
Abstract
Traumatic spinal subdural hematoma is a rare condition mostly favored by an anticoagulation therapy, a traumatic lumbar puncture, a hematologic disease, or an epidural anesthesia. This pathological condition can be subtle or be at the origin of a compression of the spinal cord and the rootlets resulting in an irreversible damage if an emergent surgery is not performed. We report the case of a 45-year-old man who has been a victim of a brain trauma which resulted in a cerebral edema. A week later, the patient came to the emergency department for disabling abdominal pain, predominant in the back. An abdominal computed tomography was performed and showed an incidentally spontaneous hyperdensity in the spinal cord, which raised the suspicion of a spinal hematoma that has been confirmed through spine magnetic resonance imaging. In this case, we discuss the different subtypes of spinal hematoma. We recall the main differential diagnoses to help setting an accurate diagnosis and to not delay the adequate therapy that is most of the time emergent when indicated.
Introduction
Spinal hematomas are a serious pathological problem due to their ability to cause irreversible neurological sequelae if not diagnosed and treated on time. The term spinal hematomas enclose different conditions that are: epidural hematoma, subdural hematoma, spinal subarachnoid hemorrhage (SSAH), and intramedullary hemorrhage. The high resolution of magnetic resonance imaging (MRI) made it the modality of choice to detect spinal hematoma and identify its exact location owing to a methodological approach to the different components of the spine. 1
Case report
A 45-year-old man with no medical history has been a victim of an assault with a head impact and a brief loss of consciousness. The brain computed tomography (CT) has been performed in the nearest hospital and was normal according to him. Patient was kept under observation after an examination by a specialized medical team and got discharged the day after. A week later, while he returned to his hometown, he continued to feel headaches associated with a severe abdominal pain more predominant in the lower back. A new brain and abdominal CT were decided. The brain X-ray scan was a bit artifacted due to the patient’s movements but showed cerebral edema (Figure 1). The abdominal CT showed no particularity at the level of the intra- and retroperitoneal cavity but showed incidentally a spontaneous hyperdensity in the spinal cord respecting the epidural fat, excluding the possibility of an epidural hematoma thus (Figure 2). When a spine MRI was performed, it effectively showed a spinal subdural hematoma, typical of the inverted Mercedes-Benz sign (Figure 3). This hematoma extended from L1 at the level of the lumbar fossae to the terminal part of the dural sac (Figure 3). This case was discussed by a multidisciplinary team of neurosurgeons and radiologists, who, after a thorough examination of the patient, decided on close monitoring. Angiography was suggested to rule out a vascular malformation, but the patient refused. A surgical approach was planned, with the patient’s consent if the symptoms worsened. The patient stayed at the hospital for almost a week till the improvement of the brain edema which was attested by a CT scan, as well as the pain in the back. He was followed-up at close intervals, and spine MRI was performed at the end of the sixth month which was totally normal (Figure 4).

Brain CT showing a cerebral edema consisting of a blurring of the white-gray junction and a scarcity of sulci.

Abdominal CT scan showing a spontaneous hyperdensity surrounding the spinal cord (a; arrows), raising the possibility of a subdural or subarachnoid hematoma, but respecting the epidural fat, it is still hypodense, excluding an apidural hemorrhage (b; arrow).
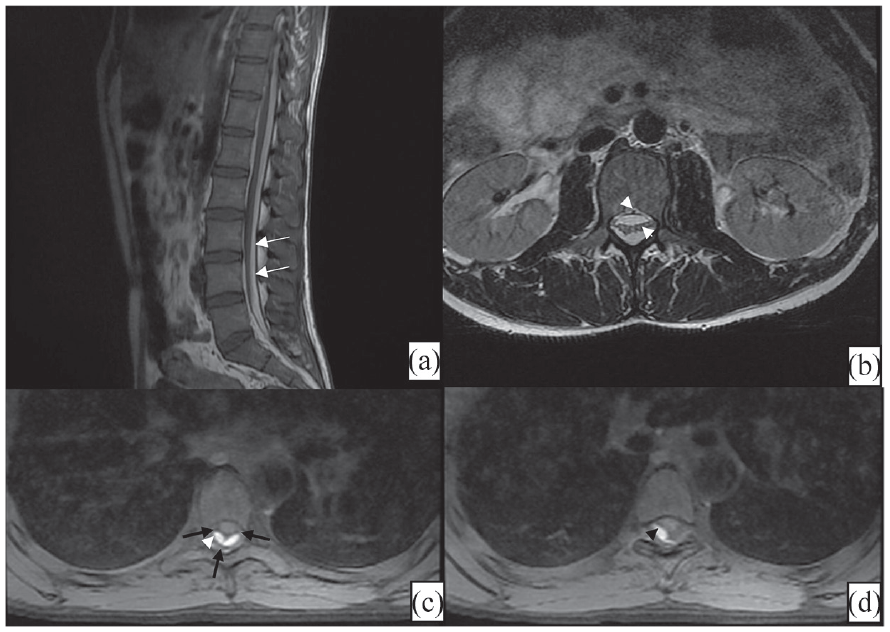
Spine MRI according to sagittal T1 (a), axial T2 (b), and axial T1FS (c,d) showing an hypersignal underlying to the dura mater (white arrows) respecting the epidural fat (a). This hematoma has a mass effect on rootlets that are clumped (b). The incomplete inverted Mercedes-Benz sign is evident on axial images (c, d) attesting the subdural location of this hematoma owing to two lateral denticulate ligaments and a midline dorsal septum (black arrows) generating two posterior collections (arrowheads).

Follow-up MRI of the patient according to the sagittal T1WI, showing the disappearance of the subdural hematoma.
Discussion
Spinal subdural hematomas are less common than epidural ones as the existence of a true subdural space is controversial in the anatomy literature. Contributing factors include anticoagulation, coagulopathy, pain management interventions, surgery, and trauma.2,3
Clinical manifestations are similar, related to the compression of the spinal cord and nerves generating a cauda equina syndrome often preceded by back or radicular pain.
Subdural hematomas are usually of a venous origin explaining the slow onset of symptoms, that are, however, rapidly progressive than those in patients with epidural hematomas. 4
The mechanism of spinal subdural hematoma is not well elucidated as there are no bridging veins in that spinal space. The inner layer of the dura is weak and vulnerable to injuries. One of the possible explanations would be a redistribution of blood from the supratentorial subdural space to the most dependent areas in response to gravitational forces.5–7 The increasing intracranial pressure is thought to result in a shear between the spinal subdural and subarachnoid spaces, leading to a tear of the inner dura and its bleeding. 8 This theory is very plausible, as there are still signs of cerebral edema in our patient. The last possibility remains that of an ignored impact on the lumbar spine when the patient was the victim of the assault, which resulted in a loss of consciousness.
Imaging plays a central role in the diagnosis of the subtypes of the spinal hematoma, as it is difficult to differentiate between them on the basis of the clinical history. CT, as more available, is very useful for the detection of blood as a spontaneously hyperdense crescent-shaped hyperacute hematoma. The respect of the low density of the surrounding epidural fat excludes an epidural hematoma. Nevertheless, in its subacute phase, this hematoma becomes isodense, thus, more challenging to identify and localize. MRI provides the same information than those of CT and allows more details, specially the craniocaudal extent of this hematoma, other possible pathological conditions, and the dating. The appearance of spinal hematoma goes along with that of intracranial one with five described stages of hemorrhage depending on the state of oxygenation of the blood and on the integrity of the red cell membrane (Table 1). Even so, these time frames are estimations, and intensity characteristics may show some degree of variation depending on the tempo of blood degradation from one to another.
The evolution of the appearance of blood on Magnetic Resonance Imaging.

On MRI, spinal subdural hematoma is located within the thecal sac with no displacement of the hypointense dura matter or the epidural fat, and the blood is limited by the denticulate ligaments and the dorsal septum, resulting in the collections of the classic “Mercedes Benz inverted sign.”9–11 When the spinal subdural hematoma is smaller, this sign may miss and the collection may evolve only a part of the thecal sac with mild or no compression to the nerve roots as it is the case in our patient (Figure 3(c) and (d)).
The main differential diagnosis of the spinal subdural hematoma is the epidural one, which, at controversy, extends to the neural foramina and is in direct contact with bone. This distinction is not easy sometimes when the epidural fat is thin anteriorly, but the combination of sagittal and axial images helps assessing the accurate location. The SSAH would not be considered a confusing diagnosis as the sedimentation of blood products in the cerebrospinal fluid (CSF) is a pathognomonic sign easily recognized. 12
Other possible differential diagnoses include subdural abscess and hygroma where the clinical history is of paramount importance. Subdural abscess presents usually with fever and back pain. At imaging, there is a peripheral enhancement with a variable signal, but with no gradient echo susceptibility or hypersignal on T1-weighted images unless blood products are present. Hygroma may occur in patients with a recent history of trauma or intervention leading to CSF entrapment in the subdural space. Differentiation from a located spinal subdural hematoma could be challenging and the radiologist should seek for signs going from a subtle irregularity of the dura matter to a significant leakage responsible of a venous engorgement or a pachymeningeal enhancement raising the suspicion of a tear that would be confirmed on a CT myelography. Epidural lipomatosis is a confusing diagnosis in the subacute phase when the spinal subdural hematoma may appear hyperintense on T1 and T2 WI due to extracellular methemoglobin. However, the slightly different signal, the deep location under the dura matter and particularly the fat-suppressed images rectify the diagnosis. 13
Small spinal subdural hematoma may be mistaken for intradural extramedullary masses, of which the most common are meningioma and nerve sheath tumors that enhance avidly at contrast injection at controversy to hematoma, while arachnoid cyst follows the signal of CSF on all sequences.14,15
Displacement of clumped nerve roots during arachnoiditis may sometimes mimic a spinal subdural hematoma, but they are still totally surrounded by CSF with no visible “inverted Mercedes Benz sign.” 16
The treatment of spinal subdural hematoma has been discussed in literature with two possible attitudes. Spinal angiography may be performed when a vascular malformation is suspected. This approach is particularly useful in the presence of symptoms that have been evolving for a long time, and in the absence of a triggering factor. On the other hand, vascular malformations are rare, occur usually from birth, and are insidiously and progressively symptomatic. The acute manifestation in our patient, and the presence of a trauma are in favor of his decision. The conservative management is chosen when the hematoma is small, the neurological deficit is mild with an early progressive improvement, or when there is a coagulopathy.8,17 The evolution then could be followed through MRI. Surgery consists of a durotomy with an excision of the blood clot and is indicated in cases of significant neurological deficit. In our case, the patient suffered more from abdominal pain accompanied by very subtle paresthesia, and subsequently refused to undergo surgical treatment. We therefore opted for conservative management, which proved successful. Finally, it is important to note that cervical and thoracic locations as well as the coexistence of a SSAH are all factors of poor prognosis.18,19
Conclusion
Spinal subdural hematoma is a serious condition occurring in different situations. Its early suspicion is of paramount importance, allowing an accurate diagnosis and emergent surgical therapy when needed. MRI is the gold standard to set this diagnosis and rule out other mimicking conditions. Thus, the mastery of the anatomy and the imaging characteristics is required from the radiologist.
Footnotes
Author contributions
All authors participated actively in the elaboration of this scientific document: The first author, who’s the correspondent one: wrote the text. The second and third: helped at its elaboration. The other authors set the diagnosis and the latest one, in addition, corrected it.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.