
Abstract
Study Design
Case report.
Objective
The recommended treatment of cervical subluxation is currently closed or open reduction. These treatments are better accomplished in the acute setting, when muscular and ligamentous laxity allows the required maneuvers to realign the dislocated segments. However, subsets of patients are still being treated subacutely. The majority of the literature addressing subacute subluxations reports treatment through “front and back” approaches, many of them performed in two, three, or even four stages. Other authors recommend days or weeks of traction to reduce the subluxation, followed by anterior or posterior approaches. Herein, we present a one-stage open posterior surgical treatment of a 2-month standing C5–C6 subluxation with “jumped facets,” describing a useful technique to reduce these challenging cases without the need of traction or multistage procedures.
Methods
After opening and exposing the posterior elements, we performed a wide C5–6 bilateral foraminotomy; we then put lateral mass screws and rods from C4 to C6. Resembling the technique used in the reduction of high-grade lumbar spondylolisthesis, we used a rod reducer to bring back the C5 screw head toward the rod, thus realigning the lateral mass screw heads and reducing the subluxation.
Results
No changes were observed in the motor evoked or somatosensory potentials during this maneuver. Following an uneventful procedure, the patient was transferred to the postanesthetic care unit and discharged 3 days later.
Conclusions
This open single-stage posterior approach dramatically reduces operating time. This technique could be added into the decision-making armamentarium for cases without disk herniation.
Case Report
History
A 64-year-old woman with no previous medical history sustained a motor vehicle accident (MVA) on January 23, 2012 (she crashed into a truck from behind). When examined in the field, the patient noted numbness and weakness in her arms and numbness in her lower limbs. She was put in a Philadelphia collar and transferred to the nearest hospital, where head and spine images were obtained. The cervical spine X-rays and computed tomography scan showed a frank C5–C6 dislocation with jumped facets (Figs. 1A, B, and C). Magnetic resonance imaging (MRI) showed a spared posterior longitudinal ligament with ruptured posterior elements (interspinous and supraspinous ligaments; Fig. 1D). Within 24 hours of admission, her neurologic symptoms resolved. Based on her imaging findings, she was advised to undergo surgery within 48 hours. The patient refused surgical treatment and was discharged home 4 days after the accident on the Philadelphia collar. During the weeks following the MVA, she consulted other neurosurgeons, who also recommended surgery. She was referred to our department 38 days after the accident. At that time, she was neurologically intact (Frankel grade E); however, she experienced neck pain, which was moderately controlled with nonsteroidal anti-inflammatory drugs. After carefully explaining her condition to her, she finally decided to proceed with surgery a few weeks later and was operated on March 22 (59 days after the MVA). Considering the facet remodeling found in these kind of cases 1 and the fact that failure of closed reduction is more common with facet dislocation injuries, 2 we decided not to attempt traction before the procedure.
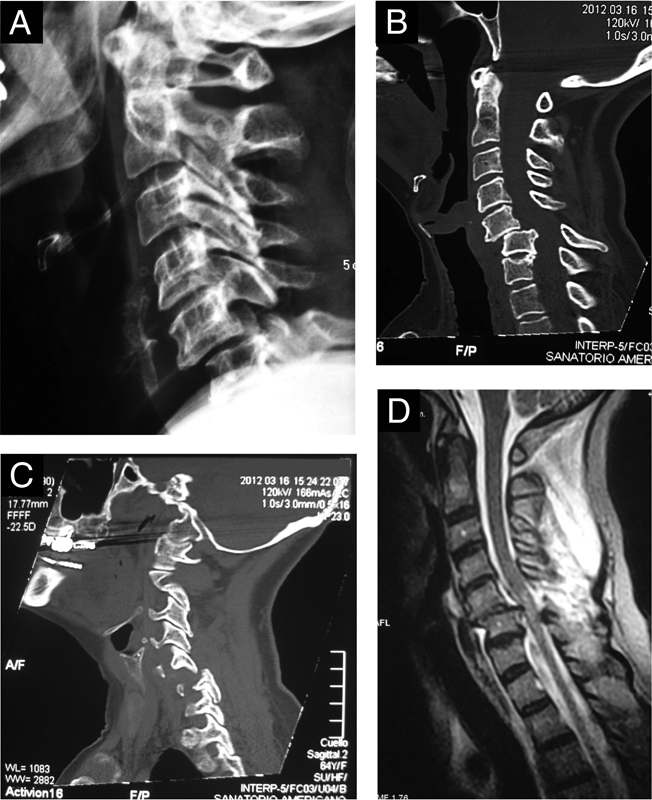
(A) Initial plain X-ray showing a C5–6 subluxation with bilateral locked facets. (B) Preoperative sagittal computed tomography (CT) scan with bone windows; degeneration at the C4–5 level is clearly seen. (C) Parasagittal CT scan with bone windows; although the C5–6 facet joint appears to be separated, they looked fused intraoperatively. (D) Preoperative sagittal T2-weighted magnetic resonance imaging showing an intact posterior longitudinal ligament without disk extrusion.
Operation
Because the posterior longitudinal ligament was intact and the posterior ligaments were disrupted (Fig. 1D), we performed a posterior approach under neurophysiologic monitoring of motor and somatosensory evoked potentials (MEPs and SSEPs). The patient was placed in a Mayfield head holder with her neck slightly extended. After opening and exposing the posterior elements, the locked C5–C6 facets appeared ossified, and no joint space could be identified (Fig. 3A). Using a high-speed drill and with the aid of the C-arm, we performed a wide bilateral foraminotomy to refracture the partially ossified facets and release both C6 roots. After this, we placed four lateral mass screws (two on C5 and two on C6; Vertex system; Medtronic Sofamor-Danek, Memphis, Tennessee, United States). Initially, we thought the C5 body could be easily brought back with a towel clamp, as described by Lim et al.3 However, the C5 vertebral body stayed in that position and could not be reduced by this maneuver. Because the C4–5 space was already degenerated (Figs. 1B and D), we decided to extend the instrumentation to C4 (Fig. 3B), and we secured a rod from C4 to C6, spanning the C5 lateral mass screw. Resembling the technique utilized in the reduction of high-grade lumbar spondylolisthesis with “reduction screws,”4 we used a rod reducer to bring the C5 screw head back toward the rod (Fig. 3C), thus realigning the lateral mass screw heads and reducing the subluxation (Fig. 3D; Fig. 2B). No changes were observed in the MEPs or SSEPs during this maneuver. After both rods were tightened with six lock head screws, bone was harvested from the posterosuperior iliac crest to achieve posterolateral fusion.
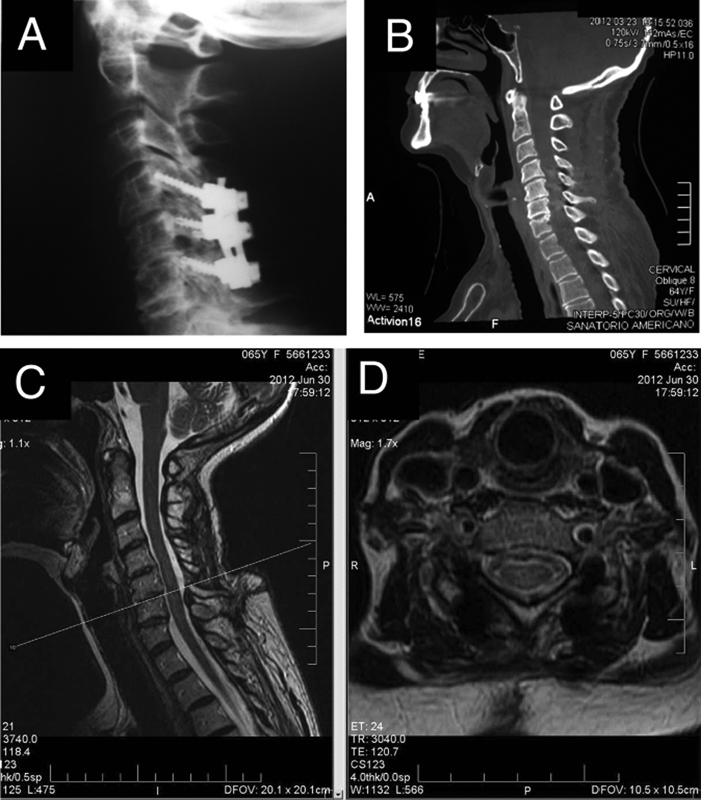
(A) A 9-month postoperative plain X-ray. (B) Postoperative sagittal computed tomography scan with bone windows. (C, D) Postoperative T2-weighted magnetic resonance imaging taken 3 months after the operation, showing complete reduction.
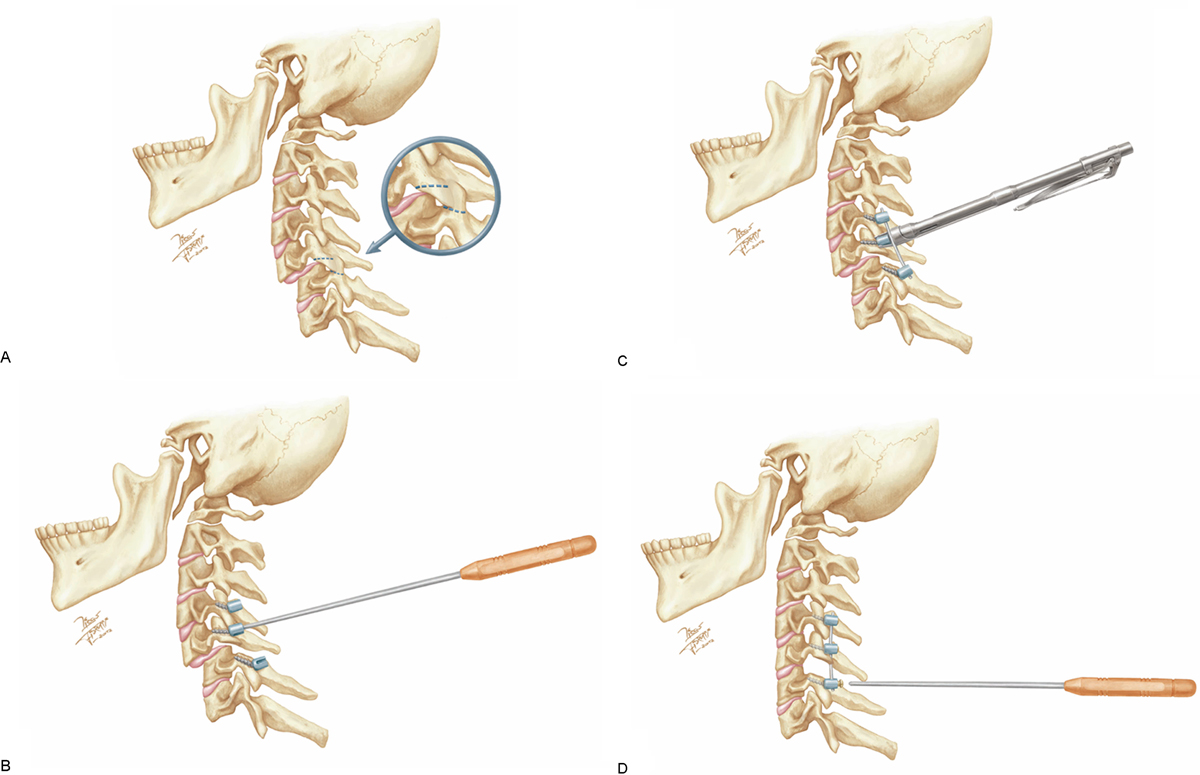
(A) Artist's drawing depicting the C5–6 bilateral facet subluxation. Note the almost fused facet joint, which is usually found in old cases. Dotted lines mark the limits of the facetectomy performed. (B) Lateral mass screw placement at C4, C5, and C6. (C) Reduction maneuver utilized in this case to “bring back” the C5 lateral mass's screw head toward the rod. The rod reducer (Vertex system; Medtronic Sofamor-Danek, Memphis, Tennessee, United States) allowed a gentle and controlled reduction, one side at a time. (D) Final construct showing complete C5–6 reduction.
Postoperative Course
Following an uneventful 3-hour procedure, the patient was transferred to the postanesthetic care unit and discharged 3 days later. On her immediate postoperative exam, a mild (4/5) right C6 paresis was noted, which resolved completely within 48 hours. On postoperative follow-up, she remained neurologically intact and pain free (Figs. 2A, C, and D). She has been followed for more than 20 months now.
Discussion
About 200,000 people currently live with spinal cord injuries in the United States, with 15 to 40 new cases per million people estimated to occur annually. 5 , 6 More than 50% of these involve the cervical spine, and half of these present with unilateral or bilateral subluxations. The vast majority of these cases are treated within a week, either by traction, open reduction, or both.
When the interval between the accident and diagnosis is longer than 3 weeks, the injury is considered old.7,8 Some authors consider injuries old when the interval is longer than 8 weeks. 1 There are few reports on the management of old dislocations of the subaxial cervical spine in the literature, 1 , 7 , 9 , 10 , 11 but these injuries still occur. They have been called “old,” 10 “neglected,” 7 or “delayed managed” 1 cervical traumatic subluxations and usually occur in older populations. 1 , 10 This could explain the relatively mild neurologic status of these patients (Frankel C or more) because, in this age group, the facet dislocation may be produced by less severe forces, which are less likely to damage the cord. 12
In one of the biggest series published to date, Hassan reported the surgical treatment of 12 patients with an old dislocation of the lower cervical spine. 10 The time from injury to presentation averaged 3.5 (range 1.5 to 12) months, and the majority of the dislocations were between C4 and C5. The author's treatment protocol started with 1 week of skull traction followed by anterior fusion with plate fixation. If reduction was not achieved, the traction was continued for another week and then followed by anterior diskectomy and fusion with plate fixation. In cases in which reduction by traction did not succeed, a posterior partial facetectomy was performed, followed by a posterior fusion with plate fixation. The average follow-up was 34 (range 12 to 54) months, and all patients developed bone fusion and showed neurologic improvement.
Jain et al described the open reduction of four patients in whom the mean delay between injury and presentation was 4 months (range 1 to 5). 7 The mean age of the patients was 48.2 years old (range 27 to 60), and three of them had a myelopathy. Each patient experienced neck pain and restricted movement of the cervical spine. They performed a two-stage procedure under the same anesthetic. On the first stage, they performed a posterior soft tissue release and partial facetectomy to allow partial reduction of the dislocation, supplemented by interspinous wiring and corticocancellous graft. During the second, anterior stage, they did a diskectomy, tricortical bone grafting, and anterior cervical plating. All the patients achieved a nearly anatomical reduction with a mean follow-up of 2.6 years (range 1 to 4). The myelopathy settled completely in three patients, and there was no graft dislodgement or graft-related problems. In the authors’ experience, the posteroanterior procedure for neglected traumatic bilateral dislocation of the subaxial cervical spine is a good method of achieving sagittal alignment.
Bartels and Donk reported the surgical treatment of three cases. 1 They treated the first two cases through a three-stage approach (anterior-posterior-anterior). Because these cases failed and a fourth stage had to be added to correct misalignment, the third case was done through a posterior-anterior-posterior approach. As in our case, the authors stated that facet joints were covered with fibrous tissue and the joint space was not seen. Based on their experience, they suggest that in cases of nonacute bilateral cervical facet dislocations, the operating sequence should be posterior-anterior-posterior. It should be noted that the cohort's mean age was 71, suggesting again that patients who present subacutely tend to be older. For this reason, an open single-stage posterior approach under neurophysiologic monitoring dramatically reduces operating time, which is important to reduce morbidity in these cases. Note that this technique can be added to the decision-making armamentarium only for cases without disk herniation. When signs of frank disk herniation are found on the preoperative MRI, anterior diskectomy is mandatory to avoid neurologic deterioration during reduction, as recommended by Eismont et al. 13 Although this technique could be easily criticized due to the fact that a rostral level needs to be included in the fusion, we believe this does not add morbidity and has been done for years in lumbar spondylolisthesis.4 Moreover, because this entity is more frequent in older patients, the chances of finding an already degenerated level rostral to the subluxation are high.
Whereas a 2-month subluxation is regarded as old by most authors, it is uncertain whether this technique would work on most chronic dislocations. Perhaps dislocations older than 3 months could not be easily reduced through this technique, as a result of ossification of the uncovertebral joints. Finally, it is critical to note that this technique is somewhat different from its lumbar counterpart. Given the fact that lumbar pedicle screws achieve a much better purchase than cervical lateral mass screws, there is a potential risk for screw pullout during the reduction technique. Hence, we recommend bicortical lateral mass screws to avoid this possible complication.
Disclosures
The authors report no financial relationships or conflicts of interest regarding the content herein.
Footnotes
Acknowledgments
The author would like to thank Mr. Kelmen Muro for helping us preparing the manuscript, Mr. Fernando Zacarias, who was very helpful in composing the pictures, and Mr. Diego Fiorucci, the artist behind the beautiful drawings.