
Abstract
Study Design
Case report.
Objective
This case exemplifies the importance of a high index of suspicion when dealing with intractable pain and neurologic symptoms in patients with a history of cancer. Fallopian tube cancer is relatively uncommon, accounting for less than 0.2% of all female malignancies. Because of a low index of suspicion, it is often detected at an advanced stage. From an orthopedic perspective, osseous metastasis from primary fallopian tube malignancies is rare with only a few documented cases in the medical literature.
Methods
This case report documents a 68-year-old woman who developed back pain and leg weakness after undergoing surgical resection with adjuvant therapy of a primary fallopian tube adenocarcinoma. Her hospital course and follow-up are documented.
Results
Imaging revealed a compression fracture in the L1 vertebral body that when a biopsy confirmed a soft tissue diagnosis of a high-grade serous papillary adenocarcinoma of fallopian tube origin. The patient underwent a surgical decompression, posterior stabilization, and tumor debulking with postoperative resolution of her symptoms.
Conclusions
This is the first reported case of a spine metastasis from a fallopian tube serous carcinoma in a living patient. This case documents the diagnosis of a pathologic vertebral fracture due to metastasis of an atypical cancer.
Keywords
Introduction
Osseous metastasis from primary fallopian tube malignancies are rare with only a few documented cases in the medical literature. 1 , 2 In addition, to our knowledge, there are currently no documented symptomatic cases of primary fallopian tube carcinoma metastases to the spine. A review of the literature demonstrates that there is an important place for surgical treatment of symptomatic spinal metastasis. 3 , 4 , 5 , 6 , 7 This case report illustrates a 68-year-old woman with a compression fracture in the L1 vertebral body that when biopsied confirmed our suspicions of a metastatic fallopian tube cancer, which was operatively repaired.
Case Report
A 68-year-old African American woman presented to the hospital with intractable back pain and lower extremity weakness. Her back pain began about a year prior, but gradually worsened during the weeks before her admission to the hospital. She also developed a progressive left lower extremity weakness a week prior to admission that eventually caused a significant disability including leg buckling. She has a history of fallopian tube cancer with positive right axillary lymph nodes diagnosed in 2009 that warranted an exploratory laparotomy, hysterectomy, and bilateral salpingo-oophorectomy with radiation and chemotherapy. Notably, she had a remote 20 pack-year history, and her grandmother and aunt were diagnosed with breast cancer.
Physical examination demonstrated a distended abdomen and paraspinal tenderness around T12–L1. Her neurologic examination revealed left hip flexor strength at 2/5 and left quadriceps strength at 4/5. Right lower extremity strength was 5/5 in all muscle groups tested. Sensation was intact to light touch and pinprick, and reflexes were 1+ and symmetric throughout. A CT scan of the lumbar spine revealed an L1 pathologic compression fracture with moderate to severe canal narrowing (Fig. 1). Magnetic resonance imaging of her lumbar and thoracic spine demonstrated soft tissue extension of the L1 tumor going into the canal and toward T12 (Figs. 2 and 3). Also, a large mass was noted in her left retroperitoneal space.
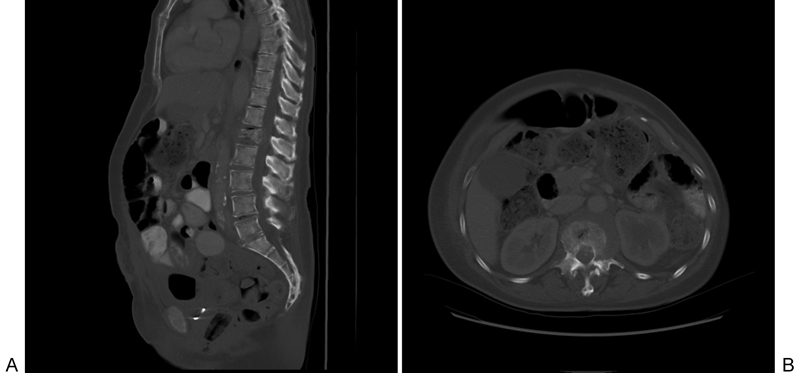
Preoperative computed tomography with sagittal (A) and axial (B) views demonstrating a compression fracture of the L1 vertebral body.
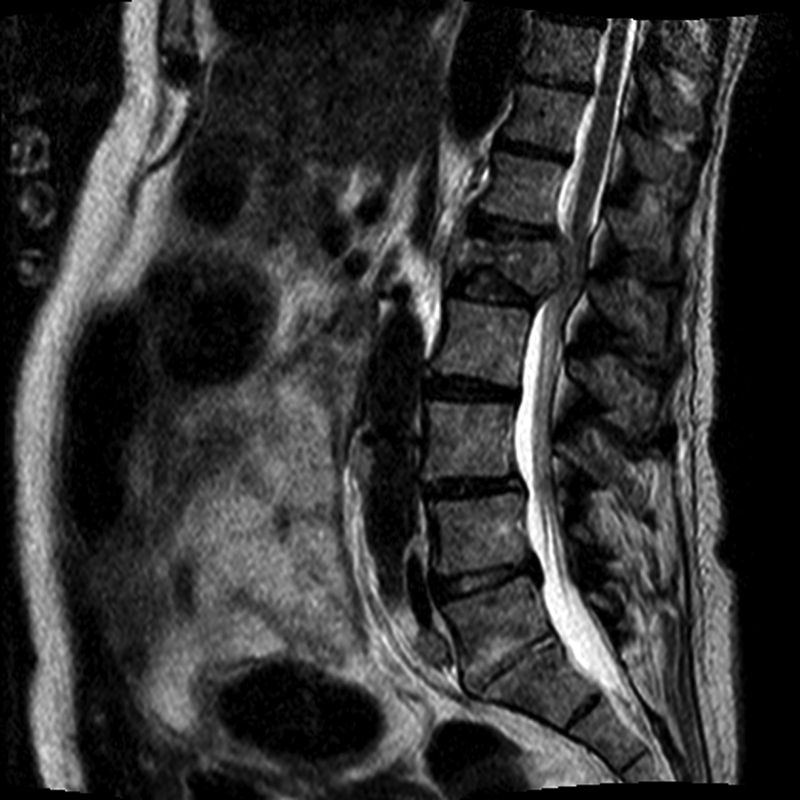
Preoperative sagittal T2-weighted magnetic resonance imaging demonstrating a compression fracture of the L1 vertebral body and impingement of the conus medullaris and nerve roots of the cauda equina.
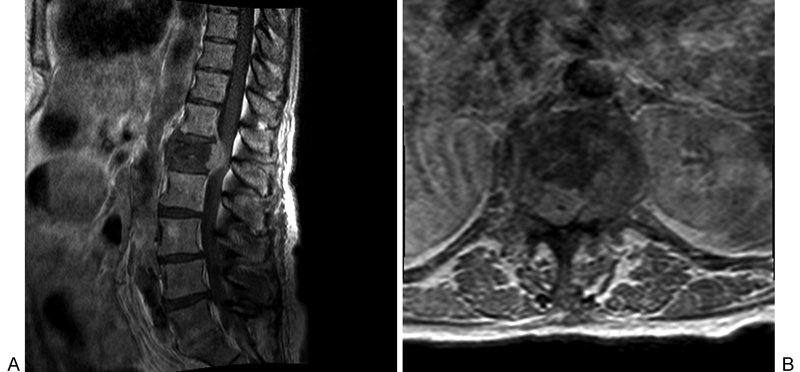
Preoperative T1-weighted magnetic resonance imaging with gadolinium-based contrast with sagittal (A) and axial (B) views demonstrating a compression fracture of the L1 vertebral body and impingement of the conus medullaris and nerve roots of the cauda equina.
The history, physical, and imaging studies were highly suspicious for a recurrence of her fallopian tube cancer, and the mass was biopsied. Interventional radiology performed the biopsy, revealing a high-grade serous papillary adenocarcinoma of fallopian tube origin, warranting surgical intervention (Fig. 4). This pathology was confirmed with the specimen sent at the time of surgery. Prior to the procedure, preoperative embolization was performed to control the feeders and to minimize the blood loss. We performed a midline posterior procedure, which included a laminectomy from T12 to L2 followed by L1 corpectomy and reconstruction with a Synthes polyetheretherketone expandable cage and DePuy expedium screws for posterior fixation packed with autograft followed by posterior instrumented arthrodesis of T9–L4. Tumor removal was complicated by adhesions to the spinal cord, aorta, and kidney as well as brisk bleeding during the removal of the tumor and vertebral body. She was then treated with chemotherapy and radiation.
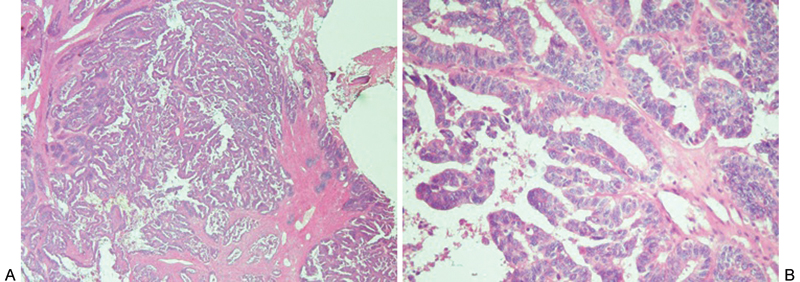
Histologic specimen originating from the patient's spine (A; hematoxylin and eosin, 40×) demonstrating a metastatic papillary carcinoma and (B; hematoxylin and eosin, 200×) demonstrating complex papillae with epithelial budding and marked nuclear atypia, consistent with high-grade serous papillary adenocarcinoma.
The patient's symptoms resolved postoperatively with no complications. At her 6-month follow-up visit, she was able to ambulate without a cane and maintained 5/5 bilateral lower extremity strength. The postoperative X-rays demonstrate the spinal reconstruction and fixation at 6 months (Fig. 5).
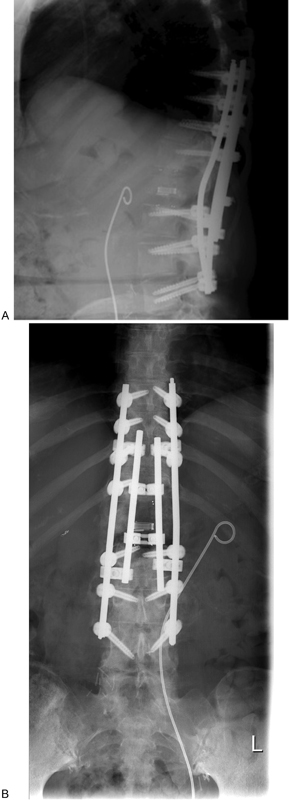
Anteroposterior (A) and lateral (B) X-rays demonstrating instrumented fusion at 6-month follow-up.
Discussion
Primary fallopian tube malignancies are rare, representing less than 0.2% of all malignancies diagnosed in women. 8 They are usually diagnosed at an advanced stage, with 72% of fallopian tube malignancies being diagnosed at stage III or higher. 9 Clinically and histologically, fallopian tube cancer resembles epithelial ovarian cancer and is generally managed in the same manner. 8 However, because fallopian tube cancer is less common and has a low index of suspicion, treatment is often delayed. 10 Management guidelines suggest surgical removal of the gross disease usually accompanied by adjuvant radiation or chemotherapy. 11
Skeletal metastasis from a primary fallopian tube malignancy is an even more infrequent occurrence with only a few documented cases in the medical literature. In a clinicopathologic study of 305 patients with gynecologic carcinomas, 49 patients had evidence of skeletal metastasis, but only one of these cases came from a patient with primary fallopian tube carcinoma. 2 This lesion was detected during autopsy in the vertebrae of a patient with high-grade stage II papillary serous adenocarcinoma with widespread metastasis. 2 Courville et al reported a case of a 56-year-old woman with metastasis of a fallopian tube cancer to the right femur and left eighth anterior rib. The patient received a trochanteric intramedullary nail and also underwent chemotherapy and radiation therapy to the right femur and left anterior ribs with a good clinical outcome. 1 To our knowledge, after an exhaustive PubMed search, this is the only documented case of symptomatic spinal metastasis from a primary fallopian tube carcinoma. Despite the advanced nature of this patient's disease, this case illustrates that pathologic spinal fractures from metastatic primary cancer can be treated surgically at a late stage with good clinical outcomes.
Conclusion
This is the first reported case of spine metastasis from a fallopian tube serous carcinoma in a living patient. This is a rare entity, but this case exemplifies the importance of a high index of suspicion when dealing with intractable pain and neurologic symptoms in patients with a history of cancer. It also highlights the vital role of clinical, radiologic, and histologic correlation in the diagnosis of a pathologic vertebral fracture due to metastasis of an atypical cancer.
Disclosures
Jonathan P. Eskander, none
Eren O. Kuris, none
Andrew J. Younghein, none
Samuel Landsman, none
Leonard Japko, none
Mark S. Eskander, none