
Abstract
Study Design
Retrospective study.
Objectives
Lumbar radiculopathy is rarely observed in patients who have achieved bony healing of vertebral fractures in the middle-lower lumbar spine. The objectives of the study were to clarify the clinical features of such radiculopathy and to evaluate the preliminary outcomes of treatment using a modified posterior lumbar interbody fusion (PLIF) procedure.
Methods
Fourteen patients with at least 2-year follow-up were enrolled in this study. The radiologic and clinical features of radiculopathy were retrospectively reviewed. As part of our modified PLIF procedure, a bone block was laid on chipped bone to fill the cavity of the fractured end plate and to flatten the cage–bone interface.
Results
The morphologic features of spinal deformity in our patients typically consisted of the intradiscal vacuum phenomenon, spondylolisthesis, and a retropulsed intervertebral disk with a vertebral rim in the damaged segment. Cranial end plate fracture resulted in radiculopathy of the traversing nerve roots due to lateral recess stenosis. On the other hand, caudal end plate fracture led to unilateral radiculopathy of the exiting nerve root due to foraminal stenosis. The mean recovery rate based on the Japanese Orthopaedic Association score was 65.0%. Solid fusion was achieved in all but one case.
Conclusions
Because of severe deterioration of the anterior column following end plate fracture, the foraminal zone must be decompressed in caudal end plate fractures. The modified PLIF procedure yielded satisfactory clinical outcomes due to anterior reconstruction and full decompression for both foraminal and lateral recess stenoses.
Keywords
Introduction
Vertebral collapse is a common injury in elderly patients. Some reported treatments for fresh collapse and delayed-onset vertebral collapse can cause paraparesis of the thoracolumbar spine. 1 , 2 On the other hand, in the middle-lower lumbar spine, vertebral collapse is less common, and lumbar radiculopathy is rarely observed in patients who have achieved bony healing of vertebral fractures. Thus, the clinical features of such radiculopathy that are essential to making a decision regarding the surgical strategy have been reported in only one publication, 3 and there has been a limited number of reports on their treatment. 4 , 5 , 6 Although the posterior lumbar interbody fusion (PLIF) procedure can facilitate reconstruction of the anterior column and neural decompression, unfavorable congruency between the cage and deformed end plate is a major difficulty. In our institute, we have used modified PLIF to flatten the cage–bone interface against the cavity of the deformed end plate.
The aims of this study were to clarify the clinical features of radiculopathy secondary to healed vertebral collapse of the middle-lower lumbar spine and evaluate the preliminary outcomes of treatment using our modified PLIF procedure.
Materials and Methods
Study Population
From April 2003 until February 2011, 14 patients (5 men, 9 women), with a mean age of 74 years (range, 59 to 86 years), underwent our modified PLIF procedure with instrumentation for radiculopathy following the bony healing of vertebral collapse of the middle-lower lumbar spine. Three patients had a history of minor trauma, involving falling or tripping. The other 11 had occult fractures with unknown causes. In only one patient, the initial treatment for vertebral fracture consisted of bed rest and then ambulation with a soft lumbar corset. Four patients were treated with a soft lumbar corset without bed rest. Nine patients received no initial treatment. The level of the vertebral fracture was L3 in 7 patients, L4 in 4, and L5 in 3. The mean period from radiographic diagnosis of the fracture to surgery was 12 months (range, 10 to 15 months).
Clinical and Radiologic Evaluations
To clarify the clinical features of radiculopathy, medical records were retrospectively reviewed. We preoperatively identified the nerve root suspected from neurologic and radiologic findings as the causative nerve root by selective radiculography and block. In addition, the validity of our diagnosis was postoperatively confirmed by the disappearance of radiculopathy. The morphologic features of vertebral deformity were identified on radiographs, multiplanar reconstructions of computed tomography, and magnetic resonance imaging in all patients.
The duration of surgery, estimated intraoperative blood loss, and surgery-related complications were examined in all patients. Except for 1 patient who required revision surgery, surgical outcomes, as described below, were reviewed in 13 of the 14 patients with at least 2-year follow-up. The mean follow-up period was 32 months (range, 24 to 54). The clinical outcome was assessed using the Japanese Orthopaedic Association (JOA) score (Table 1) and the recovery rate of the JOA score before surgery and at the final follow-up. 7 Sagittal alignment of the fused segment was measured on neutral lateral radiographs with the Cobb technique preoperatively, immediately after surgery, and at the final follow-up. 8 Solid spinal fusion was confirmed by the presence of interbody bone bridging, absence of continuous radiolucent interbody lines, and no motion on lateral flexion-extension radiographs at the final follow-up.
The assessment scale proposed by the Japanese Orthopaedic Association
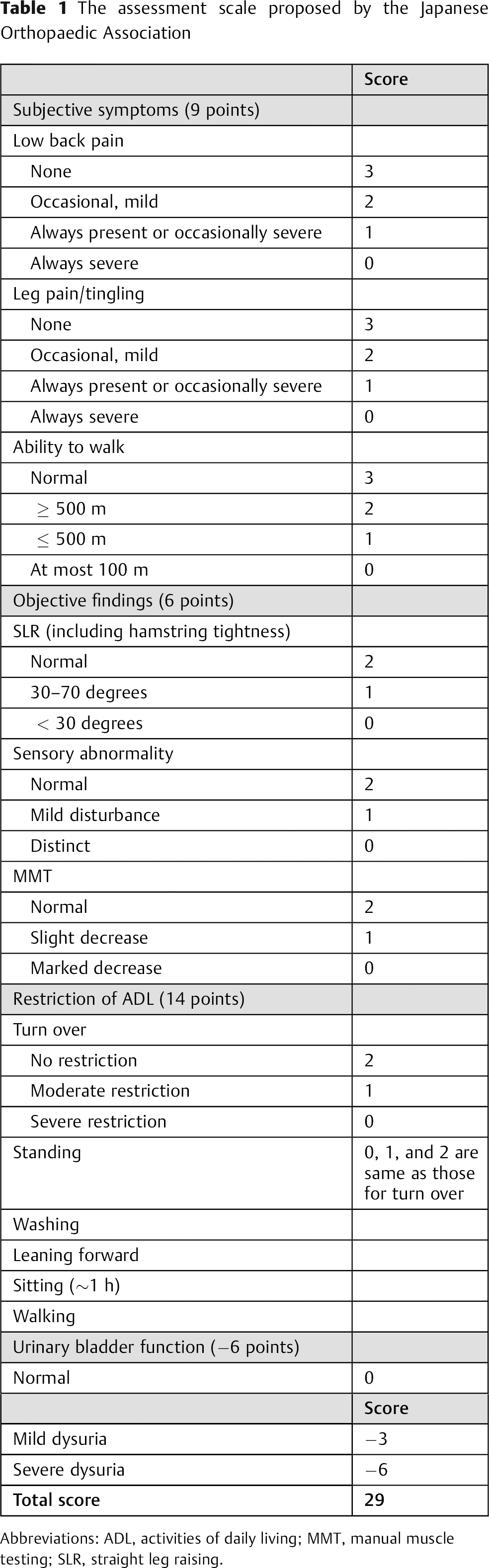
Abbreviations: ADL, activities of daily living; MMT, manual muscle testing; SLR, straight leg raising.
Surgical Technique
PLIF was indicated at the intervertebral disk space adjacent to the fractured end plate. Patients with radiculopathy of the exiting nerve root due to foraminal stenosis underwent total facetectomy on the symptomatic side. Patients with radiculopathy of the traversing nerve roots resulting from lateral recess stenosis underwent medial or total facetectomy, as appropriate. The cartilaginous end plate was carefully removed to avoid damage to the fractured end plate. We used autograft bone in all cases. The Brantigan carbon fiber cage (DePuy, Raynham, Massachusetts, United States) was used, and local bone was obtained from the spinous process, laminae, and facet. An iliac bone graft was required in only one patient. A morselized bone graft was packed into the anterior disk space. As part of our modified PLIF procedure for the poor congruency between the cage and deformed end plate, a bone block was laid on chipped bone to fill the cavity of the fractured end plate and to flatten the cage–bone interface (Fig. 1). Chipped bone was morselized bone from cancellous and cortical bone. The bone block was a sheet of structurally intact cortical bone. Two cages filled with the milled local bone were then inserted into the central disk space. Then, two strut bone blocks were inserted lateral to the cages.
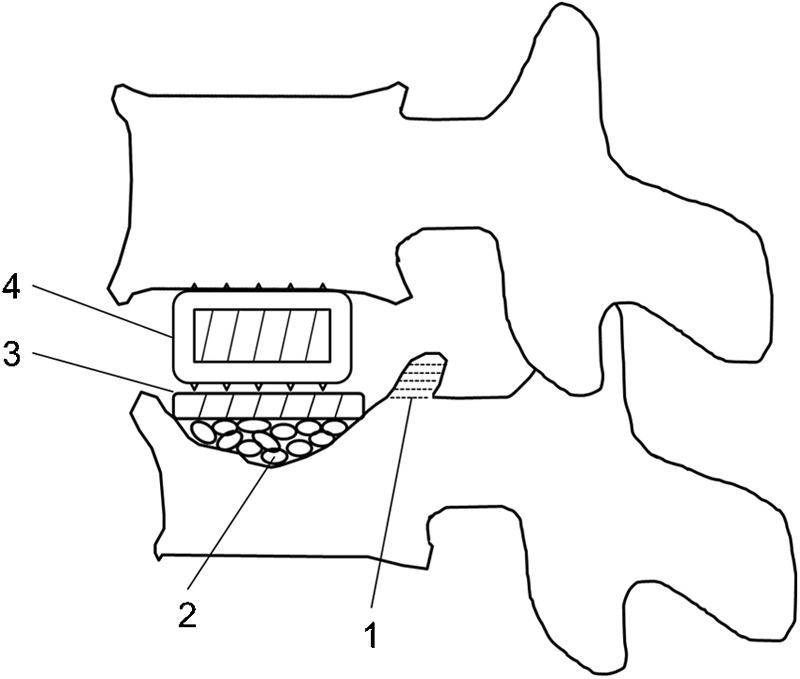
Schema of the modified posterior lumbar interbody fusion procedure. The retropulsed rim (1) and disk were removed, and a bone block (3) was laid on the chipped bone (2) to flatten the cage–bone interface. Two cages (4) were then inserted.
The fused segment was fixed with a pedicle screw system without augmentations, such as sublaminar wiring, calcium phosphate cement, bone cement, or granulated hydroxyapatite. When it was possible to insert pedicle screws into the collapsed vertebrae, single-segment PLIF was performed. When this was impossible due to severe vertebral collapse at the cranial end plate, the surgical options were as follows: (1) laminar hooks were applied to the fractured vertebrae for single-level PLIF or (2) posterolateral fusion or PLIF with pedicle screws was added at one more caudal segment for two-level fusion. No patients had more than two-level fusion. Based on these surgical strategies, single-level PLIF was performed in 10 patients, 1 patient underwent two-level PLIF, and single-level PLIF with supplemental single-level posterolateral fusion was indicated in 3 patients.
Patients were ambulated on postoperative days 2 to 14 (mean, day 3). A soft lumbar orthosis was routinely worn for 3 months postoperatively.
Results
Clinical Features
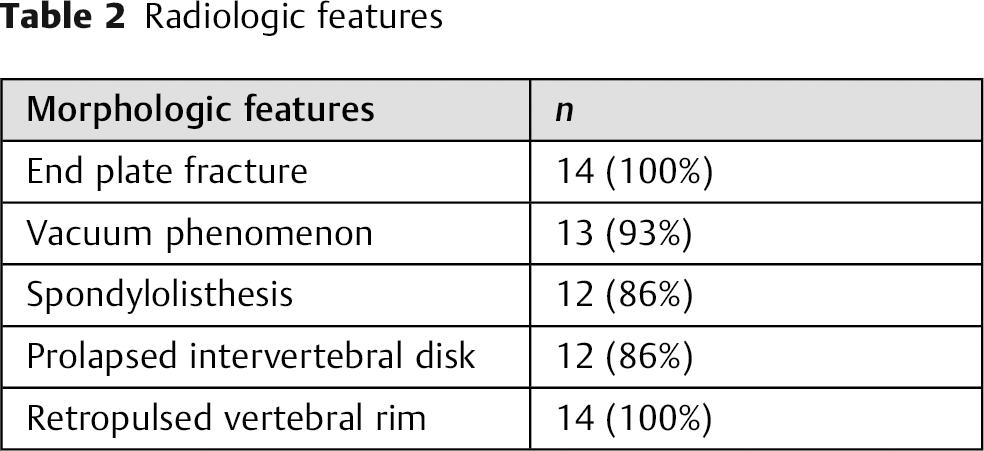
According to the AO Spine classification of thoracic and lumbar injuries, the injury patterns were divided into only two patterns: type A3.1.1 (superior incomplete burst fracture) in 7 patients and type A3.1.3 (inferior incomplete burst fracture) in 7 patients. 9 All patients showed end plate fracture at the cranial and caudal end plates (seven patients each). The vacuum phenomenon in the intervertebral disk adjacent to the deformed end plate was noted in 13 patients, spondylolisthesis at the damaged segment in 12, and a prolapsed intervertebral disk in 12; a retropulsed vertebral rim was identified in all patients (Table 2). Nine of the 14 patients developed radiculopathy ∼1 month after the time of injury. The other 5 patients suffered from radiculopathy with onset 3 to 5 months after the time of injury. In all cases, severe radicular pain continued even after the healing of the fracture was confirmed. In patients with cranial end plate fracture, the cranial vertebra adjacent to the collapsed vertebra slipped, causing bilateral radiculopathy of the traversing nerve roots due to lateral recess stenosis. Lateral recess stenosis occurred from a combination of a retropulsed vertebral rim and thickened ligamentum flavum (Fig. 2). In those with a caudal end plate fracture, the collapsed vertebra slipped, causing unilateral radiculopathy of the exiting nerve root due to foraminal stenosis. Foraminal stenosis occurred from the vertebral rim and/or disk protruding toward the foraminal zone (Fig. 3). The patients’ clinical features are summarized in Table 3.
Radiologic features
Patients’ clinical features
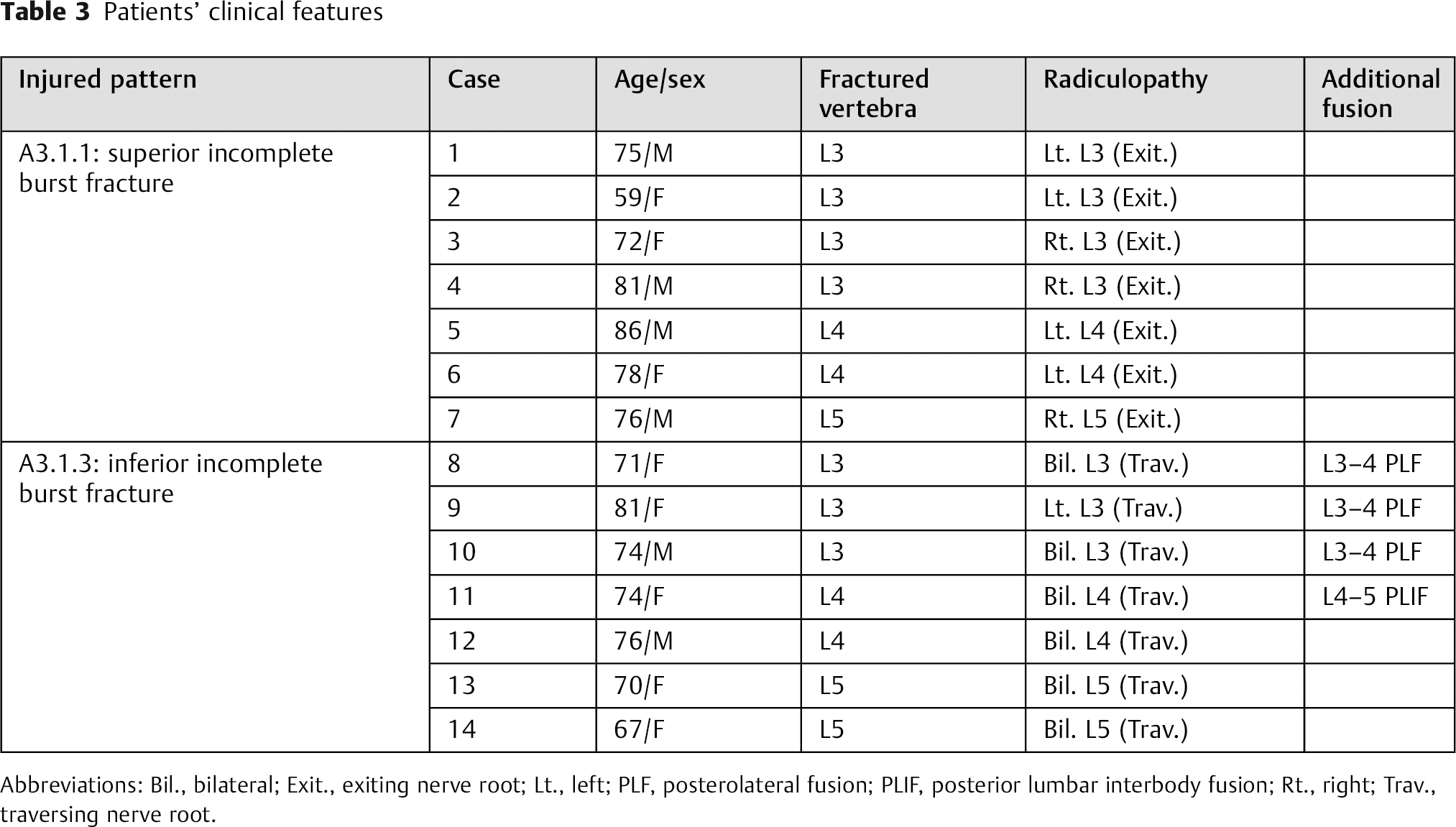
Abbreviations: Bil., bilateral; Exit., exiting nerve root; Lt., left; PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion; Rt., right; Trav., traversing nerve root.
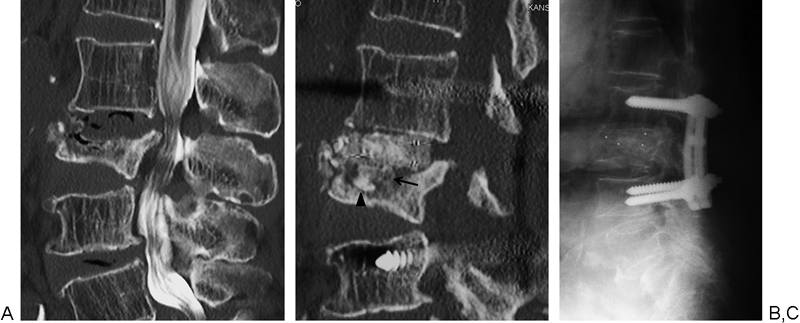
Case 1 with a cranial end plate fracture of L3. (A) Preoperative sagittal reconstruction using computed tomography (CT) myelography shows a prolapsed intervertebral disk, vacuum phenomenon, and retropulsed vertebral rim at L2–3. (B) Postoperative sagittal reconstruction using CT shows that the bone block (arrow) is laid on chipped bone (arrowhead) used to fill the cavity of the fractured end plate to flatten the cage–bone interface. (C) At the 2-year follow-up, a lateral radiograph shows solid fusion with a more pronounced lordotic alignment at the posterior lumbar interbody fusion site.

Case 9 with a caudal end plate fracture of L3. (A) Preoperative myelography shows that the collapsed vertebra (L3) has slipped. (B) Preoperative coronal reconstruction using computed tomography (CT) shows vertebral body collapse mainly in the left L3–4 foraminal zone (arrowheads). (C) Preoperative sagittal reconstruction using CT shows foraminal stenosis occurred from the vertebral rim and disk (arrows). (D) Postoperative sagittal reconstruction using CT shows the bone block (arrow) laid on chipped bone (arrowhead) used to fill the cavity of the fractured end plate to flatten the cage–bone interface. (E) At the 2-year follow-up, a lateral radiograph shows solid fusion with a more pronounced lordotic alignment at the posterior lumbar interbody fusion site.
Surgical Outcome
The mean duration of surgery was 190 minutes (range, 107 to 405 minutes), and the mean estimated intraoperative blood loss was 340 mL (range, 50 to 740 mL).
The mean JOA score was 9.0 points (range, 4 to 16 points) before surgery, showing improvement to 22.1 points (range, 17 to 29 points) at the final follow-up. The mean recovery rate of the JOA score was 65.0% (range, 30.8 to 100%).
The mean local kyphosis at the segment treated by PLIF improved from 5.3 degrees before to −1.1 degrees after surgery, but it had deteriorated to 0.2 degrees at the final follow-up (Table 4). Solid fusion was obtained in all but one patient (case 10), who showed severe kyphosis of 25 degrees at the injured segment before surgery and refused to wear an orthosis after surgery. Due to progressive kyphosis following pedicle screw loosening 6 weeks after the initial operation, revision surgery of the anterior reconstruction using fibula struts and posterior long instrumentation was needed. Symptomatic adjacent segment degeneration was not observed, but vertebral collapse at the cranial end of PLIF segments occurred in one patient 3 years postoperatively.
Kyphosis at PLIF segment (degrees)
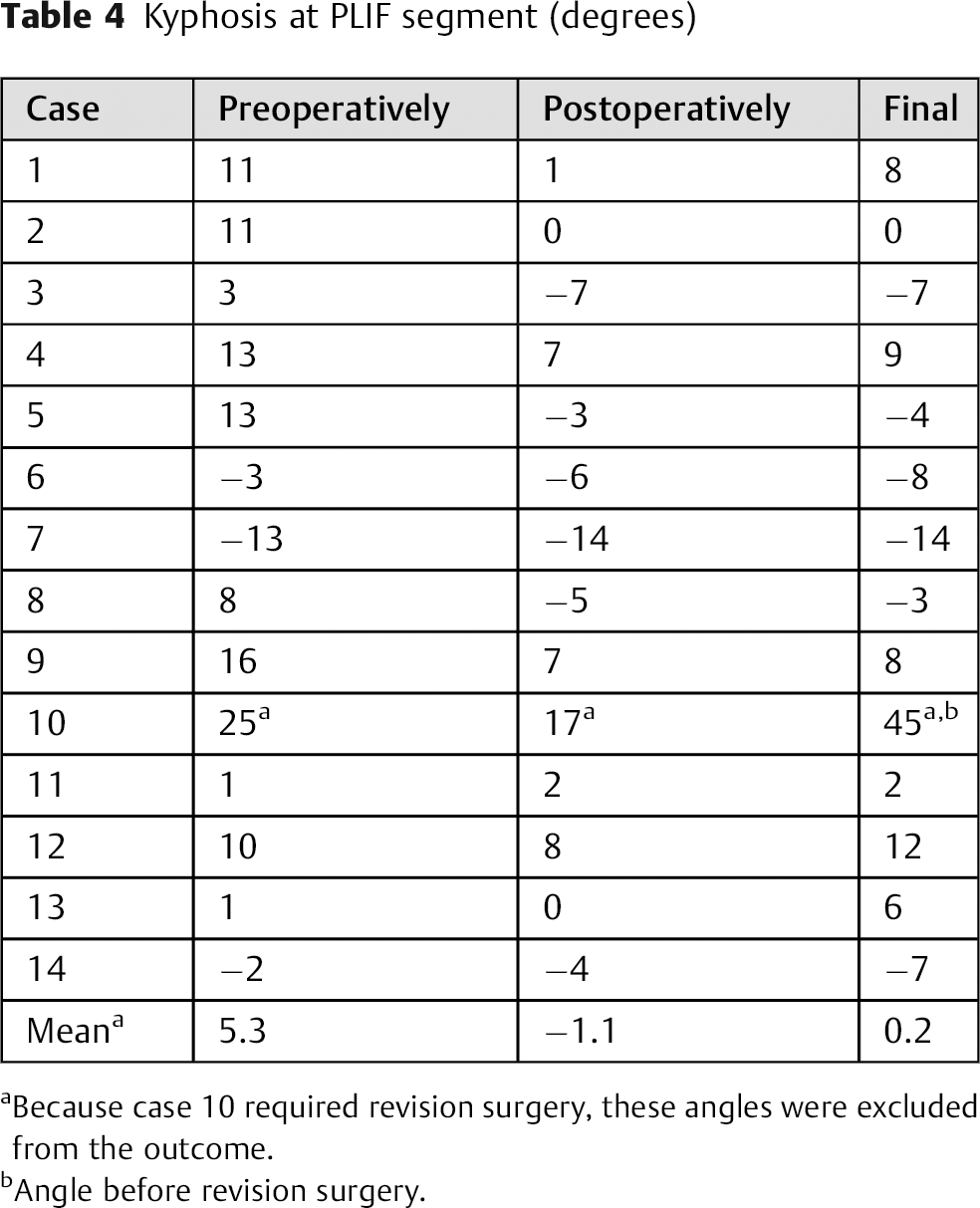
Because case 10 required revision surgery, these angles were excluded from the outcome.
Angle before revision surgery.
Discussion
In the present study, almost all patients showed the vacuum phenomenon and spondylolisthesis at the injured segments, which means the progression of intervertebral disk degeneration, 10 Central end plates play a more important role in the transportation of metabolites into and out of the disk than peripheral end plates. 11 , 12 , 13 , 14 Unlike the thoracolumbar region (T10–L2), the axial compression forces posterior to the spine in L3 and below tend to cause concave-type collapse with central end plate fracture. 15 Therefore, disk degeneration of the middle-lower lumbar spine may show a tendency to progress and even accelerate after fracture, as seen in most of the patients in the present study who had received no initial treatment for vertebral collapse. Thus, the surgical strategy must incorporate reconstruction of the anterior column.
Interestingly, the patterns of neural compression vary between caudal and cranial end plate fractures. In particular, it must be kept in mind while operating that the foraminal zone should be decompressed in caudal end plate fractures. Sasaki et al also reported that radiculopathy following vertebral collapse frequently involves lumbar foraminal stenosis. 3 Although end plates have been reported to be thinner centrally and cranially, only the most posterior region of the caudal end plate in a parasagittal plane through the pedicle has been reported to be thinner than the cranial end plate and to decrease in thickness near the central region. 11 Therefore, the caudal vertebral rims could protrude not posteriorly, but posterolaterally, and induce foraminal stenosis.
A few reports have discussed the treatment of lumbar radiculopathy following vertebral collapse. A modified eggshell procedure with posterior decompression and posterolateral fusion, vertebroplasty, or kyphoplasty with interspinous process spacers and only vertebroplasty were previously reported. 16 , 17 , 18 However, the mechanism of neural compression by the movement of fractured bony fragments in these three reports was distinct from that by stable bony protrusion with segmental instability in this series.
With the same pathogenesis as the present study, Sasaki et al reported unfavorable results of posterior decompression without spinal fixation: 3 of 6 patients treated with posterior decompression developed radiculopathy again caused by foraminal stenosis at the same level, and 2 of them presented progressive preexisting spondylolisthesis. The two patients whose condition deteriorated were free from pain until the last follow-up after second PLIF operations. The scores of patients treated with posterior decompression alone gradually worsened in the late postoperative periods, whereas the scores of the patients treated with PLIF were maintained during the postoperative follow-up period. The authors suggested that late deterioration of the scores in the patients treated with posterior decompression alone was attributed to spinal instability caused by removal of posterior spinal elements. 3 Given the clinical features of spinal condition identified in the present study, PLIF is reasonable. PLIF with total facetectomy can fully decompress the foraminal zone and obtain rigid spinal stability.
Nishi et al reported favorable neurologic and functional outcomes in four patients who underwent instrumented posterolateral fusion including two to four levels. 6 In that study, the mean correction loss of sagittal alignment of the fused segments reached 13.0 degrees at the final follow-up. Despite long fusion, their treatment without anterior reconstruction cannot maintain lordotic alignment after surgery. On the other hand, in the present study, the loss of correction could be minimized using our modified PLIF procedure with at most two-level fusion. For solid fusion with lordotic alignment, the contact area between the deformed end plate and graft should be large and perpendicular to the axial force. To flatten the contact area, resection of the vertebral body containing the deformed end plate requires a large amount of graft bone. Moreover, resection of the bony end plate can lead to progressive subsidence of grafts. We were able to achieve optimal congruency with a bone block laid on chipped bone to fill the cavity of the fractured end plate. We could obtain a sufficient amount of bone for grafting from local bone in all except one patient. Because case 10 had severe kyphosis before surgery and needed revision surgery due to vertebral destruction and progressive kyphosis following pedicle screw loosening, severe osteoporosis and/or kyphosis may require anterior reconstruction and posterior long instrumentation.
We present the algorithm for surgical treatment from results obtained in the present study (Fig. 4). The present study has several limitations, including the small number of patients and absence of evaluation of other treatments. However, these preliminary results suggest that our modified PLIF procedure can provide satisfactory clinical outcomes for radiculopathy following healed vertebral collapse of the middle-lower lumbar spine.
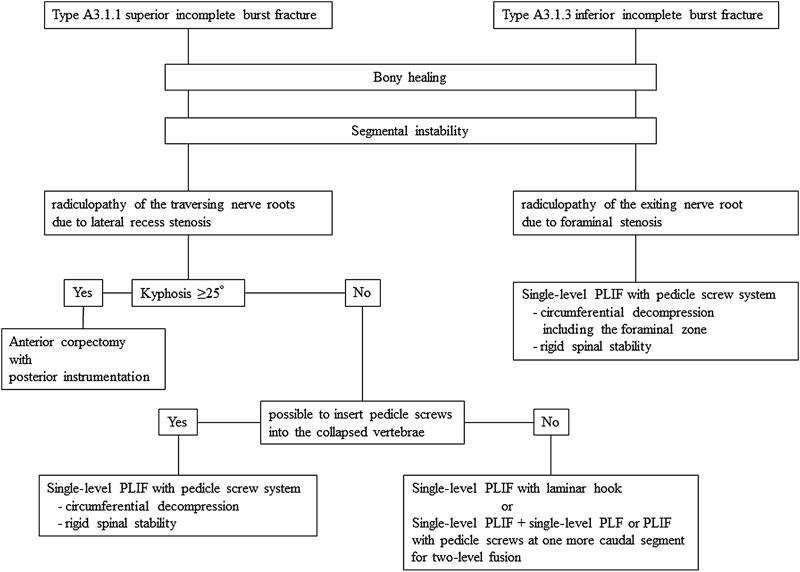
Surgical treatment algorithm for radiculopathy following healed vertebral collapse of the middle-lower lumbar spine. Abbreviations: PLF, posterolateral fusion; PLIF, posterior lumbar interbody fusion.
Conclusion
In severe deterioration of the anterior column following end plate fracture, the foraminal zone must be decompressed in caudal end plate fracture. The modified PLIF procedure facilitated satisfactory clinical outcomes due to anterior reconstruction with less correction loss and full decompression for both foraminal and lateral recess stenoses.
Disclosures
Tomoya Yamashita, none
Hironobu Sakaura, none
Toshitada Miwa, none
Tetsuo Ohwada, none