
Abstract
Study Design
Case report and literature review.
Objective
Spinal subdural hematomas are rare events that often progress with severe neurologic deficits. Although there have been several case reports in the literature of spontaneous spinal subdural hematomas in the setting of anticoagulation, antiplatelet therapy, or coagulation disorders, the exact pathophysiology of such phenomena remains obscure.
Methods
We present the first report of a subdural hematoma after a percutaneous vertebroplasty and provide a comprehensive review on the anatomy of venous drainage of the vertebral bodies with emphasis on the possible effects of venous congestion caused by cement obstruction.
Results
Because the subdural hematoma occurred in the absence of major cement extravasation to the spinal canal and two levels above the site of the vertebroplasty, we discuss the possible role of venous congestion as the main etiologic factor leading to rupture of the fragile, valveless radiculomedullary veins into the subdural space.
Conclusions
The reported case supports a possible new pathophysiological scheme for the development of spinal subdural hematoma in which venous congestion plays a pivotal etiologic role. The reported findings suggests that future anatomical and histologic studies investigating the response of the radiculomedullary veins to congestive venous hypertension may shed new light into the pathophysiology of spinal subdural hematomas.
Keywords
Introduction
Spinal subdural hematomas (sSDHs) have been reported to occur after minor trauma, lumbar puncture, spinal anesthesia, 1 or spinal surgery, especially in the presence of intraoperative dural tears. 2 Nontraumatic (spontaneous) sSDHs are much more rare, with a recent review having identified 106 cases reported in the English literature. 3 Several predisposing factors have been associated with the occurrence of spontaneous sSDHs, such as coagulation abnormalities, anticoagulation therapy, 4 platelet dysfunction, 5 polycythemia vera, 6 pregnancy, 7 arterial wall abnormalities, 8 and, more rarely, the presence of spinal arteriovenous malformations. 9
Most sSDHs occur at the lower thoracic region (the second most common location being the upper cervical spine) and typically extend from two to five segments. 10 The vast majority of sSDHs are located anteriorly to the spinal cord, while most epidural spinal hematomas are located posteriorly to the spinal cord. 11 This difference is related to the fact that the posterior longitudinal ligament closely adheres to the vertebral bodies, thus limiting anterior epidural collections. Interestingly, the vast majority of case reports on operated sSDHs identified no intermingling between the subdural blood and the cerebrospinal fluid (CSF). Because the hematoma is confined to the extra-arachnoid space, some authors have suggested that what is commonly designated as an sSDH is, in fact, a dissection between the two inner layers of the spinal dura. 12 This concept is supported by anatomic studies that demonstrated that under physiologic conditions, the spinal subdural space is only a “capillary slit,” which may occasionally extend into a genuine space under pathologic conditions such as during a subdural bleeding.10,13
Percutaneous vertebroplasty is a therapeutic strategy that has gained increasing interest in the neurosurgical community for the treatment of refractory axial mechanical pain in patients with vertebral compression fractures. One of the main therapeutic mechanisms of cement augmentation has been proposed to be the improvement in the spinal stability provided by the injection of polymethyl methacrylate (PMMA) into the fractured vertebral body. 14
Several complications of vertebroplasty have been reported in the literature, with the vast majority of them being related to cement extravasation to the epidural canal leading to spinal cord compression (some series report extravasation rates of up to 20% with approximately one-third of such patients being neurologically symptomatic and requiring surgical intervention) 15 or related to cement migration through the epidural veins to the venous system leading to pulmonary embolism (reported to occur in 0.8 to 2.1% of the patients, with the vast majority of patients being asymptomatic). 16 In this context, the severity grade of the fracture and a low viscosity of PMMA cement have been identified as strong and independent risk factors for cement leakage. 17
In this article, we report a patient who developed an acute sSDH following a percutaneous vertebroplasty without signs of major cement extravasation to the spinal canal. This is the first report of such a complication after percutaneous vertebroplasty. The authors perform a comprehensive literature review on the pathophysiology of sSDH and highlight the specific nuances of the presented case report to support a new hypothetical role of venous congestion as a possible etiologic factor involved in the pathophysiology of sSDH. Finally, directions for future experimental and clinical research for further investigation of such hypothesis are also delineated.
Case Report
A 49-year-old woman presented to the outpatient clinic with complaints of axial midthoracic pain and a history of a recent fall down the stairs. At that time, the computed tomography (CT) scan of the thoracic spine demonstrated a T8 compression fracture affecting mainly the midportion of the vertebral body, with preservation of the posterior cortex (Fig. 1A). She was treated conservatively with a TLSO brace and analgesics. However, at the 3-months follow-up, she still presented with episodes of severe, deep axial pain centered on her midthoracic spine. The pain was essentially mechanical in nature, with worsening of the symptoms with activity and partial improvement with bedrest. Her visual analog scale for back pain was 5/10 and 0/10 for leg pain. The 3-months follow-up X-ray demonstrated progression of the compression fracture with further loss of height especially in the anterior third of the vertebral body leading to worsening of the kyphotic deformity (Fig. 1B).
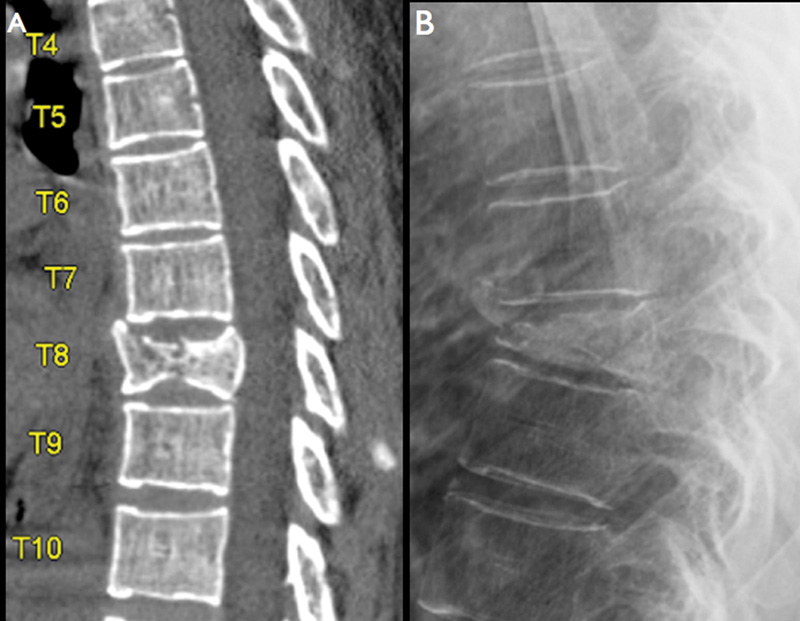
(A) Initial sagittal computed tomography scan demonstrating a T8 compression fracture affecting mainly the midportion of the vertebral body, with preservation of the posterior cortex. (B) Lateral plain X-ray of the thoracic spine performed at the 3-months follow-up after failed conservative treatment demonstrating progression of the fracture with further loss of height especially in the anterior third of the vertebral body, leading to worsening of the kyphotic deformity.
The patient was referred for percutaneous vertebroplasty. The procedure was performed under general anesthesia. After cannulation of the left T8 pedicle and the initial injection of PMMA, a small posterior extravasation of cement to the epidural veins was observed (Fig. 2A). At that point the injection was stopped and the general anesthesia was reversed. After awaking, the patient presented diffuse numbness on the left side (both in the superior and inferior limbs) as well as diffuse weakness (strength 3/5) in the left leg. An immediate CT scan demonstrated only a very small posterior leakage of PMMA toward the epidural space as well as into the adjacent costotransverse joint (Fig. 2). However, it was possible to observe a hyperdense collection anterior to the spinal cord beginning one level above the site of the vertebroplasty and extending up to the cervical spine. The presence of pneumorrhachis at a point distant to the level of the vertebroplasty was also identified.
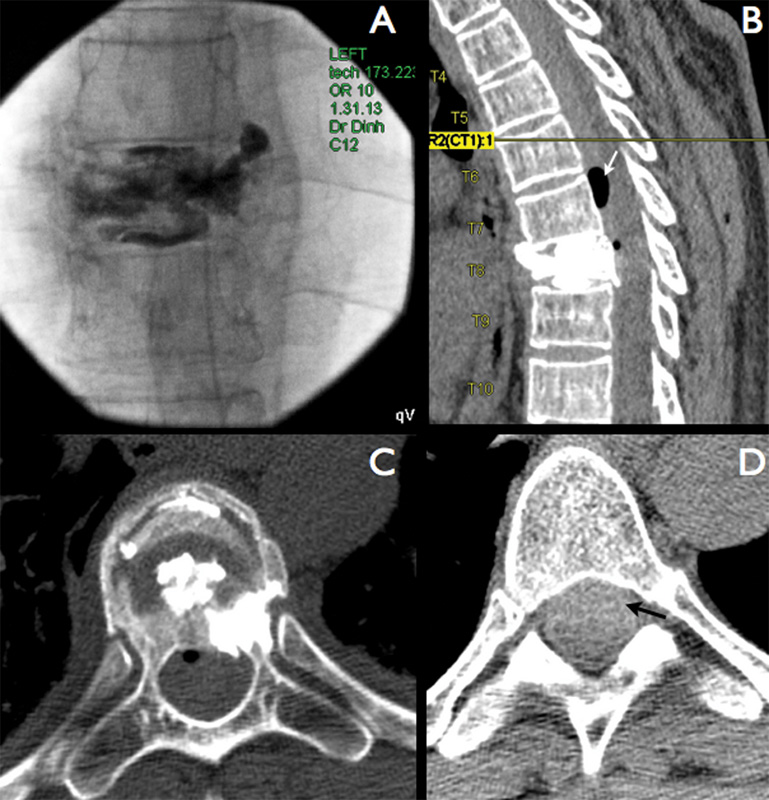
(A) Intraoperative fluoroscopy demonstrating a small extravasation of cement to the posterior epidural veins in the most superior region of the vertebral body. Immediate postprocedure (B) sagittal and (C) axial computed tomography scans demonstrating only a very small posterior leakage toward the spinal canal, as well as the presence of (D) a spinal subdural hematoma (black arrow) extending from one level above the vertebroplasty to the lower cervical spine. Note also the presence of pneumorrhachis (white arrow).
Due to the acute motor deficit in the left lower limb, the patient was submitted to an immediate decompressive laminectomy at the level of the vertebroplasty and extending one level above and one level below to encompass those levels in which the cross-sectional area of the spinal canal was significantly compromised. No major compression of the thecal sac or epidural bleeding was identified during the surgical procedure.
The postoperative magnetic resonance imaging (Fig. 3) confirmed the presence of a collection with imaging characteristics of an sSDH, beginning one level above the vertebroplasty and extending up to the lower cervical spine, but without any residual signs of compression, as demonstrated by the presence of CSF posterior to the spinal cord (Fig. 3B and D).
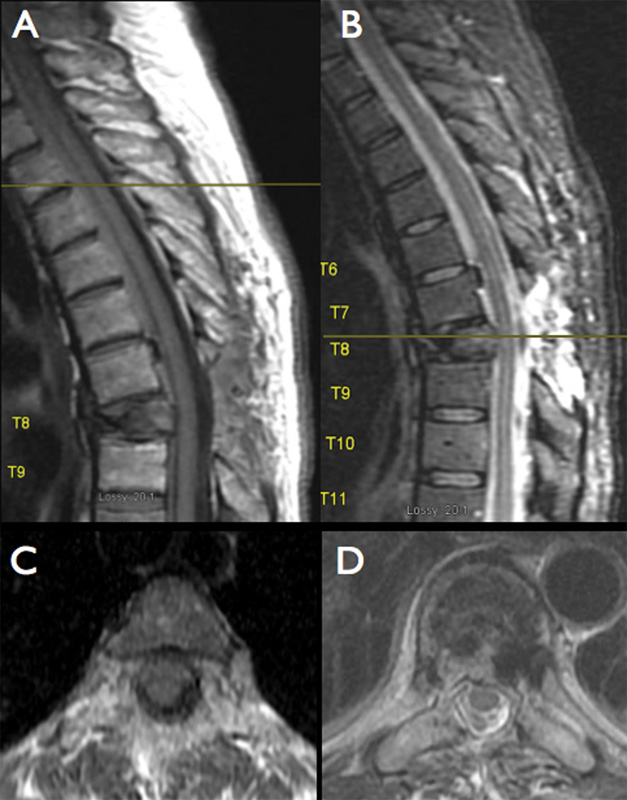
Sagittal postoperative magnetic resonance imaging of the thoracic spine. The subdural collection is located anterior to the spinal cord and extends up to the cervical spine. The acute spinal subdural hematoma is hyperdense in both T1- (A) and T2-weighted imaging (B). The axial images demonstrate no residual compression either at the laminectomy level (C) or in the levels above (D) as evidenced by the presence of cerebrospinal fluid posterior to the spinal cord.
After physical therapy and rehabilitation the patient progressively recovered the motor function in the left leg. At the 3-months follow-up, she presented with almost complete recovery of her strength in the left leg (grade 4+/5 for hip flexion, hip extension, leg flexion and extension, and dorsiflexion and plantar flexion), although the sensory symptoms still persisted in the whole left side, both in the superior and inferior limbs, requiring treatment with gabapentin.
Discussion
Anatomy of Spinal Venous Drainage
The vertebral venous plexus is a complex, large-capacity, plexiform venous system that is believed to play an important role in the regulation of intracranial pressure with posture changes. Additionally, due to this plexus’ valveless, bidirectional flow, it also provides a direct route for tumor or infection dissemination from the pelvic and lower lumbar region to the thoracolumbar spine. The fact that the vertebral venous plexus appears to be much larger than what would be expected for the drainage of the spinal cord and meninges has led some authors to suggest that this vascular bed may also function as an alternate route for venous blood drainage between the inferior and superior vena cava. 18 , 19 Moreover, the fact that such a large plexus does not contain valves has led some authors to infer a possible secondary role as a pressure-regulating system that can protect the spinal cord from the volume and pressure peaks occurring in the intra-abdominal, intrathoracic, intracranial, and intraspinal spaces. 10 , 11
The anatomy of the vertebral venous plexus has been somewhat ignored by ancient anatomic reports and only received the due attention in recent centuries; special acknowledgments must be given to the works of Batson (1894–1979), after whom this venous plexus is named, and Breschet (1784–1845). 20 The vertebral venous plexus has been classically divided into an internal (intradural) vertebral plexus (which possesses an anterior and a posterior component) and an external (or epidural) vertebral plexus. Recently, it has been demonstrated that the epidural vertebral plexus is closely connected to the intracranial venous sinuses in what could be described as the cerebrospinal venous system, 21 or the so-called extradural neural axis compartment. 22
In relation to the vertebral bodies, several small subsystems of plexiform veins work synergistically to accomplish their venous drainage (Fig. 4). The basivertebral system, which is arranged horizontally in the middle of the vertebral body, forms a large-scale venous grid into which the vertical veins of the vertebral body flow from above and below. The main vertical venous channels are of large caliber and present tortuous courses. The subarticular collecting system is another important plexus formed by large-caliber vertical tributary veins, which abruptly turn to run horizontally, parallel to the vertebral endplates, ultimately draining posteriorly into the epidural venous plexus. 23
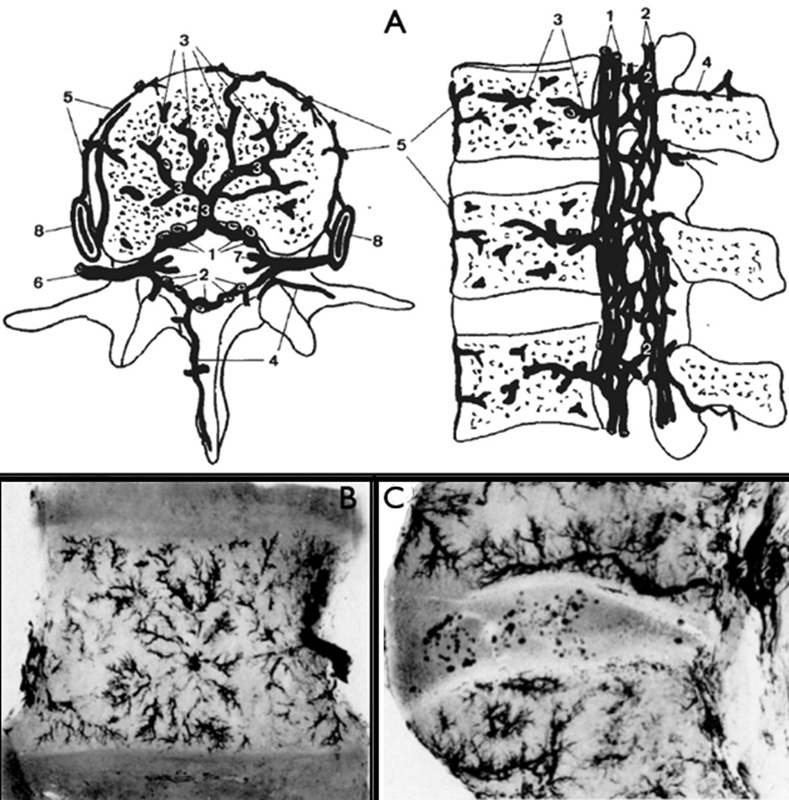
(A) Schematic representation of the vertebral venous system, which can be divided into an internal vertebral plexus (composed of 1: anterior internal vertebral venous plexus; 2: posterior internal vertebral venous plexus), and an external (or epidural) vertebral plexus (composed of 4: posterior external vertebral venous plexus; 5: anterior external vertebral venous plexus; and 8: radicular vein) and the (6) radiculomedullary vein, which connects both. The drainage of the vertebral body is mainly performed by the (3) basivertebral plexus and the subarticular collecting plexus (not shown in this image). (B) A radiograph of a thin coronal section near the central area of a lumbar vertebra. Note the stellate arrangement of tributaries draining into the central vein of the basivertebral plexus. (C) Radiograph of a thin sagittal section cut laterally near the vertebral pedicle. The horizontal subarticular collecting venous system of the vertebral body can be seen running parallel to the inferior vertebral endplate. This system drains by vertical stems through perforations in the vertebral endplates into the larger horizontal subarticular collecting vein system. (A) Reproduced with permission from Groen RJM, Grobbelaar M, Muller CJF, et al. Morphology of the human internal vertebral venous plexus: a cadaver study after latex injection in the 21–25-week fetus. Clin Anat 2005;18(6):397–403. (B and C) Reproduced with permission and copyright © of the British Editorial Society of Bone and Joint Surgery from Crock HV, Yoshizawa H, Kame SK. Observations on the venous drainage of the human vertebral body. J Bone Joint Surg Br 1973;55(3):528–533. 23
Similar to its arterial counterparts, multiple radiculomedullary veins provide segmental drainage to the emerging spinal nerve roots. These radiculomedullary veins run in the same oblique course as the radiculomedullary arteries, but typically arise at different spinal levels. It has already been demonstrated that the radiculomedullary veins constitute the weakest link between the intradural venous system (the internal vertebral venous plexus) and the epidural space (the external vertebral venous plexus).24 Although presenting a small caliber, such radiculomedullary veins are believed to be of crucial importance for the venous drainage of the nerve roots of the cauda equina. In fact, several studies have suggested that the symptoms of neurogenic claudication and radicular pain in patients with lumbar canal stenosis may be more related to venous congestion than to deficits from an impaired arterial supply of the cauda equina. 22 , 25
Although the radiculomedullary veins have already been extensively investigated for their supposed role in the pathophysiology of spinal dural arteriovenous fistulas, 21 very few studies have mentioned their possible role in the etiology of spontaneous or traumatic spinal subdural hematomas. 26 , 27 Moreover, although several previous studies have investigated the general anatomy of the epidural vertebral venous plexus 20 , 28 , 29 , 30 , 31 and the internal vertebral venous plexus, 32 , 33 no specific study focusing on the anatomy of the radiculomedullary veins exists. Additionally, no previous histologic study has investigated the actual vulnerability of such apparently weak connection point between the epidural vertebral venous system and the internal venous plexus, as well as its response to congestive venous hypertension.
Pathophysiology of Spinal Subdural Hematomas
Although several reported cases of sSDH have been associated with minor traumatic events or some predisposing coagulation disorder, the exact pathophysiology of sSDH still remains obscure. Intracranial subdural hematomas have been commonly ascribed to the rupture of subdural bridging veins. However, unlike the intracranial subdural space, it has already been shown that the spinal subdural compartment lacks bridging veins. 34
Interestingly, previous reports have demonstrated the association of sSDH with sudden episodes of increased intra-abdominal or intrathoracic pressure (such as coughing or straining), 26 , 35 , 36 suggesting the presence of a so-called locus minoris resistentiae (a place of lower resistance) in the vascular venous system between the internal and external vertebral venous plexus, which, when submitted to excessive pressures due to venous congestion, would possibly rupture, ultimately leading to extravasation of blood into the subdural space. 35 , 36
Alternatively, some authors have suggested that sSDHs might possibly originate from a few thin and delicate extra-arachnoid vessels that have been identified on the inner dural surface. 37 , 38 Although such etiology might explain some specific cases of sSDH in which the subdural hematoma occurs in association with a subarachnoid hemorrhage of traumatic origin, it does not explain the several reported cases of sSDHs in which it has been confirmed intraoperatively that the blood was confined to the extra-arachnoid space. 39
In the reported case, another factor suggesting an etiology involving venous congestion (related to the obstruction by PMMA of the vertebral venous plexus responsible for the venous drainage of the vertebral body) is the occurrence of neurologic deficits in the absence of signs of spinal cord compression. In the same way, the occurrence of secondary neurologic deficits due to venous congestion and hypoxia secondary to venous outflow obstruction has already been described in a previous report of a patient who presented with reversible myelopathy and spinal cord edema after a traumatic mediastinal hematoma leading to compression of the brachiocephalic vein. 40 Similar neurologic deficits related to intraspinal venous hypertension and hypoxia have already been reported after venous thrombosis and venous outflow obstruction during embolization of spinal dural arteriovenous fistulas. 41 Additionally, the occurrence of a special form of chronic necrotic myelopathy is a well-known phenomenon related to the chronic venous congestion that occurs in patients with spinal dural arteriovenous fistulas (the so-called Foix-Alajouanine syndrome). 42
The appearance of pneumorrhachis (presence of air in the subdural space) in the presented case also supports the hypothesis of a breakdown in the venous system that generated a differential pressure with the surrounding spaces due to its negative intraluminal pressure, ultimately leading to focal accumulation of air in the subdural space. Similarly, previous reports have demonstrated the occurrence of pneumorrhachis in situations associated with an increased intrathoracic or intra-abdominal pressure (such as cardiopulmonary resuscitation and airway obstruction because of foreign body aspiration) leading to hypertensive venous obstruction of the epidural venous system. 43 , 44
Although the management of sSDH is controversial in the literature (with some authors proposing surgery in the acute phase for spinal decompression and hematoma drainage), it has been demonstrated that patients with incomplete neurologic deficits tend to present a positive recovery without drainage of the hematoma. Also, in the absence of radiologic evidence of spinal cord compression (such as in the reported case, in which it was possible to visualize pouches of CSF posterior to the spinal cord in the affected levels), 27 surgical attempts to open the dura and drain the hematoma seem to be of questionable value, especially in extensive lesions involving several levels as in the reported case. 26 In the long term, it has been demonstrated that the physiologic flow of CSF tends to dilute the sSDH, ultimately leading to its spontaneous resolution as observed by follow-up imaging. 26 , 45
Conclusions
This is the first report of an sSDH after a percutaneous vertebroplasty. The occurrence of such a complication in a level different from that of the intervention and in the absence of a major PMMA extravasation into the spinal canal (as well as in the presence of pneumorrhachis) strongly suggests a venous congestive mechanism as the most plausible etiologic explanation. In this article, we propose a new pathophysiological scheme that may explain the development of sSDHs, at least in a subset of patients. This newly proposed etiologic pathway emphasizes the role of venous congestion leading to the rupture of the fragile radiculomedullary veins into the subdural space. Ultimately, this case report highlights the necessity of further anatomical and histologic studies of the radiculomedullary veins to better investigate their behavior in the face of congestive venous hypertension, as well as the supposed relationship between their possible rupture and the development of sSDHs.
Disclosures
Tobias A. Mattei, none
Azeem A. Rehman, none
Dzung H. Dinh, none