
Abstract
Study Design
Retrospective Cohort.
Objectives
Craniovertebral instability can arise from various congenital or acquired conditions, but definitive management often requires craniocervical fusion. This study evaluates whether postoperative clivo-axial angle (CXA) can predict distal junctional failure in patients undergoing craniocervical fusion. While postoperative alignment of the head and cervical spine can be quantified via the CXA, it is unclear whether the CXA can predict distal junctional failure.
Methods
All patients undergoing craniocervical decompression and fusion (CCF) for craniovertebral instability between 2012 and 2023 at a single institution were identified. Patients experiencing adjacent segment disease (ASD) were identified and compared to those without said pathology based on CXA, Grabb-Oakes line (pBC2), and the presence of cervical kyphosis, cervical disc degeneration, or subluxation on pre- and postoperative imaging. Statistical analysis included Shapiro-Wilk tests for normality, followed by independent t-tests or Mann-Whitney U tests with FDR adjusted P values as appropriate, and univariable logistic regression.
Results
71 patients were included, of whom ten (14.3%) developed distal junctional kyphosis and 3 (4.3%) developed cervical spondylolisthesis. The median postoperative CXA was significantly lower in non-ASD patients (144° [IQR: 140-148°] vs 158° [IQR: 153-162°]; P < .001) and logistic regression showed that each 10° degree increase in CXA was associated with a 6.7-fold higher odds of ASD.
Conclusions
We found craniocervical alignment, as assessed by CXA, independently predicted distal junctional disease in patients undergoing craniocervical fusion, possibly due to low preoperative CXA in these patients. Large increases in CXA may contribute to postoperative instrumentation failure.
Keywords
Introduction
Multiple pathologies can cause instability of the craniovertebral junction (CVJ), including trauma, congenital disorders (e.g., Morquio syndrome, Down syndrome, Ehlers-Danlos syndrome), tumors, and autoimmune disease (e.g., rheumatoid arthritis/RA). Definitive management is through craniocervical fusion (CCF).
1
CVJ deformities can be assessed using parameters such as the clivo-axial angle (CXA) and the Grabb-Oakes line (pBC2). A low CXA and a high pBC2 are associated with cervicomedullary compression, which craniocervical fusion (CCF) aims to relieve by realigning the CVJ. (Figure 1). Additional compression at the CVJ may result from the formation of a retro-odontoid pannus, as seen in RA. CVJ stabilization with CCF eliminates the micromotions that cause the repeated CVJ injury leading to inflammation and pannus formation, thereby often resolving the pannus over time.
2
Illustrations. Left: Pre-reduction basilar invagination. Right: After Chiari decompression, cervical distraction and extension, and occipitocervical fusion, the basion is distracted rostral to the odontoid and the clivus—canal angle is increased, permitting anterior decompression of the brainstem. Reproduced with permission from Kim et al, Journal of Neurosurgery; published by The Journal of Neurosurgery Publishing Group 2004.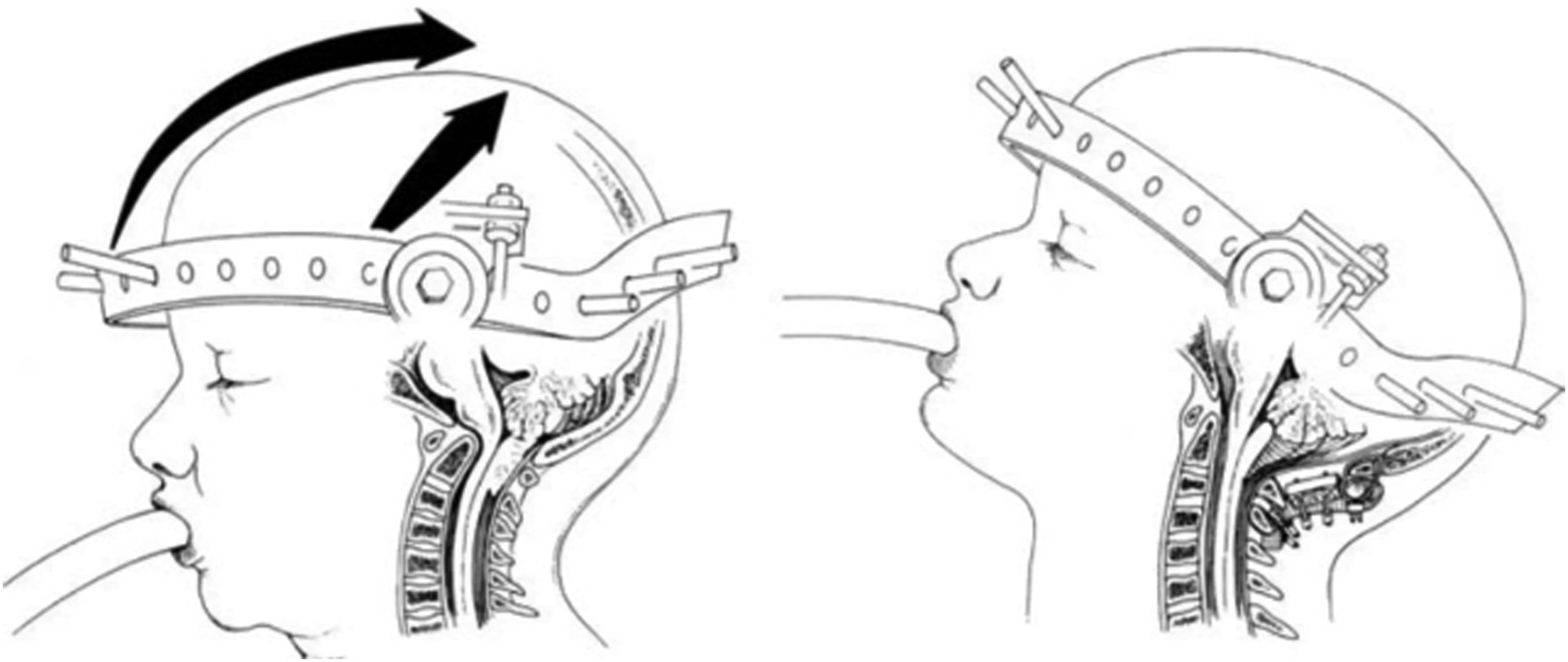
Despite addressing the altered biomechanics of the CVJ, CCF may significantly alter the biomechanics of the subaxial cervical spine, generating a stress riser below the occipitocervical construct. Adjacent segment disease (ASD) is well-documented following instrumented fusion of the cervical, thoracic and lumbar spine for degenerative pathologies3,4 and encompasses degeneration of the subjacent intervertebral disc, kyphosis at the motion segment adjacent to the lowest instrumented vertebra (LIV), and even hardware loosening.5,6 Though often asymptomatic, it may be associated with symptoms requiring the need for surgical revision.
Both construct length and the relative degree of extension at the CVJ may alter the biomechanics of the CCF construct in such a manner as to influence the risk for ASD. However, such an analysis has not been described heretofore. The objective of the present manuscript is to assess the degree to which postoperative locoregional alignment, as described by CXA and pBC2, is associated with ASD following CCF.
Materials and Methods
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Northwell Health (Lenox/NSUH Neurological Tumor Database IRB #21-0008, approved March 10th, 2021). The need for informed consent was waived due to the retrospective study design and de-identified data used for analysis.
Study Design
Following IRB approval, all patients who underwent O-C2 or O-C3 craniocervical fusion between 2012 and 2023 for craniovertebral instability were identified. Pre- and postoperative MRI, CT, and lateral X-rays were evaluated for the CXA, pBC2, and development of radiographic ASD. Junctional instability in the postoperative setting was defined by the development of new degenerative changes or pathological mobility at the subaxial cervical spine levels adjacent to the site of craniocervical fusion. Radiographic changes included the development of new degenerative changes such as cervical kyphosis or spondylolisthesis, segmental kyphosis, more than 2 mm of anterolisthesis, and more than 3 mm of motion on flex-ex films. Radiology review was performed with first available post op imaging. Patients were included if they had both pre- and postoperative MRI, CT, and lateral X-rays. Patients were excluded if they lacked the aforementioned imaging studies to ensure the accuracy and consistency of the measurements of key parameters, such CXA and pBC2. Since these imaging modalities are crucial for precisely evaluating CVJ alignment, inconsistent or missing imaging data would have compromised the validity of the measurements and reliability of the study’s findings. Among patients meeting inclusion/exclusion criteria, details were gathered on preoperative craniocervical alignment, patient demographics (sex, age), and postoperative craniocervical alignment. All data were blinded prior to analysis. This included the removal of patient identifiers and any information that could potentially reveal group assignment or outcomes.
Radiographic Measurements
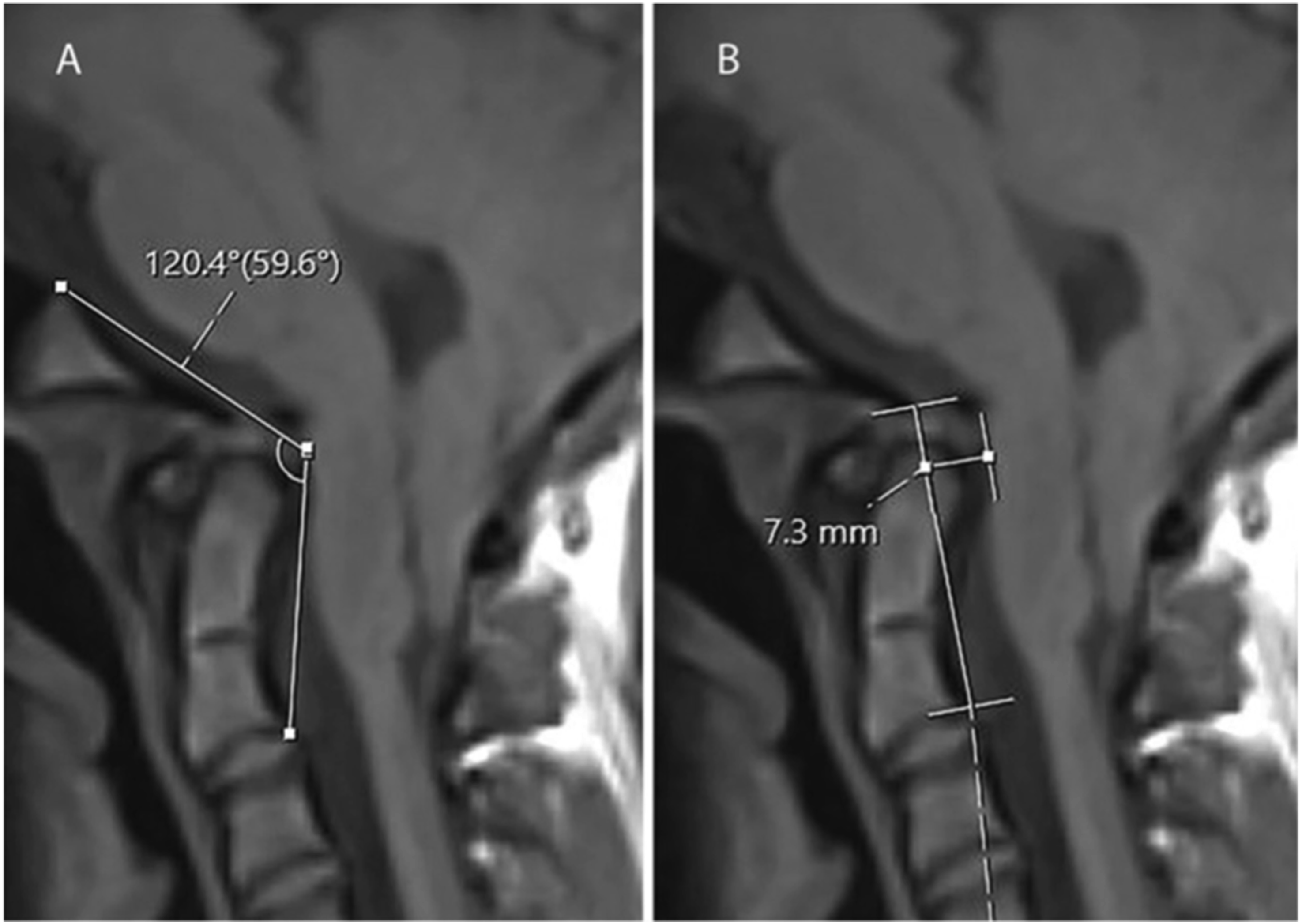
Preoperative craniocervical alignment was assessed using mid-sagittal slices of supine T1-weighted MRI. The CXA was defined by the angle subtended by a line extended along the posterior surface of the clivus and the posterior axial line – the line drawn superiorly from the posterior inferior vertebral body of C2 along the odontoid (Figure 2A).
7
The pBC2 was measured as the orthogonal distance between a line drawn from the basion to the posterior inferior C2 body and the ventral neuraxial surface (Figure 2B). Two board certified radiologists independently obtained the measurements assessed in this study. The bony anatomy was utilized for all measurements to avoid confounding of measurements when a soft tissue pannus was present. For each patient, the adjacent segments were defined as the immediate subjacent level below the end of the fusion construct. Each segment was assessed for new degenerative disc changes, spondylolisthesis, cervical kyphosis, and pathologic mobility on dynamic imaging as defined by radiologic measurement. CXA and pBC2 Measurements. (A) Example measurement of Clivo-Axial Angle (CXA); (B) Example measurement of Grabb-Oakes line (pBC2). Adapted from Sunshine et al under CC BY 4 License.
7
Outcome Definitions
ASD was defined as radiographic evidence of degeneration at levels immediately adjacent to the fusion construct. This included distal junctional kyphosis (DJK), defined as kyphotic deformity developing below the lowest instrumented vertebra. Cervical spondylolisthesis was defined as anterior translation of a vertebra relative to the subjacent vertebra by more than 2 mm on imaging. In cases where both DJK and spondylolisthesis were present, the pathology was classified under the broader category of DJK for analytical purposes. Distal junctional failure (DJF) represented cases where ASD progressed to require surgical intervention.
While preoperative measurements were consistently obtained from MRI to optimize visualization of neural elements and soft tissue structures, pragmatic considerations occasionally necessitated the use of alternative imaging modalities (CT or X-ray) for postoperative measurements. This approach reflects real-world clinical practice where radiation exposure must be balanced against imaging needs. Therefore, in some cases where measurements were obtained from alternative imaging studies using consistent anatomical landmarks.
Statistical Analysis
The primary outcome of interest was the development of radiographic adjacent segment disease on follow-up imaging.
Based on Shapiro-Wilk test results, comparisons between groups were performed using independent t-tests for normally distributed variables and Mann-Whitney U tests for non-normally distributed variables. Variables are presented as mean ± standard deviation for normally distributed data or median (interquartile range) for non-normally distributed data. P-values were adjusted for multiple comparisons using the False Discovery Rate method. Logistic regression was employed to assess the relationship between multiple predictor variables and the development of ASD. Logistic regression allows for the estimation of odds ratios, which quantify the strength of the association between our predictors, such as postoperative CXA and the likelihood of ASD. The use of logistic regression also facilitates the adjustment for potential confounding variables, providing a more accurate model of the factors influencing ASD risk. Statistical significance was set at P ≤ .05. All analyses were conducted using Microsoft Excel (Microsoft, 2024) and graphs were made using GraphPad Prism 10 (GraphPad Software, 2024). Patients with radiographic evidence of ASD were compared to those without using independent t-tests for continuous variables (e.g., age, preoperative CXA, postoperative CXA, and change in CXA) and chi-square analysis for categorical data (e.g., gender distribution, use of posterior fossa reconstruction, occurrence of revision surgery). Univariable logistic regressions were performed to identify whether radiographic parameters on pre- or postoperative predicted the occurrence of ASD. For those predictors identified as significant, receiver operating characteristic (ROC) analyses were performed to determine the predictive value of the radiographic parameter for the occurrence of ASD. Statistical significance was established as P ≤ .05.
Results
Demographic and Surgical Characteristics Comparison.
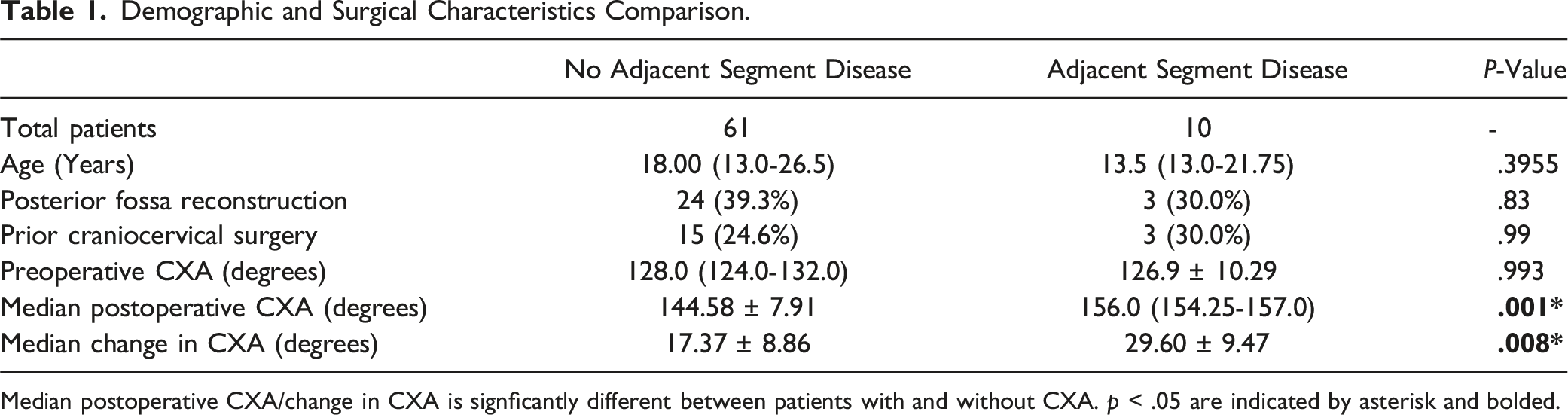
Median postoperative CXA/change in CXA is signficantly different between patients with and without CXA. p < .05 are indicated by asterisk and bolded.
There were no notable differences in surgical techniques between patients who developed ASD and those who did not. Both cohorts had similar rates of posterior fossa reconstruction and revision surgery, indicating that the surgical approach was consistent across the groups. No significant differences were found between the cohorts in terms of the surgical dates with the timing of surgeries similar across both groups.
Comparison of Radiographic Measures Between ASD and Non-ASD Groups.
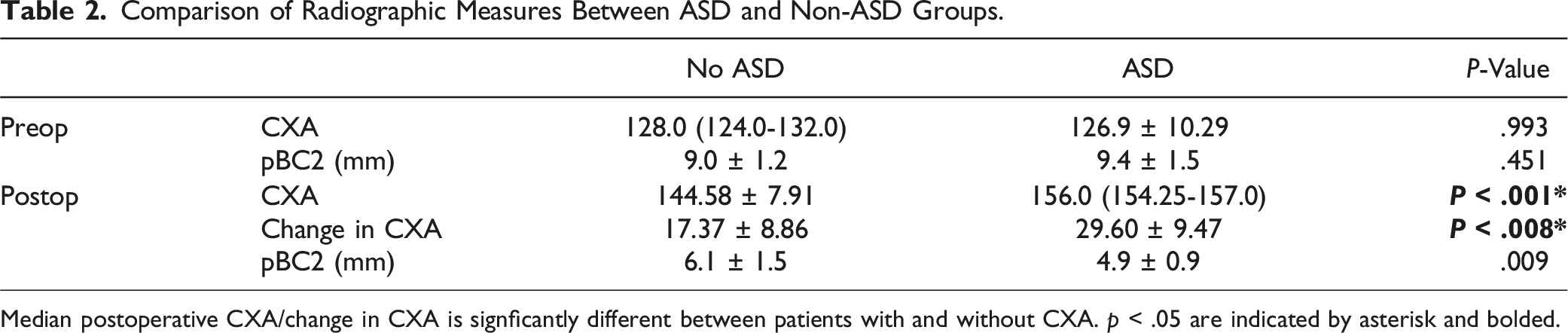
Median postoperative CXA/change in CXA is signficantly different between patients with and without CXA. p < .05 are indicated by asterisk and bolded.
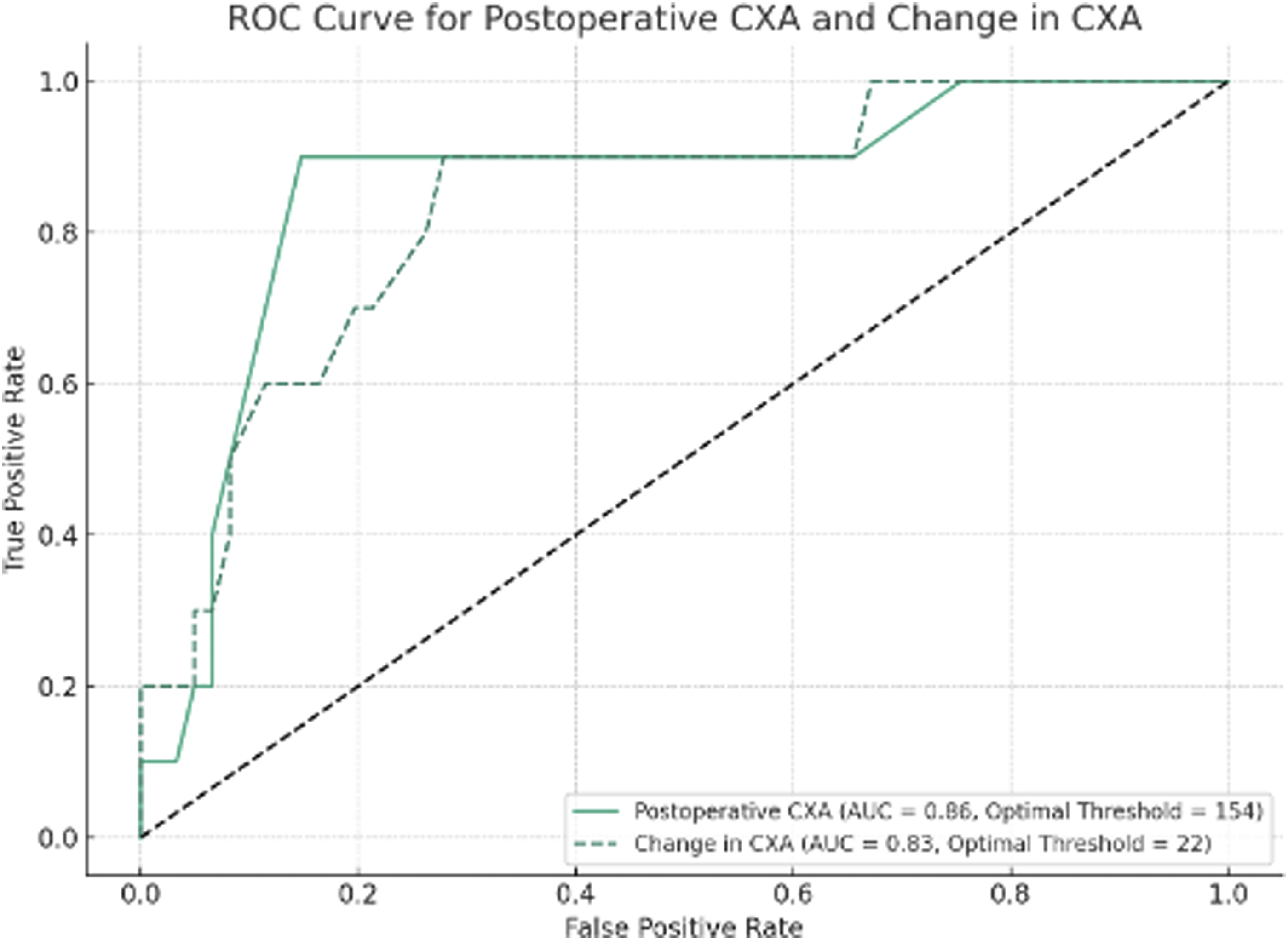
Logistic regression showed a 1.2-fold increased odds of ASD for each one-degree increase in postoperative CXA (P = .001, FDR Adjusted). At CXAs of 145° and 155°, the probabilities of ASD were 5.6% and 28.6%, respectively with an odds ratio of 6.7 for every 10° increase in postoperative CXA (Figure 3). This statistically significant finding suggests a strong association between increased postoperative CXA and the likelihood of ASD, indicating that even small changes in CXA can substantially impact the risk profile for patients undergoing CCF. There was a strong correlation between the change in CXA and change in pBC2 postoperatively (R = −0.778, P < .001). ROC curves created for postoperative CXA and change in CXA showed C-statistics of 0.86 and 0.83, respectively, indicating good predictive ability (Figure 4). Optimal thresholds for predicting the occurrence of ASD were 154° for postoperative CXA and 22° for change in CXA. Probability of adjacent segment disease (ASD) based on postoperative clivo-axial angle (CXA). Receiver Operating Characteristic (ROC) curves for postoperative clivo-axial angle (CXA) and change in CXA. The figure illustrates the receiver operating characteristic curves for postoperative CXA (solid line) and change in CXA (dashed line), predicting the occurrence of adjacent segment disease (ASD). Area under the curve (AUC) values are 0.86 for postoperative CXA and 0.83 for change in CXA, indicating good predictive ability. Optimal thresholds identified are 154° degrees for postoperative CXA and 22° for change in CXA.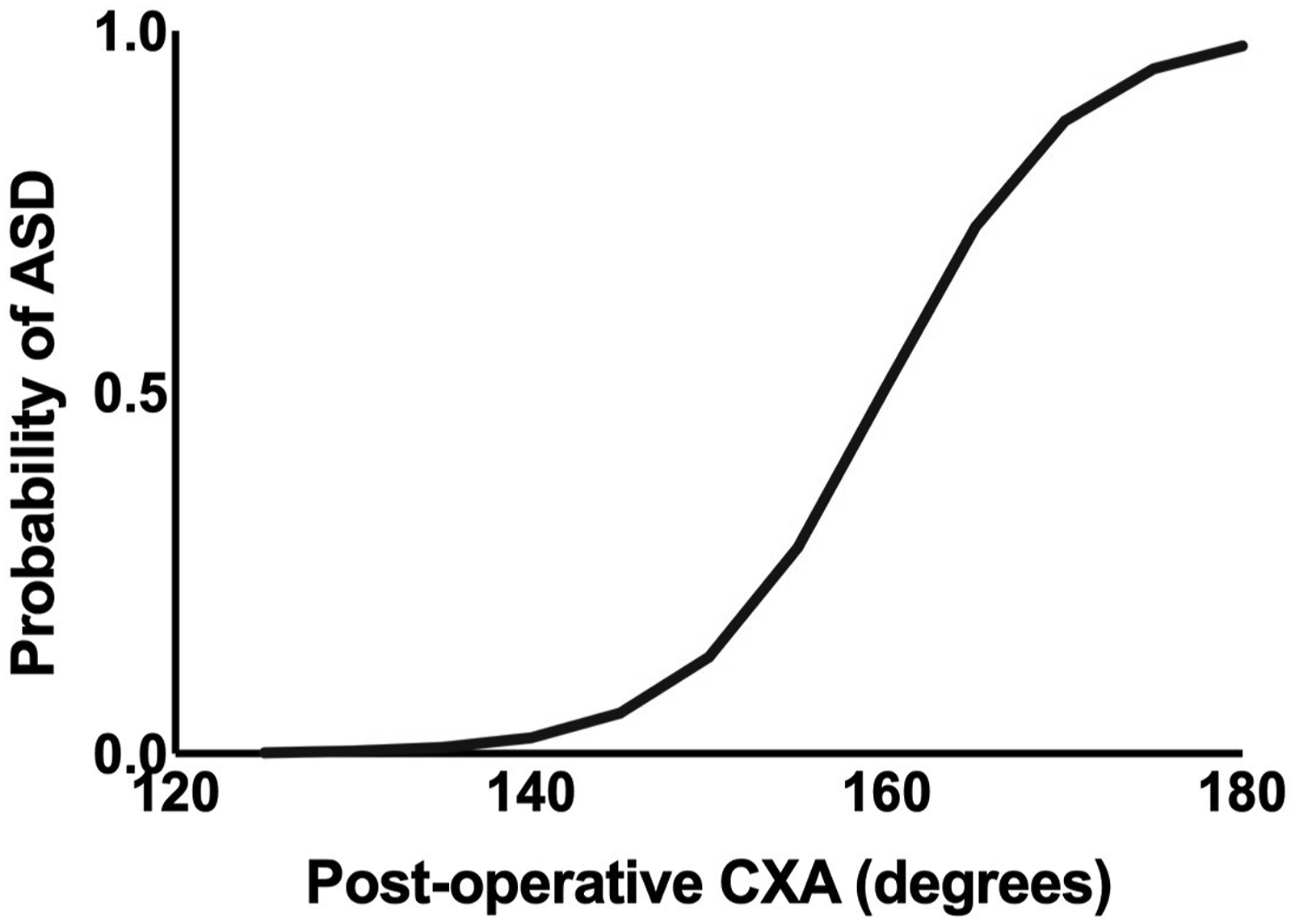
Discussion
Occipitocervical fusion is the standard of care for patients with symptomatic craniocervical instability. 8 In many patients with craniocervical instability surgical correction focuses on extension of the atlantooccipital joint, as baseline flexure at the CVJ results in compression of the cervicomedullary junction. This compression can be associated with central sleep apnea, weakness, or lower cranial nerve dysfunction.9,10 By altering the orientation of the occipitocervical junction and fusing both the atlantooccipital and atlantoaxial joints, occipitocervical fusion alters the biomechanics of the cervical spine, 11 as approximately 50% of flexion-extension and 50% of axial rotation in the cervical spine occur at these two motion segments. The immobilization of these motion segments creates a stress riser at the distal end of the construct, 12 which may predispose this segment to subsequent degeneration, with some series showing ASD in over 1/3 of cases. 13 In the present study, we aimed to assess the relative impact of occipitocervical alignment on the risk of this outcome. We found that for each 1° increase in postoperative clivoaxial angle, there was a 20% higher odds of subsequent adjacent segment disease; patients with a CXA of 155° had a more than 6-fold higher odds of ASD as compared to patients with a CXA of 145°. This suggests that overextension during surgery could substantially elevate the risk of junctional failure. This highlights the importance of optimizing CXA within a target range that balances effective brainstem decompression with the need to minimize mechanical stress on adjacent segments. In practice, surgeons might need to employ more conservative adjustments to CXA, avoiding excessive extension that could predispose patients to ASD and other related complications. These insights could inform preoperative planning and intraoperative decision-making, ultimately improving patient outcomes by reducing the incidence of postoperative junctional failure.
We hypothesize that a reciprocal snaking phenomenon may occur e.g., compensatory biomechanical changes in the cervical spine in response to alterations in CVJ alignment. Specifically, when the occipito-cervical junction is fused in relative extension, the subaxial cervical spine may develop compensatory kyphosis as a mechanism to maintain horizontal gaze and overall sagittal balance. This compensatory kyphosis can increase mechanical stress at the segments adjacent to the fusion, potentially leading to ASD. Biomechanical studies have demonstrated that changes in the alignment of one spinal region can lead to compensatory adjustments in other regions to preserve overall spinal balance and posture. 14 For instance, cervical spine alignment is intricately linked to thoracic and lumbar curvature, with changes in one region often resulting in compensatory changes in the others. This interconnectedness supports the idea that fusion in a hyperextended position at the occipito-cervical junction could lead to compensatory kyphosis in the subaxial spine, thereby increasing the risk of ASD. 15 Moreover, the concept of global spinal balance, which emphasizes the importance of maintaining appropriate alignment across the entire spine, underscores the potential impact of even small changes in CVJ alignment on adjacent segments.3,16
Given advances in anti-rheumatologic therapies, there has been a decrease in the prevalence of craniocervical pathology in patients with rheumatoid arthritis, 17 a population that used to comprise a large proportion of all patients undergoing occipitocervical fusion. Consequently, OCF has been increasingly rare and so there is a relative paucity of literature considering the effects of craniocervical alignment on ASD risk in those undergoing OCF. One study by Matsunaga et al examined the association of occipitoaxial alignment on subaxial subluxation in 38 patients who underwent occipitocervical fusion for irreducible atlantoaxial dislocation in the setting of rheumatoid arthritis. 18 Quantifying alignment using the occipitoaxial (O-C2) angle – the Cobb angle defined by McGregor’s line and inferior surface of the C2 body – they found that patients with O-C2 angles differing from those seen in 120 healthy controls had an increased risk of subaxial subluxation. Interestingly though, the authors found that this association was only true for patients with abnormal O-C2 kyphosis, in whom 86% experienced subaxial subluxation, most commonly at the C4/5 segment.
CXA is an alternative strategy for analyzing occipitocervical alignment, with normal values lying between 145 and 160° and ≤135° being considered pathologic. 10 However, there has been no establishment of an optimal CXA with respect to minimizing ASD risk following occipitocervical fusion. 9 And despite increased awareness of the importance of the impact of regional and global misalignment on the development of ASD, there still exists a relative paucity of literature addressing craniocervical alignment. For patients undergoing CCF for brainstem decompression, our results suggest that while a higher CXA may result in improved ventral brainstem decompression, it may also increase the risk for postoperative adjacent segment disease. As the values of postoperative CXA and the change in CXA increased, so did the rates of adjacent level disease (Figure 3). This illustrates the importance of considering optimal spinal alignment parameters for durable treatment results, particularly in patients with low pre-operative CXA.
Both the CXA and the pBC2 are critical parameters in evaluating pathology, especially with regards to cervicomedullary compression. 9 The CXA is especially significant in determining the flexion or extension at the CVJ. Low CXA is correlated with ventral brainstem compression, which can manifest in a variety of neurological symptoms, ranging from headaches to more severe forms of medullary dysfunction.
Similarly, the Grabb-Oakes line is a reliable indicator of ventral cervicomedullary compression, particularly in conditions such as basilar invagination and Chiari malformations. 19 An elevated pBC2 value suggests that the brainstem may be bowstringing over the odontoid process, exacerbating compression and potentially leading to neurological compromise. In this series, subaxial cervical spine kyphosis emerged as the predominant form of adjacent segment disease. Increased craniovertebral angle (CXA) suggests greater extension at the O-C1-C2 complex, which may induce kyphosis as a compensatory mechanism to maintain horizontal gaze. Spinal alignment and gaze are crucial for overall balance, with cranio-spinopelvic parameters and their impact on Health-Related Quality of Life (HRQOL) being well documented. 20 Horizontal gaze facilitates interactions with the environment, hazard avoidance, dynamic locomotion, and social signaling. 21 As skull extension increases, McGregor slope decreases, indicating elevated horizontal gaze and a negative chin-brow vertical angle (CBVA). 22 Consequently, to preserve horizontal gaze, compensatory kyphosis in the subaxial spine develops, regardless of the level of the lower instrumented vertebra, highlighting an issue with overall alignment rather than construct integrity.
Illustrative Case
A 34-year-old man with a history of Ehlers-Danlos Syndrome presented with neck and shoulder pain, headaches, and numbness of the hands. MRI showed a cervical syrinx, pBC2 of 10.2 mm, and CXA of 144° (Figure 5A). He underwent posterior fossa decompression and CCF. After 1 year the patient complained of continued neck pain and CT showed a rod fracture (Figure 5B). Measured CXA was 175° and pBC2 was 4.8 mm. Pre- and postoperative MRI. (A) Preoperative MRI showing a syrinx at the C6/C7 level, pBC2 of 10.2 mm, and CXA of 144°; (B) Postoperative CT showing posterior rod fracture.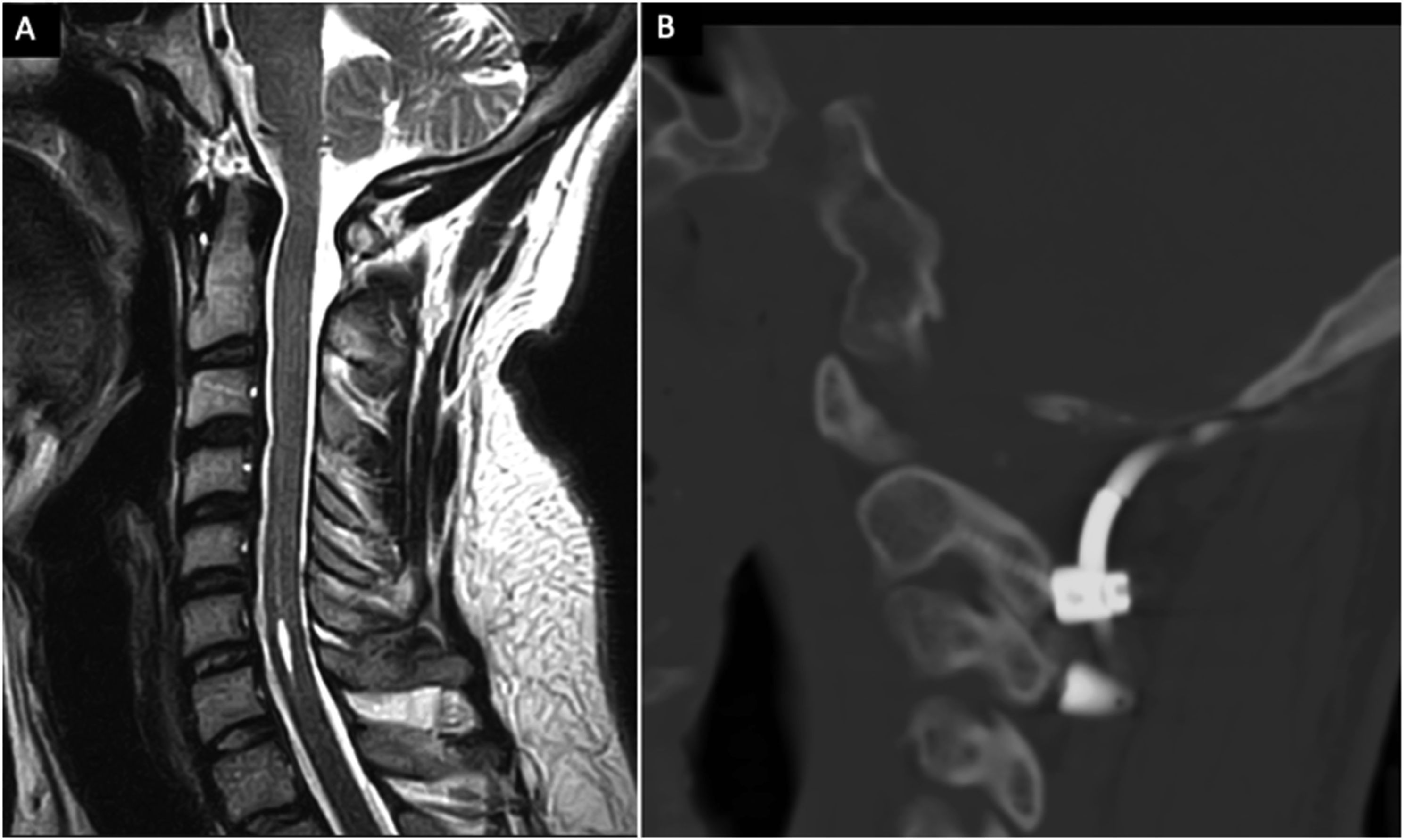
The rod was revised, however 1 month later the patient continued to complain of pain. MRI showed worsened cervical kyphosis with ASD and cervical X-rays showed anterolisthesis at C3-C5 (Figures 6A and 6B). The patient underwent a C3-5 anterior cervical discectomy and fusion with extension of the posterior fusion to C6 with improvement in his neck pain (Figures 6C and 6D). Based on the linear regression model, a pBC2 of 9 could have been achieved with just a 9.8° increase in CXA. This decrease in pBC2, along with direct PFD, may have been sufficient to relieve the patient’s symptoms while reducing the patient’s risk of ASD by approximately 60%. Adjacent segment disease and treatment. (A) MRI showing worsened cervical kyphosis with adjacent segment disease; (B) X-ray showing anterolisthesis of C3-5; 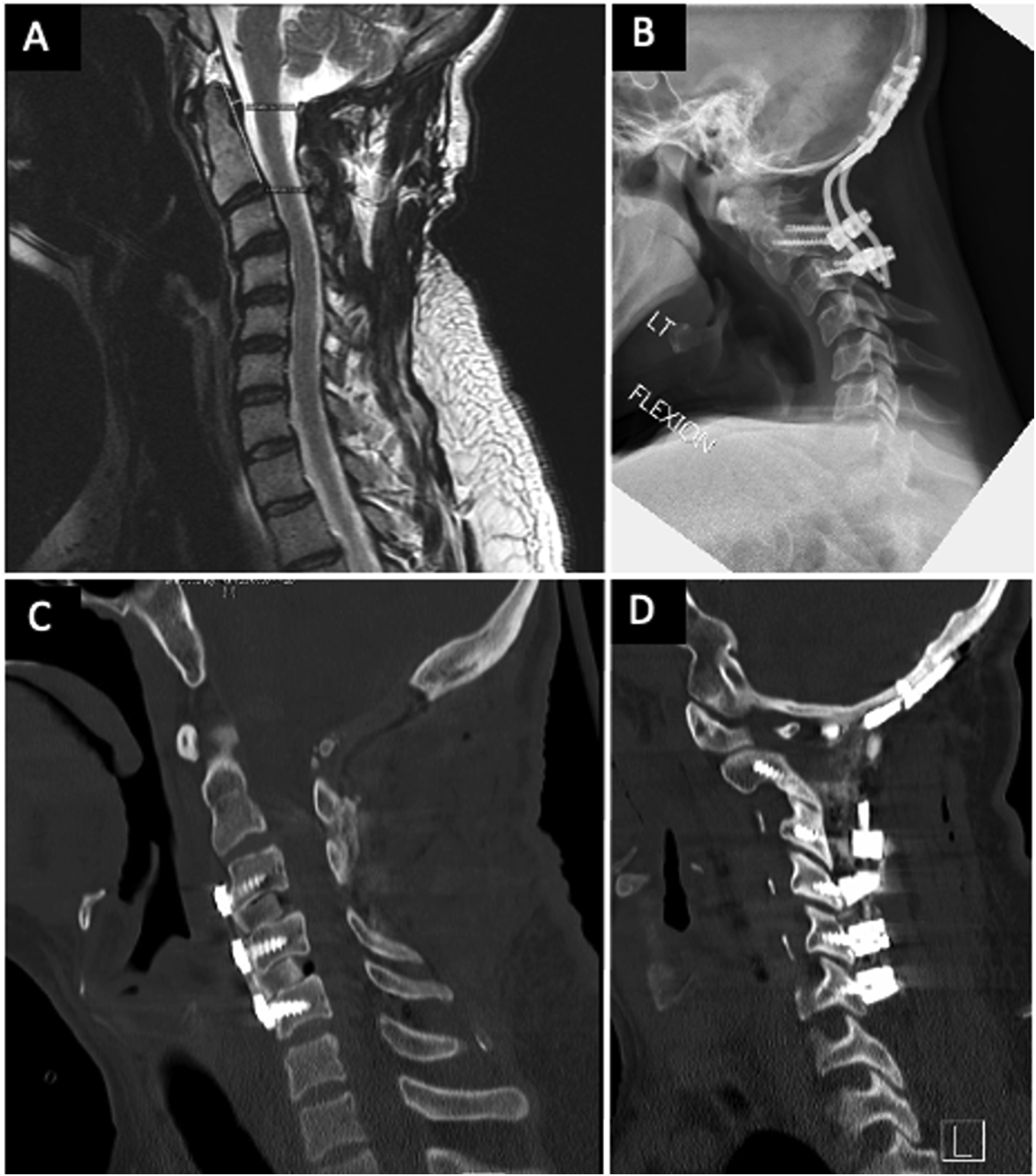
The biomechanical implications of connective tissue disorders in our cohort merit particular consideration. These conditions can affect the tensile strength and elasticity of ligamentous structures throughout the spine, potentially altering the distribution of mechanical stresses across motion segments. In patients with conditions like Ehlers-Danlos Syndrome, as illustrated in our example case, increased ligamentous laxity may accelerate the development of adjacent segment pathology due to altered load distribution patterns. 23 While our sample size precludes definitive subgroup analysis of outcomes stratified by underlying pathology, the presence of connective tissue disorders may represent an important effect modifier in the relationship between postoperative alignment and adjacent segment disease risk. The complex interplay between tissue biomechanics, surgical alignment, and long-term outcomes in this population warrants dedicated investigation in future studies.
Beyond alignment parameters, multiple factors likely influence the biomechanical environment at the craniovertebral junction following fusion. Surgical technique variations may affect the distribution of forces across the construct and adjacent segments. The rigidity of the construct itself - determined by factors like rod diameter, material properties, and cross-connector usage - could theoretically influence the magnitude of stress transfer to adjacent levels. 24 While standardized surgical techniques were employed across our cohort as detailed in our methods, the relative contribution of these technical factors to adjacent segment disease risk remains challenging to isolate in retrospective analyses. Additionally, patient-specific factors such as bone quality, activity level, and cervical muscle strength may modify the relationship between alignment and adjacent segment pathology. 25 Understanding the complex interplay between these variables would require prospective studies with standardized assessment of these parameters.
Limitations
Several limitations of this analysis should be considered. Due to the retrospective nature of this study and limited access to historical clinical documentation, we were unable to comprehensively assess the symptom status of patients who developed ASD. The relatively small sample size of the ASD cohort (10 cases) may reduce the statistical power and generalizability of our findings. Importantly, this low event rate precluded multivariate analysis, which could have better controlled for potential confounding factors. The exclusion of patients who lacked complete imaging could introduce selection bias into the study. By excluding these patients, the study sample may not fully represent the broader population of individuals undergoing craniocervical fusion.
Given the retrospective nature of our data collection, we were unable to precisely discern the timing of complications in relation to the surgical procedure. This limitation arises from the fact that our study did not employ a standardized prospective imaging interval or surveillance protocol. Additionally, the use of various imaging modalities for postoperative measurements, while necessary for comprehensive evaluation, may introduce some measurement variability. While this approach enabled us to capture a broad range of postoperative outcomes, it also means that specific temporal relationships between surgery and the development of complications were not systematically documented. Consequently, no definitive causal relationship can be established between postoperative craniocervical alignment and risk of adjacent segment disease distal to the fusion construct.
Additionally, there may be institutional practices with regard to suboccipital muscle exposure, C2 screw placement technique, and occipital fixation that could alter post-surgical ASD risk, but which may not be seen in a more generalized population. Additionally, while our cohort included patients with connective tissue disorders, limitations in historical clinical documentation prevented accurate determination of the precise prevalence of these conditions in our study population. Future prospective studies with standardized documentation of underlying diagnoses would better characterize the impact of these disorders on outcomes. As such, the results may not be generalizable to patients undergoing occipitocervical fusion for other indications, including trauma (e.g., occipitocervical dislocation), infection (e.g., tuberculosis), or tumor. Last, nearly all patients in the present cohort underwent occiput-C2 instrumentation; only one patient underwent longer segment fusion and so the degree to which occipitocervical alignment affects the odds of ASD in the setting of long-segment occipitocervical fusion is unclear.
Future Directions
The findings of this study highlight several avenues for future research that could further enhance our understanding of CCF and its impact on ASD. First, larger, multicenter trials are needed to validate our findings in more diverse patient populations. Given that our study was conducted at a single institution with a relatively small sample size, expanding the research to include a broader range of patient demographics and underlying conditions would help to generalize the results. Such studies could particularly benefit from including patients with varying degrees of craniovertebral junction CVJ instability, different underlying etiologies (i.e., trauma or congenital conditions), and standardized prospective imaging protocols. Studies like those conducted by Matsunaga et al. have shown the importance of considering various patient populations when evaluating surgical outcomes in craniocervical fusion, suggesting the need for broader research to confirm these results. 18
Second, long-term studies focusing on patient-reported outcomes and quality of life measures would provide valuable insights into the clinical significance of our findings. While this study primarily focused on radiographic outcomes, understanding how variations in postoperative CXA and pBC2 influence functional outcomes over time is critical. Future research could explore whether optimizing these alignment parameters not only reduces the incidence of ASD but also improves patients’ overall functional status and quality of life in the years following surgery, similar to the findings in studies on long-term outcomes of spinal surgeries.3,4 Another promising area of research lies in the development of novel surgical techniques aimed at minimizing the risk of ASD while optimizing craniocervical alignment. For example, intraoperative imaging advancements could allow for more precise adjustments of CXA, ensuring that alignment is within an optimal range that balances effective brainstem decompression with the mechanical demands of the subaxial cervical spine. 9 Additionally, exploring the use of dynamic stabilization techniques or customized fixation hardware that better accommodates individual patient anatomy could reduce postoperative complications, as suggested by biomechanical studies. 12
Biomechanical modeling and simulation represent another critical avenue for future exploration. By developing detailed models of the cervical spine, researchers could simulate various surgical scenarios to predict the effects of different alignment strategies on the cervical spine’s biomechanics. 14 Such models could help refine surgical approaches and improve the accuracy of preoperative planning. Finally, the concept of personalized medicine could be applied to the surgical management of craniocervical instability. Future studies could investigate the feasibility of tailoring surgical goals, such as the target CXA, to individual patients based on their specific anatomical and pathological characteristics. 10 This personalized approach could potentially improve outcomes by accounting for the unique biomechanical environment of each patient’s spine.
Additionally, as larger datasets become available through multi-institutional collaboration, advanced analytical approaches including predictive modeling could further refine our understanding of risk factors for adjacent segment disease. Such approaches could potentially integrate multiple variables including alignment parameters, patient characteristics, and surgical factors to develop more sophisticated risk stratification tools for clinical decision-making.
These future directions not only build upon the findings of this study but also open new pathways for improving the surgical management of patients undergoing craniocervical fusion. As research in this area continues to evolve, the potential to enhance both surgical outcomes and patient quality of life is substantial.
Conclusions
This preliminary study suggests an association between occipitocervical alignment following craniocervical fusion and the development of adjacent segment disease. Specifically, patients who are fused in relative extension, as measured by an elevated postoperative CXA, appear more likely to develop ASD. While our findings show statistical significance, the relatively low event rate limits more complex statistical analyses that could better control for potential confounding factors. Our observations regarding postoperative alignment and ASD risk should be considered hypothesis-generating, requiring validation through larger, prospective studies with standardized imaging protocols and longer follow-up periods. Such future research is needed to better establish the relationship between postoperative alignment and clinical outcomes, and to determine optimal alignment parameters that balance the goals of neural decompression with biomechanical stability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.