
Abstract
Study Design
Retrospective radiographic study.
Objective
We have performed occipitothoracic (OT) fusion for severe rheumatoid cervical disorders since 1991. In our previous study, we reported that the distal junctional disease occurred in patients with fusion of O–T4 or longer due to increased mechanical stress. The present study further evaluated the association between the distal junctional disease and the cervical spine sagittal alignment.
Methods
Among 60 consecutive OT fusion cases between 1991 and 2010, 24 patients who underwent O–T5 fusion were enrolled in this study. The patients were grouped based on whether they developed postoperative distal junctional disease (group F) or not (group N). We measured pre- and postoperative O–C2, C2–C7, and O–C7 angles and evaluated the association between these values and the occurrence of distal junctional disease.
Results
Seven (29%) of 24 patients developed adjacent-level vertebral fractures as distal junctional disease. In group F, the mean pre- and postoperative O–C2, C2–C7, and O–C7 angles were 12.1 and 16.8, 7.2 and 11.2, and 19.4 and 27.9 degrees, respectively. In group N, the mean pre- and postoperative O–C2, C2–C7, and O–C7 angles were 15.9 and 15.0, 4.9 and 5.8, and 21.0 and 20.9 degrees, respectively. There were no significant differences between the two groups. The difference in the O–C7 angle (postoperative angle − preoperative angle) in group F was significantly larger than that in group N (p = 0.04).
Conclusion
Excessive correction of the O–C7 angle (hyperlordotic alignment) is likely to cause postoperative distal junctional disease following the OT fusion.
Keywords
Introduction
The cervical spine is frequently affected in rheumatoid arthritis (RA), and various surgical methods have been reported to manage these lesions. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 In particular, mutilating-type RA is frequently associated with severe cervical involvement, both at the craniovertebral junction (CVJ) and subaxial levels, causing significant neurologic deficit. 9 , 10 , 11
We have performed occipitothoracic (OT) fusion for severe destructive cervical disorders since 1991 and have previously reported its clinical results and complications. OT fusion resulted in improvements in neurologic symptoms and prognosis, and postoperative distal junctional disease was the most frequent complication. 11 , 12 Hirano et al also reported the management and complications of 56 patients with RA who underwent OT fusion and noted that 11 patients (19.6%) developed thoracic spine lesions (10 fractures, 1 subluxation) after the surgery. 13 In our previous study, 12 we evaluated the incidence and risk factors for distal junctional disease in 35 patients who underwent OT fusion and found that 9 patients (26%) experienced distal junctional disease (10 fractures). Distal junctional disease occurred in patients who underwent fusion of O–T4 or longer.
To our knowledge, no published study has demonstrated the correlation between the radiographic parameters and distal junctional disease after OT fusion. Therefore, in the present study, we selected patients who underwent O–T5 fusion to avoid the influence of the number of fused vertebrae, and we measured the pre- and postoperative cervical spine sagittal alignment in these patients to evaluate the correlation between these radiographic parameters and distal junctional disease after the surgery.
Materials and Methods
Patients
Among 60 consecutive OT fusion cases between 1991 and 2010, 24 patients who underwent occipital fusion to the fifth thoracic vertebra using the RRS Loop Spinal System (Robert Reid Inc., Tokyo, Japan) were enrolled in this study. There were 4 men and 20 women with a mean age of 63.1 years (range, 47 to 75 years). The mean duration of RA was 23.5 years (range, 3 to 51 years). Twenty patients with mutilating-type disease and 4 with the more erosive subset were included. The main clinical finding was either neurologic deficit due to spinal cord compression or intractable neck-occipital pain. The neurologic status before the surgery, as determined by the Ranawat classification system, was class II in 1 patient, class IIIA in 7, and class IIIB in 16. The mean postoperative follow-up period was 42.9 months (range, 1 to 108 months). The patient characteristics are summarized in Table 1. Cervical involvement develops in the atlantoaxial joint, beginning with anterior subluxation (AAS), and may progress to vertical subluxation (VS) and/or subaxial subluxation (SAS). In this series, AAS + VS was observed in 4 patients, AAS + SAS in 1, AAS + VS + SAS in 10, SAS + ankylosis at the CVJ in 3, and SAS + anomaly at the CVJ in 1. Three patients underwent previous cervical spine surgery (2 atlantoaxial fusion, 1 occipitocervical fusion). In these patients, SAS and/or VS occurred, although solid fusion had once been achieved after the previous fusion.
Patient characteristics (n = 24)
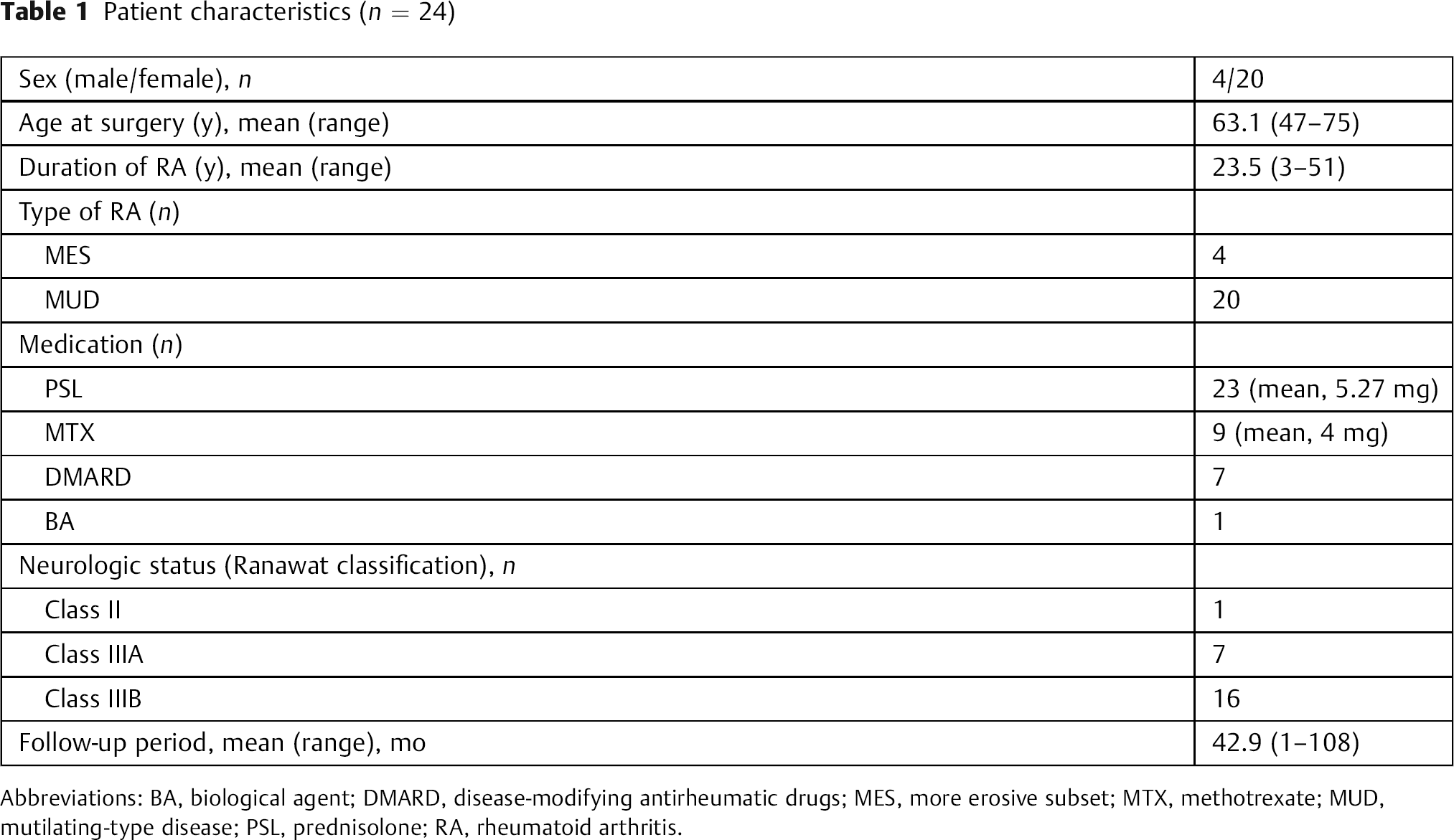
Abbreviations: BA, biological agent; DMARD, disease-modifying antirheumatic drugs; MES, more erosive subset; MTX, methotrexate; MUD, mutilating-type disease; PSL, prednisolone; RA, rheumatoid arthritis.
Operative Management
Preoperatively, the majority of patients received intermittent halo-traction on the bed for a few days to 2 weeks to obtain optimal cervical alignment, thereby reducing pain and improving the neurologic deficit. We performed O–T5 fusion using the RRS Loop Spinal System with multiple thoracic hooks (T2–T5). We used a technique with multiple hooks in the upper thoracic spine in a previous report. 12 Postoperatively, a SOMI brace was applied for 4 to 6 months.
Postoperative Distal Junctional Disease
We investigated the incidence of distal junctional disease (e.g., vertebral fracture, subluxation, dislodgement of distal anchors). Seven (29%) of 24 patients developed vertebral fractures after the surgery. However, there were no posterior element fractures with the anterior vertebral column fractures. No patient developed a new thoracic subluxation or had implant failure or dislodgment of the distal anchors. The 7 patients with distal junctional disease after the OT fusion were defined as group F, whereas the remaining 17 patients without distal junctional disease were classified as group N.
Radiographic Assessment
Sitting lateral radiographs of the cervical and upper-thoracic spine were obtained pre- and postoperatively. Lateral radiographs of the cervical spine were taken in a comfortable sitting position, with the patient's head facing forward for a horizontal gaze. The radiographic parameters investigated included the O–C2 angle, C2–C7 angle, O–C7 angle, and the difference in the cervical sagittal alignment. The difference in the cervical sagittal alignment was assessed with the following equation: dO–C2A (difference in O-C2 angle) = postoperative O–C2 angle – preoperative O–C2 angle. Then, we evaluated the correlation between the distal junctional disease and these values.
Statistical Analysis
The radiographic parameters were measured twice independently by two orthopedic spine surgeons, and the average values of both observers were used as data. In addition, the intraclass correlation coefficient was calculated to determine the intra- and interobserver reliabilities for measurement of the radiographic parameters. All parameters were analyzed using the paired t test, chi-square test, and Mann-Whitney U test. A p value < 0.05 was considered significant.
Results
Radiographic Assessment
In the radiographic measurements, the intraobserver reliabilities for O–C2 angle, C2–7 angle, and O–C7 angle were 0.95, 0.95, and 0.97 by intraclass correlation coefficient. The interobserver reliabilities were 0.97, 0.93, and 0.96. All the values indicated an acceptable reproducibility (p < 0.01).
We assessed pre- and postoperative cervical sagittal alignment in all patients. The mean pre- and postoperative O–C2 angles in all patients were 14.8 ± 11.3 and 15.5 ± 9.9 degrees, respectively. The mean pre- and postoperative C2–C7 angles were 5.6 ± 13.6 and 7.4 ± 10.4 degrees, respectively. The mean pre- and postoperative O–C7 angles were 20.5 ± 10.1 and 22.9 ± 11.0 degrees, respectively (Table 2). Fifteen patients had lordotic alignment and 9 patients had kyphotic alignment preoperatively; 21 patients had lordotic alignment and 3 patients had kyphotic alignment postoperatively.
Radiographic assessment

Note: All data is expressed as mean ± standard deviation.
Distal Junctional Disease
The occurrence of distal junctional disease was assessed. Seven (29%) of 24 patients developed adjacent vertebral fractures as distal junctional disease. All fractures occurred within 1 month after surgery. There were no differences in the characteristics (sex, age at surgery, duration of RA, type of RA, medication, neurologic status before surgery) between patients with and without adjacent vertebral fracture (Table 3).
Summary of disease parameters between the two groups
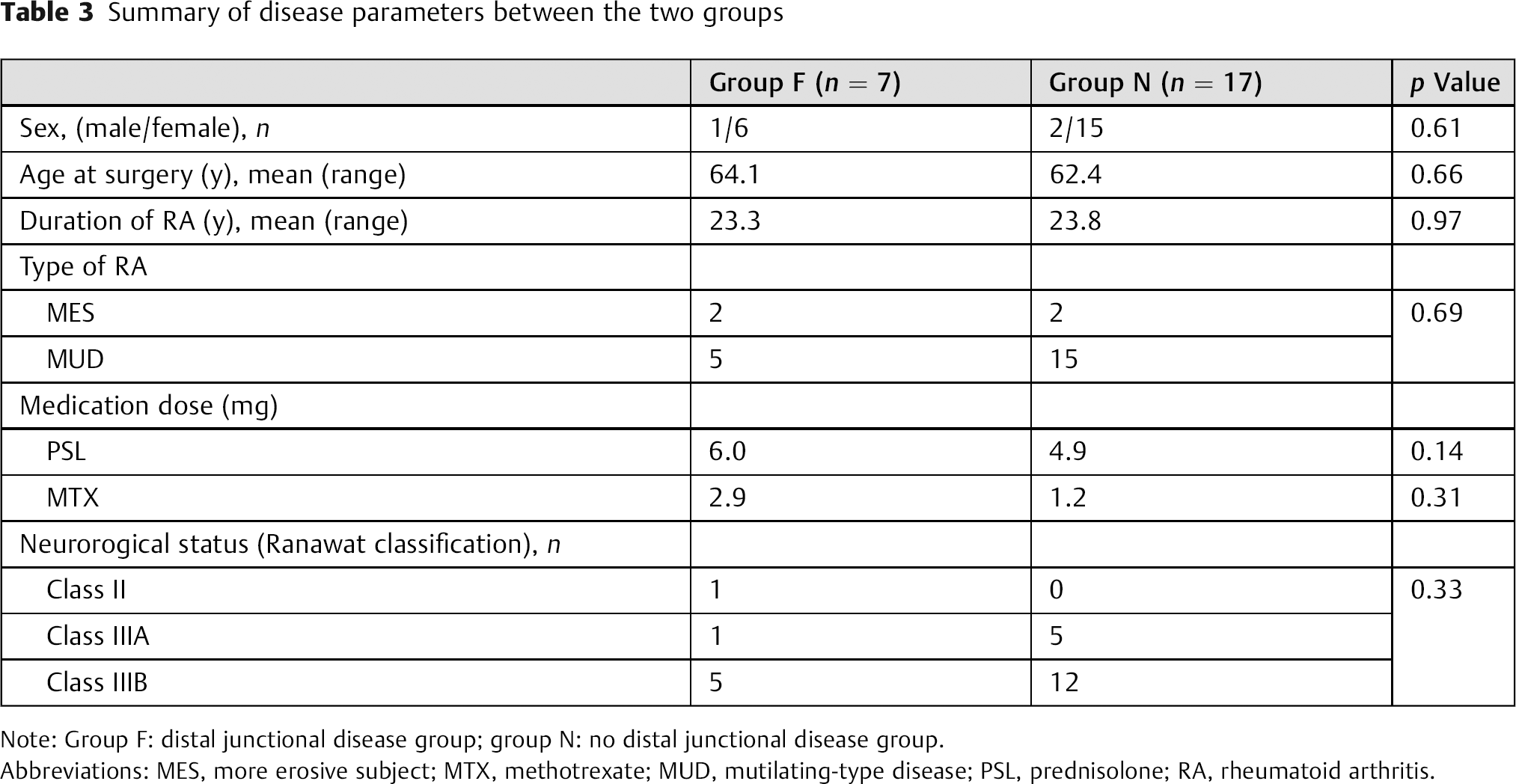
Note: Group F: distal junctional disease group; group N: no distal junctional disease group.
Abbreviations: MES, more erosive subject; MTX, methotrexate; MUD, mutilating-type disease; PSL, prednisolone; RA, rheumatoid arthritis.
Correlation between Radiographic Assessment and Distal Junctional Disease
We compared the cervical sagittal alignment between patients with and without distal junctional disease. In group F (distal junctional disease group), the pre- and postoperative O–C2 angles were 12.1 ± 12.7 and 16.8 ± 9.3 degrees, C2–C7 angles were 7.2 ± 10.6 and 11.2 ± 5.7 degrees, and O–C7 angles were 19.4 ± 10.9 and 27.9 ± 12.6 degrees, respectively. In group N (no distal junctional disease group), the pre- and postoperative O–C2 angles were 15.9 ± 10.6 and 15.0 ± 10.2 degrees, C2–C7 angles were 4.9 ± 14.7 and 5.8 ± 11.5 degrees, and O–C7 angles were 21.0 ± 9.8 and 20.9 ± 9.6 degrees, respectively. In group F, 6 patients had lordosis and 1 patient had kyphosis alignment preoperatively and all 7 patients had lordosis postoperatively. In group N, 9 patients had lordosis and 8 patients had kyphosis preoperatively and 6 patients had lordosis and 1 patient had kyphosis postoperatively. There were no significant differences between the two groups regarding the pre- and postoperative O–C2, C2–C7, or O–C7 angles. We also assessed the difference in cervical sagittal alignment. In group F, dO–C2A was 4.7 ± 8.6 degrees, dC2–C7A was 4.0 ± 10.5 degrees, and dO–C7A was 8.5 degrees ± 6.8 degrees. In group N, dO–C2A was −0.8 ± 6.9 degrees, dC2–C7A was 0.9 ± 9.5 degrees, and dO–C7A was −0.1 ± 8.8 degrees. dO–C2A and dC2–C7A were not significantly different between the two groups (p = 0.10 and 0.63, respectively). However, dO–C7A in group F was significantly larger than that in group N (p = 0.04). These results are summarized in Table 4.
Correlation between the radiographic assessment and distal junctional disease
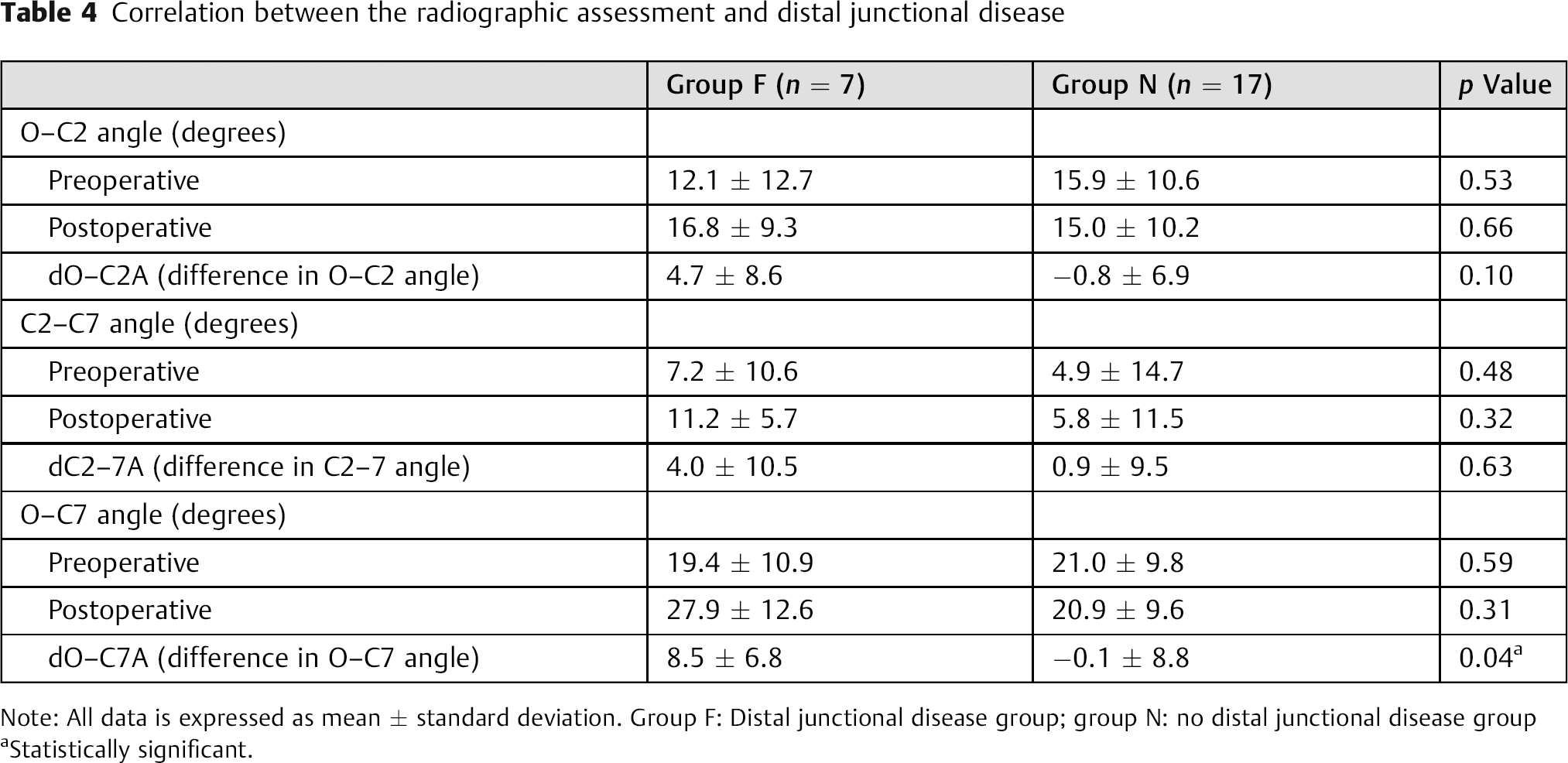
Note: All data is expressed as mean ± standard deviation. Group F: Distal junctional disease group; group N: no distal junctional disease group
Statistically significant.
Discussion
For severe destructive cervical disorders, we have performed OT fusion and previously reported its clinical results and complications. 11 , 12 In our previous report, distal junctional disease was the most frequent complication of OT fusion. Patients with RA who underwent OT fusion had advanced RA; thus, the inflammatory process may have affected distal junctional disease. 14 However, the mechanical stress due to long-distance fusion and the change in sagittal alignment may be more important factors, because all vertebral fractures in this study developed within 1 month after surgery.
With regard to the distal anchors in OT fusion, we have mainly used multiple hooks. In the present study, there were no implant failures or dislodgment of the distal anchors. We believe that safety anchors should be used at the distal ends of the stabilization area so as not to induce renewed neurologic deficits due to distal junctional disease; multiple thoracic hooks are stronger and safer than pedicle screws for the fragile spine. Several biomechanical studies supported our hook concept for fragile bones. 15 , 16 , 17
Several studies have reported the correlation between the radiographic parameters and the development of SAS in patients with RA who underwent cervical intervention. 18 , 19 , 20 , 21 , 22 , 23 With regard to C1–C2 arthrodesis for AAS, several studies have mentioned that the optimal AA angle for C1–C2 fixation is ∼20 degrees. 23 , 24 Ishii et al reported that overcorrection of the atlantoaxial angle in C1–C2 arthrodesis is strongly correlated with the development of postoperative SAS. 20 Yoshida et al reported that decrease in range of motion in the O–C1 segments is a risk factor for postoperative SAS. 21 With regard to occipitocervical fusion, Matsunaga et al reported that in patients with RA, the position of fixation of the occipital bone and axis should be within the range of 0 to 30 degrees, considering the long-term effects on the middle and lower cervical vertebrae. 22 In the present study, the postoperative O–C2 angle was outside the range of 0–30 degrees in only two patients, who did not experience distal junctional disease.
In contrast, a few studies have reported the correlation between the radiographic parameters and distal junctional disease after entire cervical fixation surgery such as OT fusion. In the present report, we focused on the O–C7 angle as the whole cervical sagittal alignment. There were no significant differences between the patients with and without distal junctional disease regarding the pre- and postoperative O–C2, C2–C7, or O–C7 angles. However, dO–C7A in patients with distal junctional disease was significantly larger than that in patients without distal junctional disease. This finding suggests that excessive correction of the O–C7 angle (large dOC–7A) might cause postoperative distal junctional disease. In the entire cervical fixation surgery, the excessive correction of the O–C7 angle (hyperlordosis alignment) can lead to the patient's head facing upward. Therefore, when the patient looks straight to obtain horizontal gaze, slightly excessive flexion force may add to the caudal end of the instrumentation area and may cause postoperative distal junctional vertebral fracture because of the significant bone fragility (Table 4, Fig. 1).
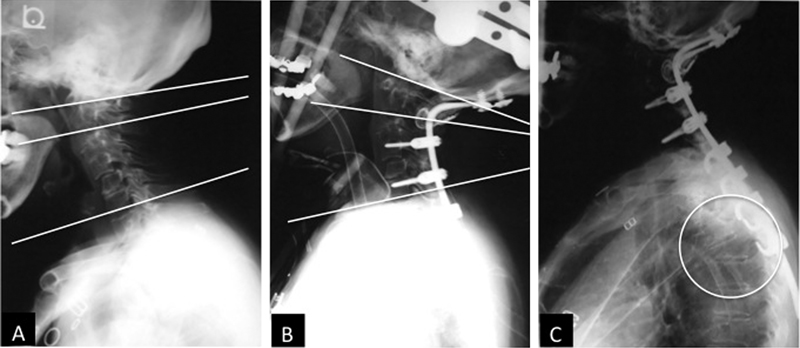
The O–C2 angle is the angle between the McGregor's line and the lower edges of the vertebral body of C2 in the lateral radiograph view. The C2–C7 angle is the angle between the line connecting the lower edges of the C2 and C7 vertebral bodies. The O–C7 angle is the sum of the O–C2 and the C2–7 angle. Lateral radiographs of a 65-year-old woman with mutilating-type rheumatoid arthritis (RA) who had distal junctional disease after O–T5 fusion. (A) Lateral radiograph showed remarkable anterior subluxation plus vertical subluxation plus subaxial subluxation due to RA before surgery. Preoperative O–C2, C2–C7, and O–C7 angles were 5, 6, and 11 degrees. (B) She underwent O–T5 fusion using RRS loop spine system (Robert Reid, Inc., Tokyo, Japan). Postoperative O–C2, C2–C7, and O–C7 angles were 14, 14, and 28 degrees. The difference in the O–C7 angle was 17 degrees, indicating excessive correction. (C) At postoperative 1 month, she had a vertebral fracture of T5 at the lowest level of the fusion area (circle).
Dysphagia and/or dyspnea after posterior occipitocervical and OT fusion in an inadequate fixed position have been recognized as a serious postoperative complication. 25 , 26 Therefore, many surgeons and researchers discussed the importance of sagittal alignment in the cervical fixation surgery. However, the optimal cervical alignment in each individual case is not known because it is complicated. Recently, several studies have reported the correlation between the cervical sagittal alignment and the T1 slope. 27 , 28 , 29 , 30 Shimizu et al investigated the outcome of posterior correction surgery for irreducible kyphotic deformity at CVJ. 30 Their report on the cervical sagittal alignment indicated that even after dynamic sagittal alignment change at the CVJ, the McGregor slope and T1 slope were stable, and that this surgical technique has a small impact on the horizontal gaze and thoracic sagittal alignment. This report and our present study indicate that the O–C7 (T1) angle in each individual case may become a useful parameter and that especially in entire cervical fixation surgery such as OT fusion, we should measure O–C7 angle in a comfortable sitting position with the patient's head facing forward for horizontal gaze preoperatively; the angle should be maintained postoperatively, even if patients need to correct local kyphosis at the CVJ and/or subaxial cervical spine.
This study had several limitations. The upper-thoracic spine, global alignment, and balance were not assessed. The upper-thoracic spine could not be evaluated precisely due to the anatomic interference limitation of the shoulder contour density, especially in the patients with an osteoporotic spine. Furthermore, we agree that the sagittal balance of the whole spine is very important. However, how to assess the cervical sagittal balance is still under discussion, and we have no global standard. In addition, most of the patients in the present study had severe neurologic deficit (16 of 24 patients could not stand, and the residual cases had unstable standing position), and standing X-rays could not be taken. Therefore, we did not evaluate the sagittal balance before surgery.
Conclusion
The change in the O–C7 angle affected the development of distal junctional disease after OT fusion in patients with RA; thus, the O–C7 angle may serve as a useful parameter for planning a fusion angle in entire cervical fixation surgery such as OT fusion. To prevent the development of distal junctional disease after OT fusion, we recommend surgeons should avoid excessive correction of the O–C7 angle.
Disclosures
Tetsu Tanouchi, none
Takachika Shimizu, none
Keisuke Fueki, none
Masatake Ino, none
Naofumi Toda, none
Nodoka Manabe, none
Kanako Itoh, none