A comprehensive diagnostic approach utilizing multimodal imaging is essential to differentiate benign stress fractures from more ominous conditions, ensuring appropriate conservative management and avoiding the risks associated with unnecessary biopsy or over-treatment.
Introduction
A stress fracture is a minor fissure in a bone. It usually happens from repeated stress or overuse, not from a single injury. Fractures are common in children and teens, especially in those who are active. These overuse injuries can harm their quality of life. Proximal fibular stress fractures are rare. They pose challenges in diagnosis and treatment, even for athletes. 1
Fibular stress fractures often cause pain in the upper leg. This can make it tricky to distinguish them from other conditions, such as growth-related pain or other fractures. 2 Their presentation is subtle, and the condition is rare. This makes diagnosis more challenging. Early recognition is vital to prevent complications. Diagnosis usually needs a careful clinical exam. Using imaging techniques such as X-rays, magnetic resonance imaging (MRI), or bone scans is also important. These help find the fracture and check for other causes of the symptoms. 3
Stress fractures in children often get misdiagnosed as tumors or infections. This happens due to the quick response of the periosteum and the large callus that forms where the injury is. 2 However, distinct imaging features can help identify stress fractures. These include a linear cortical lucency, a benign periosteal pattern, and the absence of a soft-tissue mass. Recognizing these signs is critical, as misdiagnosis can result in costly and unnecessary surgeries. 2
Managing these fractures typically involves conservative methods. These methods include rest and adjusting physical activities. Sometimes, a brace or cast is applied to support bone healing. 4 Physical therapy may also be recommended to strengthen the surrounding muscles and prevent future injuries. 4 Although surgical intervention is rarely required in pediatric patients, it may be considered in more severe cases. 4 Effective management is crucial to avoid long-term complications and ensure that the child can return to normal activities without ongoing issues. 4
This case report presents and discusses the diagnostic process of fibular stress fractures in the first decade of life. It aims to contribute to the limited existing literature and provide insights for clinicians facing similar cases to solve the dilemma between stress fractures and malignancy.
Method
This case study focuses on a first-decade pediatric patient with a mid-fibular stress fracture. It covers the clinical presentation, how we diagnosed it, the treatment provided, and the outcomes. The study includes a literature review. This helps to place the findings in a wider context and look at their impact on clinical practice. The search strategy used PubMed/MEDLINE. It focused on these keywords: “pediatric fibular stress fractures,” “mid-fibular stress fractures in children,” “lower extremity stress fractures in pediatrics,” and “diagnosis and management of pediatric stress fractures.” This literature review highlights how rare these cases are. It also shows why we must consider stress fractures when diagnosing children with limping and leg pain.
Case presentation
A 4-year-old child presented with a 2-week history of limping and localized chronic pain in the left leg. The onset of symptoms was gradual, and there was no reported history of trauma, as confirmed by the parents. The pain was localized to the left leg, exacerbated by movement but alleviated with rest and analgesics. No red flag symptoms were present. This means there was no fever, weight loss, decreased appetite, fatigue, or night sweats. Also, there were no skin signs that suggested trauma or child abuse.
During the exam, the left leg showed mild tenderness. There was no swelling, warmth, bruising, or deformity. Gait assessment revealed an antalgic gait.
Laboratory investigations were unremarkable, showing a white blood cell count of 10.81 × 109/L, hemoglobin of 12.4 g/dL, and a platelet count of 266 × 109/L. Inflammatory markers were within normal limits, with an erythrocyte sedimentation rate of 7 mm/h and a C-reactive protein level of 1.40 mg/L.
On the imaging, the first X-rays of the left leg showed a reactive lesion in the middle of the fibula (Figure 1(a)). This raised worries about possible cancer. We performed further evaluation. Computed tomography (CT) and MRI with contrast demonstrated a periosteal reaction in the fibula (Figures 2(a), 3(a), and 4). A bone tumor was suspected at first. Later, radiology reports revealed it was a mid-shaft fibular stress fracture instead.
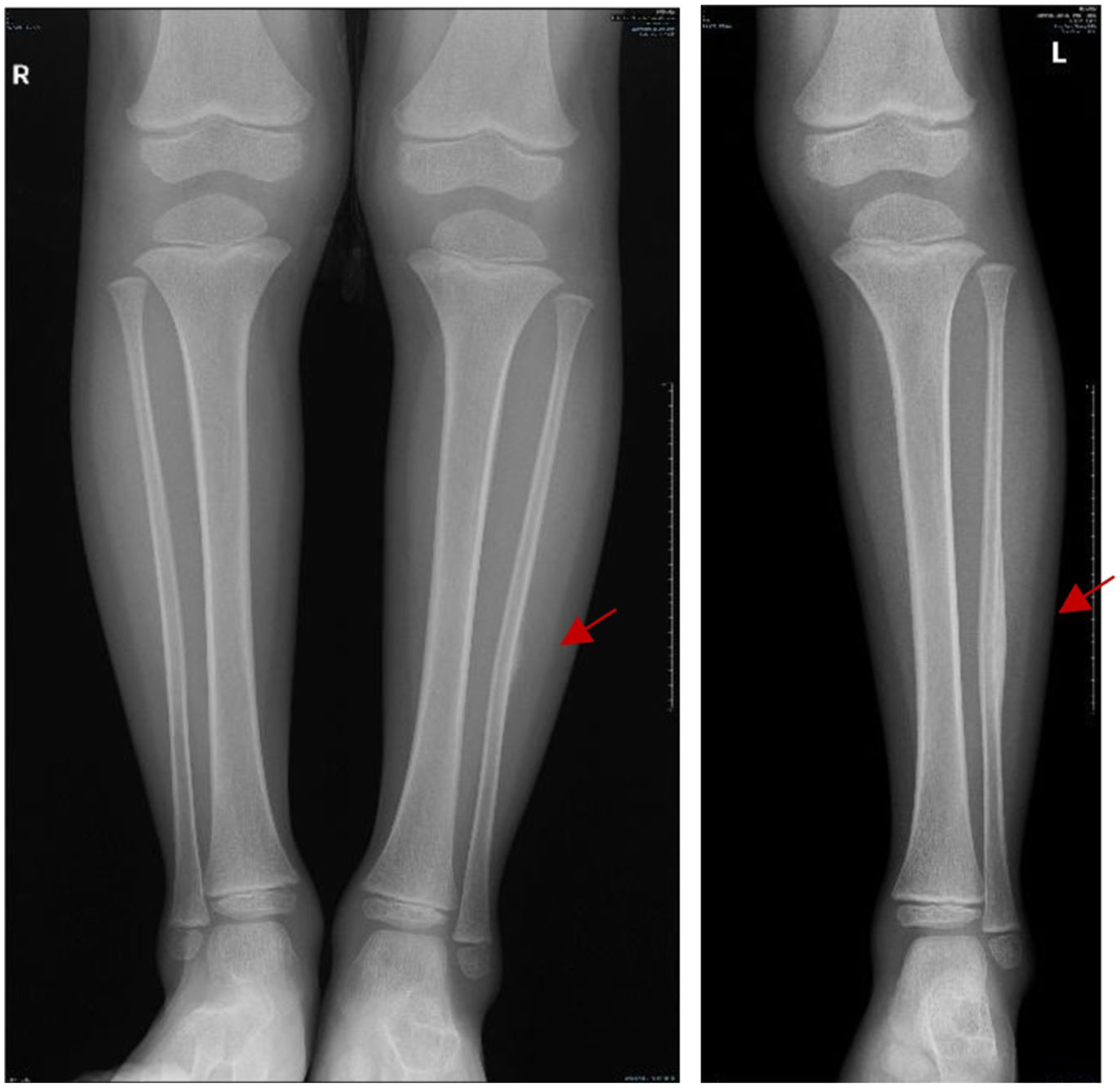
(a) A standing X-ray of the lower limb at presentation shows a left fibula mid-shaft bone reaction lesion. (b) A standing X-ray of the lower limb after 2 months shows healing of the fibula mid-shaft fracture.

(a) Axial CT scan at presentation shows an irregular periosteal reaction, no soft tissue extension. (b) Axial CT scan after 1 month shows a typical callus foration of a stress fracture.

(a) Coronial cut CT scan at presentation shows a suspicious periosteal reaction. (b) Coronial cut CT scan after 1 month shows a clear fracture line and well-formed healing callus.

MRI with contrast at presentation shows mid-shaft fibular diaphyseal nonaggressive periosteal reaction associated with bone and soft tissue edema and suspicious linear cortical defect as described, stress fracture on top of differential diagnosis.
Laboratory investigations ruled out an infectious etiology, as indicated by normal inflammatory markers, while MRI confirmed the absence of aggressive features such as cortical destruction or a soft-tissue mass. This diagnostic exclusion of osteomyelitis and tumor, combined with clear evidence of fracture healing over time, obviated the need for biopsy.
The patient received conservative management, including nonweight bearing, rest, and analgesics. At the 1-month follow-up, a repeat CT scan, as recommended by the radiologist, confirmed the diagnosis of a stress fracture (Figures 2(b) and 3(b)). The patient returned to the outpatient clinic 2 months later. Conservative management continued. The pain was gone, and they could bear full weight. X-rays showed the fracture was healing (Figure 1(b)).
Discussion
Mid-shaft fibular stress fractures are rare in young children. However, they can be hard to diagnose, especially in the first 10 years of life. These injuries usually come from repetitive stress, not sudden trauma. So, it’s important to identify them for proper treatment. 2
Stress fractures result from repetitive stress rather than sudden trauma. 2 These injuries are rare in the first 10 years of life. 5 Children’s bones are more elastic and porous than those of adults. 6 This helps the bone absorb stress and bend instead of breaking. Because these fractures are rare in young kids who don’t play hard sports, the diagnosis can be tricky. It is important to make sure the cause is not a tumor. 7
A 4-year-old child came in with a limp and pain in the left leg. The symptoms and X-ray results showed a periosteal reaction. This raised worries about bone tumors unless proven otherwise.
Primary bone tumors often occur in children. They usually show vague symptoms, unclear X-ray results, and changes in the bone’s outer layer. These findings raise concern for a bone tumor. So, it’s important to start bone tumor staging protocols right away. 5 In our patient, the gradual onset of pain without a reported history of trauma complicated the diagnosis. Initial imaging revealed a reactive lesion, raising concerns regarding malignancy. However, the utilization of multimodal imaging, specifically CT and MRI, was instrumental in differentiating the lesion from a more severe pathology.
Advanced cross-sectional imaging plays a pivotal role in distinguishing mid-fibular stress fractures from key pediatric diagnostic mimickers, particularly Ewing’s sarcoma, eosinophilic granuloma (Langerhans cell histiocytosis), and osteomyelitis. 1 On CT, stress fractures typically demonstrate a linear cortical lucency with solid periosteal reaction and preservation of cortical integrity without an associated soft-tissue mass. 1 In contrast, Ewing’s sarcoma commonly shows permeative bone destruction, aggressive or interrupted periosteal reaction (onion-skin or sunburst pattern), and a soft-tissue component, while eosinophilic granuloma often presents as a well-defined lytic lesion with beveled edges, endosteal scalloping, and limited periosteal reaction. 8 Infectious processes such as osteomyelitis may demonstrate cortical irregularity, sequestrum formation, and surrounding soft-tissue swelling. 4 MRI further improves diagnostic accuracy by revealing a low-signal fracture line with surrounding marrow edema and minimal soft-tissue involvement in stress fractures. 4 In contrast, osteomyelitis typically shows diffuse marrow signal abnormality, subperiosteal or intramedullary abscess, and soft-tissue enhancement, whereas Ewing’s sarcoma demonstrates marrow replacement with a large enhancing soft-tissue mass, and eosinophilic granuloma shows focal marrow edema with limited soft-tissue extension. 8
Biopsy was considered during the diagnostic workup given the initial radiographic concern for malignancy; however, it was deferred because advanced imaging demonstrated features consistent with a nonaggressive stress injury, and there were no systemic or laboratory findings suggestive of infection or neoplasia. In pediatric patients, biopsy is generally reserved for cases with persistent diagnostic uncertainty, aggressive imaging characteristics, soft-tissue mass, or failure of symptoms to improve with conservative management. 7 Avoiding unnecessary biopsy is crucial, as benign stress injuries and Langerhans cell histiocytosis may mimic malignant processes radiographically, and invasive procedures can expose children to avoidable morbidity. 7 Careful clinicoradiologic correlation and short-interval follow-up imaging are recommended when imaging findings are equivocal but nonaggressive. 4
In our review of fibular stress fractures in first-decade children (see Table 1), we found many cases. They show the different demographics and common diagnostic challenges linked to these injuries. Reports show that stress fractures can occur in children as young as 15 months. However, such cases are still rare. Our results support earlier research. They reveal that active children can develop stress fractures, often without any obvious trauma.
A literature review of a mid-shaft fabular stress fracture in first-decade patients.

CT: computed tomography.
A study documented a 15-month-old early walker girl with a stress fracture in the shaft of the left fibula. At first, doctors suspected Ewing’s sarcoma or eosinophilic granuloma. The doctors diagnosed a stress fracture using X-ray, CT, and bone scan tests. 5 Another case involved a 4-year-old boy with a stress fracture in the lower third of his left fibula. In this instance, bone cancer was the initial concern. The X-ray confirmed the diagnosis of a stress fracture. 9 These examples show that doctors might mistake fibular stress fractures in children for more serious problems, such as cancer. Stress fractures and specific bone tumors in the fibula can look similar on X-rays. This often leads to a misdiagnosis at first.
Stress fractures in the tibia are more common because it is the main weight-bearing bone. 1 They usually happen in the upper part of the leg. However, fibular fractures are different and often occur in the middle of the bone. 8 The pain is usually on the outer side of the leg. Since mid-shaft fibular fractures are rare in young children, they can look like Ewing’s sarcoma on an X-ray. 9 This often leads to worry about cancer before the correct diagnosis is found.
Management of mid-shaft fibular stress fractures in pediatric patients typically involves conservative strategies. 4 In our 4-year-old child, we try to decrease the child’s activity as much as possible to decrease the chance of repetitive stress fracture and allow the bone to heal, we used anterior knee slap with slight knee flexion for 2 weeks. This conservative approach is generally effective, as most pediatric stress fractures heal well with appropriate nonsurgical treatment. 4 Follow-up imaging confirmed the diagnosis. It showed significant healing. This highlights how important it is to monitor recovery in young patients.
Effective management of pediatric stress fractures necessitates a structured, evidence-based rehabilitation protocol to ensure a safe return to activity 1 :
Initial phase (weeks 0–2): Complete rest and protected weight-bearing. As noted, an anterior knee slab with slight knee flexion was utilized to minimize repetitive strain and promote primary healing.
Intermediate phase (weeks 2–6): A gradual transition to weight-bearing as tolerated, guided by the clinical resolution of local tenderness.
Return to activity (weeks 6–8+): Progressive strengthening and proprioceptive training.
Follow-up imaging in our patient confirmed the diagnosis and demonstrated significant healing. This highlights the necessity of monitoring recovery in young patients through objective assessment tools. Functional recovery was evaluated using the following criteria 4 :
Clinical: Complete resolution of localized tenderness upon palpation and the ability to perform pain-free full weight-bearing.
Functional: Restoration of a symmetrical, nonantalgic gait during normal daily activities.
Radiographic: Documentation of bone remodeling and a well-formed healing callus on follow-up imaging.
It remains crucial to differentiate fibular stress fractures from Ewing’s sarcoma and osteomyelitis. This case exemplifies the diagnostic complexity healthcare provider’s face when evaluating pediatric bone lesions. Achieving an accurate diagnosis as soon as possible after the onset of pain is essential to ensure appropriate care and avoid unnecessary intervention.
Conclusion
Finding mid-shaft fibular stress fractures in first-decade children is important for fast and effective care. Clinicians should stay alert, especially for active kids with unexplained leg pain. Unexplained radiological findings and periosteal reactions need immediate investigation to rule out bone cancer. This case contributes to the small body of research available. It highlights the need for detailed clinical evaluation and the right imaging to guide diagnosis and treatment.
Supplemental Material
sj-pdf-1-sco-10.1177_2050313X261430645 – Supplemental material for Fibular mid-shaft stress fractures in a 4-year-old child: A case report and literature review of the first decade of children with fibular stress fracture
Supplemental material, sj-pdf-1-sco-10.1177_2050313X261430645 for Fibular mid-shaft stress fractures in a 4-year-old child: A case report and literature review of the first decade of children with fibular stress fracture by Suliman Abdullah Shurbaji, Abdulaziz Ahmed Munshi, Abdulaziz Ahmed Abdulaziz, Haneen Osama Hafiz, Anas Saeed Almoabbdi and Ahmed Hosny Awad in SAGE Open Medical Case Reports
Footnotes
Ethical Considerations
The study was conducted in accordance with the ethical standards of the institutional and/or national research committee. Ethics approval for this case report was obtained, ensuring that all procedures performed involving human participants adhered to the ethical standards of the authors’ institutional research committee.
Consent to Participate
Written informed consent was obtained from the patient’s parents for participation in this case report.
Consent for publication
Written informed consent for the publication of clinical details and clinical images was obtained from the patient’s parents.
Authors’ contributions
All authors wrote the main manuscript, prepared the figures, and participated in drafting the manuscript.
Supervision was provided by
All authors have reviewed the final version to be published and agreed to be accountable for all aspects of the work.
Corresponding author:
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.