
Abstract
Study Design
Retrospective evaluation of prospectively collected data.
Objective
To compare preoperative and postoperative neck pain following laminoplasty using the Neck Disability Index (NDI).
Methods
Seventy-two patients undergoing laminoplasty from 2006 to 2009 at a single institution were identified. Thirty-four patients with a minimum 1-year follow-up who completed preoperative, 6-week, and 1-year postoperative NDI questionnaires were enrolled. Demographic data and surgical data including estimated blood loss (EBL), length of surgery, number of laminoplasty levels, complications, and length of hospitalization were collected.
Results
Mean age was 62 years (range: 34 to 88), mean follow-up was 17 months (range: 12 to 31), and there were 21 men and 13 women. Diagnoses were cervical spondylotic myelopathy (n = 26), ossification of the posterior longitudinal ligament (n = 6), and central cord syndrome (n = 2). Mean EBL was 120 mL (range: 50 to 200), and mean surgical time was 152 minutes (range: 70 to 240). Average number of laminoplasty levels was 3 (range: 1 to 5). The open door technique was used, and 24/34 (71%) did not have laminoplasty at C3 and C7. No intraoperative complications were noted, and average hospital stay was 1.6 days (range: 1 to 7). Significant improvement in NDI total score was noted at 1 year (p < 0.002) and in NDI pain score at 6 weeks (p < 0.028) and 1 year (p < 0.007) postoperatively.
Conclusions
Patients having laminoplasty experienced significant improvement in NDI pain subscore and NDI total scores at a minimum of 1 year postoperatively.
Introduction
Cervical laminoplasty, a surgical technique pioneered in Japan, is used increasingly in the United States. Axial neck pain following laminoplasty has been previously reported. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 This concern over postoperative neck pain may deter some surgeons from performing laminoplasty. To minimize neck pain following laminoplasty, investigators have recommended performing a laminectomy at C3 rather than laminoplasty to preserve the attachment of the semispinalis cervicis to C2. 10 , 11 , 12 The semispinalis cervicis is an important extensor of the cervical spine, and preserving its attachment to C2 is thought to lead to decreased axial symptoms. Other authors have recommended not doing a C7 laminoplasty to preserve the muscular attachments to the spinous process of C7. 12 , 13 , 14 , 15 , 16
At our center, we routinely perform open door laminoplasty for varying multilevel cervical spine pathologies. 17 For the majority of cases, we avoided performing laminoplasties at C3 and C7 to minimize the risk of axial neck pain. Our objective was to compare preoperative neck pain to postoperative neck pain in patients undergoing cervical laminoplasty.
Materials and Methods
Following institutional review board approval, we performed a retrospective evaluation of prospectively collected data of laminoplasty patients at our institution. We identified 72 patients undergoing cervical laminoplasty from 2006 to 2009. All surgeries were performed by the senior author at a single institution. An independent surgeon, uninvolved in the care of the patients, analyzed the data.
Our inclusion criteria were patients having laminoplasty who completed Neck Disability Index (NDI) questionnaires preoperatively, at 6 weeks postoperatively, and at 1-year follow-up. Demographic information including age at time of surgery, gender, and diagnoses were collected. Surgical data including estimated blood loss (EBL), length of surgery (minutes), number of laminoplasty levels, complications, index versus revision surgery, and length of hospitalization (days) were collected. NDI total scores and NDI pain subscores preoperatively, at 6 weeks and 1 year postoperatively, and/or at latest follow-up were compared.
Our surgical approach to the posterior cervical spine has been described elsewhere. 18 , 19 Our technique for laminoplasty has also been described. 17 Briefly, the patient is positioned prone on the OSI Jackson Table (Orthopaedic Systems, Union City, California, United States) with Gardner-Wells tong traction. We use a bivector traction with one traction rope in-line or horizontal to the patient and the other traction rope with an extension vector. Initially, the in-line traction is attached to 15 lbs and no weight is attached to the extension rope. Transcranial motor evoked potentials and somatosensory evoked potential are used. Microscopically assisted exposure is performed with meticulous dissection, and care is taken to stay in the midline. After incising the fascia, we identify the muscle belly of the semispinalis cervicis and take care to preserve it. For a C3 to C6 decompression, we would expose from the C2–3 interspace to the C6–7 interspace. At C2–3, we are careful not to detach the semispinalis cervicis from the C2. We perform a laminectomy of C3 using a handheld bur and perform the modified open door Hirabayashi technique from C4 to C6, 17 with a plate on the open side. After placing and securing the plates with two screws on the lateral mass and one to two screws on the lamina, we switch the traction to the extension rope. With this maneuver, we ensure there is no overlap or contact of laminoplasty plates on extension. During closure, performed in flexion with the in-line traction, we place a thrombin-soaked sheet of Gelfoam for hemostasis while avoiding areas where dura is directly exposed. 19 We also placed 500 mg vancomycin powder in the wound as recently described and perform multilayered closure over a deep and superficial drain. 18 The multilayered closure is critical, and we start at the muscle layer under the fascia and work superficially, attempting to approximate the muscle bellies anatomically. We routinely use 50 to 100 sutures depending on the depth of the wound. The patient is placed in a soft collar postoperatively for comfort. The soft collar is worn for comfort for 2 weeks. We emphasize to the patient that the soft collar is optional and for comfort only. The patient has no restrictions on cervical range of motion. Physical therapy is not actively initiated for patients during the postoperative period.
Statistical Analysis
Using STATA 11.2 (College Station, Texas, United States), we performed Student t test matched-pair analysis of NDI scores before and after surgery. Significance was set at p < 0.05.
Results
Demographics
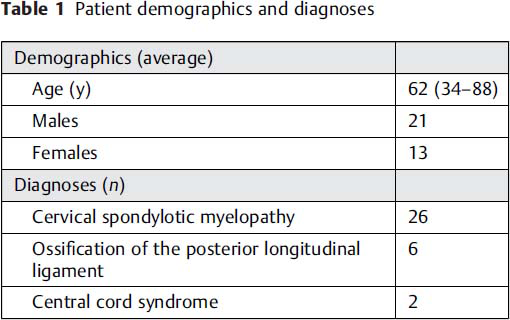
Of our 72 patients, 34 patients met the inclusion criteria from 2006 to 2009. Mean age at time of surgery was 62 years (range: 34 to 88, median 63.5), and mean follow-up was 17 months (range: 12 to 31; Table 1). There were 21 men and 13 women. Twenty-six patients (76.5%) had cervical spondylotic myelopathy, 6 (17.6%) had ossification of the posterior longitudinal ligament, and 2 (5.9%) had central cord syndrome (Table 1).
Patient demographics and diagnoses
Surgical Data
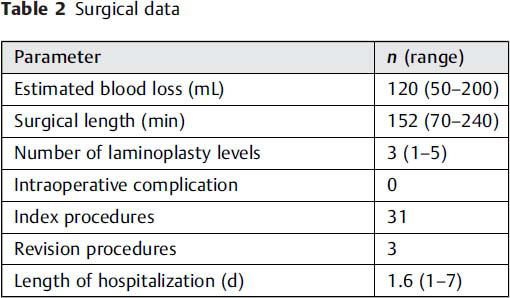
Mean estimated blood loss was 120 mL (range: 50 to 200, median 100), and mean surgical time was 152 minutes (range: 70 to 240, median 152; Table 2). Average number of laminoplasty levels was 3 (range: 1 to 5). The majority of patients, 24/34 (71%), did not have a laminoplasty at C3 and C7. Our practice of not performing laminoplasty at C3 and C7 started after 2006 following the initial reports of possible axial neck pain associated with laminoplasty at these levels. If a C3 decompression was needed, a laminectomy was performed instead of laminoplasty. The cephalad portion of C7 lamina was undercut, if needed. The majority of the cases were index procedures (31, 91.2%), and three were revisions. There were no intraoperative complications. Average hospital stay was 1.6 days (range: 1 to 7, median 1).
Surgical data
Outcome Scores
Preoperative NDI was a mean of 12.5 (median 10; Table 3). Higher scores on NDI indicate increasing disability. NDI improved to a mean of 10.1 (median 10, p < 0.1) at 6 weeks postoperatively and significantly improved to a mean of 8.5 (median 5, p < 0.002) at 1 year postoperatively.
NDI score and NDI pain subscore preoperatively and 6 weeks and 1 year postoperatively

NDI, Neck Disability Index.
The NDI pain subscore was a mean of 1.3 preoperatively and improved to a mean of 0.87 at 6 weeks postoperatively and a mean 0.7 at 1-year follow-up. Compared with preoperative levels, the improvements at 6 week (p < 0.028) and 1 year (p < 0.007) were both significant.
Discussion
Laminoplasty, a surgical technique pioneered in Japan, has gained popularity in the United States during the last two decades. One of the concerns associated with laminoplasty is the issue of persistent or de novo postoperative neck pain. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 For this reason, many spine surgeons have resisted laminoplasty. In our study group with a majority of patients with cervical spondylotic myelopathy, we sought to evaluate preoperative and postoperative neck pain following laminoplasty. Our study is one of few that applied the NDI, 20 a validated outcome measure instrument, to quantify neck pain before and after laminoplasty.
In keeping with the recommended indications for laminoplasty, preoperatively, our patients had relatively low NDI scores (less neck pain). Despite the already low baseline scores, the NDI scores improved significantly postoperatively.
Significant improvements in overall NDI scores occurred at 1-year follow-up compared with preoperative NDI scores (mean: 12.5, median 10; 1 year post-operative mean: 8.5, median 5, p < 0.002). In addition, the values for the NDI pain subscore significantly improved from a mean of 1.3 preoperatively to a mean of 0.87 at 6 weeks (p < 0.028) and a mean of 0.7 at 1 year postoperatively (p < 0.007). Prior to surgery, neck pain was not a significant complaint among our patients (preoperative NDI 12.5, median 10), thus our data do not support the use of laminoplasty to treat patients with myelopathy whose chief clinical complaint is axial pain. However, our data do suggest that neck pain should not worsen after laminoplasty.
In a small prospective randomized study, 21 7 patients undergoing cervical laminectomy and fusion were compared with 9 patients undergoing open door laminoplasty. The NDI was one of the outcome measures used. The laminoplasty group compared with the fusion group was found to have a significant improvement in NDI score postoperatively. This improvement in NDI score is similar to our study's finding, albeit only 9 patients were enrolled in this study compared with the 34 in our cohort.
In a prospective series comparing patients undergoing anterior cervical decompression and fusion (n = 64) to laminoplasty (n = 52), 22 the NDI was also one of the outcomes measures used. In this series at 6 months, the laminoplasty group did not have a significant improvement in NDI score compared with preoperative levels, in contrast to the anterior group. However, at the 2-year follow-up, significant improvements in NDI from preoperative values were noted. In our study, at 6 weeks no significant improvement in NDI score from preoperative values were noted. This lack of initial improvement may be due to the dissection of the posterior musculature and subsequent healing that occurs during the 6-week postoperative period. By the 1-year follow-up, there is significant improvement in the NDI scores because adequate postsurgical healing and recovery have occurred.
Others have examined the issue of axial neck pain following laminoplasty, albeit without using the NDI instrument. Ohnari et al developed their own questionnaire to evaluate axial neck pain following laminoplasty. 6 They administered this questionnaire to 51 patients in addition to collecting the Japanese Orthopaedic Association (JOA) score. They divided axial symptoms into pain, heaviness, stiffness, and other. They noted that 42 of the 51 subjects had postoperative axial symptoms. However, the JOA score did not worsen postoperatively.
Hosono et al compared 37 patients undergoing C3–C7 laminoplasty with 54 patients undergoing C3–C6 laminoplasty. 15 They did not use NDI to quantify neck pain and instead classified it as severe, moderate, and mild. Using this classification, they noted the C3–C7 group had 49% axial neck pain in the perioperative period versus 15% in the C3–C6 group. The authors credit C7 laminoplasty as a source of axial neck pain due to the insertion of trapezius and rhomboid muscles at C7 and connection to the scapula. By disruption of these muscular attachments, axial neck pain may result.
Meanwhile, Takeuchi et al compared C3 laminectomy with C4–C7 laminoplasty and C3–C7 laminoplasty. 10 There were 40 patients in the C4–C7 laminoplasty group versus 16 patients in the C3–C7 laminoplasty group. Preoperative and postoperative axial symptoms were compared using a nonvalidated measure (no symptom, mild symptoms, severe symptoms). They noted that the C3 laminectomy and C4–C7 laminoplasty group had diminished axial symptoms postoperatively compared with the other group. They attribute the preservation of the semispinalis cervicis, which inserts at the C2 spinous process and plays a role in extension, as a critical component to the diminishing axial pain.
Interestingly, in the series of Hosono et al, C3 laminoplasty was routinely performed and C7 laminoplasty was not performed. 15 Meanwhile, in the series of Takeuchi et al, C7 laminectomy was performed routinely. 10 We adopted both practices and no longer perform C3 laminoplasty; instead, we do a laminectomy. At C7, we undercut the top 25 to 30% of the lamina and avoid a laminoplasty, if it is possible to do so without compromising the decompression. For the majority of our cases, 24/34 (71%), we did not perform laminoplasties at C3 or C7. In addition, we performed a multilayered closure of the posterior musculature and fascia, which we have recently described. 18 , 19 The importance of reduction of neck muscle strength leading to axial neck pain after laminoplasty has also been recently described. 9 With the meticulous closure, we aim to approximate the extensor muscles as precisely as possible. We believe the combination of these three techniques resulted in the significant improvement seen in NDI total score and pain score.
Our intraoperative complication rate was 0%. It is plausible that intraoperative or postoperative complications can lead to higher NDI scores postoperatively. C5 palsy occurs in up to 4.8% (5/104) of patients following laminoplasty. 23 However, we did not encounter this complication in this series, although we have had this complication in other series.
Limitations of our study include the small sample size. We performed a post hoc power analysis that demonstrated we needed a sample of 40 (6 more patients) to reach a power of 0.80. However, although slightly underpowered we still believe our study highlights the importance of surgical technique (avoiding C3 and C7 laminoplasty and meticulous muscular approximation) in decreasing the prevalence of neck pain after laminoplasty. Another limitation is our average follow-up of 17 months. With longer follow-up, there could have been a detectable increase in axial symptoms. However, from our review of the literature, the common time span of axial pain following laminoplasty is from the perioperative period to 6 months postoperatively, and we have captured this period in our study. Also, longer-term follow-up may result in new onset of axial neck pain due to ongoing degenerative changes unrelated to the operation. Another caveat regarding our study is that we used the open door laminoplasty technique, a modification of the one described by Hirabayashi et al. 24 Therefore, our results may not necessarily apply to the French door technique. However, because the surgical exposure for French door and open door laminoplasty techniques is similar, we anticipate similar outcomes with the French door technique. It would be valuable if this study were replicated in centers that perform French door laminoplasty. We also operated on patients who had relatively low baseline NDI scores. It is possible that patients with a higher baseline NDI score may not fare as well as our group. However, a recent study using visual analog scale (VAS) to quantify neck pain following laminoplasty found that even in patients with preoperative neck pain and higher VAS scores, significant improvement in VAS score was noted at latest follow-up. 25 Finally, we relied on the NDI as our outcome score, and it is plausible that our study would have been strengthened by concurrent use of the VAS score to assess neck pain.
In conclusion, in a series of 34 patients undergoing laminoplasty with relatively low baseline NDI scores, significant improvements in NDI pain subscore and NDI total scores at a minimum of 1 year postoperative were noted. In our practice, we routinely perform open door laminoplasty and believe that the postoperative axial pain symptoms can be alleviated with the following strategy: (1) preserve the insertion of the semispinalis cervicis at C2 by performing laminectomy rather than laminoplasty at C3; (2) whenever possible, avoid performing laminoplasty at C7 to preserve the muscular attachments of the rhomboid and trapezius; and (3) perform meticulous multilayered closure of the semispinalis cervicis and fascia so as to avoid dead space and muscle atrophy.
Disclosures
Addisu Mesfin, none
Moon-Soo Park, none
Chaiwat Piyaskulkaew, none
Tapanut Chuntarapas, none
Kwang Sup Song, none
Han Jo Kim, Consultant: Medtronic, K2M, Biomet
K. Daniel Riew, Board membership: AOSpine International; Royalties: Biomet, Medtronic, Osprey; Stock/stock options: Amedica, Benvenue, Expanding Orthopedics, Nexgen Spine, Spinal Kinetics, Spineolgy, Vertiflex, PSD