
Abstract
Study Design:
Prospective case series.
Objective:
To evaluate the efficacy of anterior-only approach, for treatment of type C F4 (AO classification) traumatic subaxial cervical spine injuries.
Methods:
Patients with type C F4 traumatic cervical injuries presenting to a tertiary center between June 2017 and July 2018 were included. Outcome measures included self-reported measures (Neck Disability Index, visual analogue scale, and return to work), radiological measures (local segmental angle, Ishihara curvature index, cervical lordosis angle, and step-off distance), fusion state, and neurological state according to American Spinal Injury Association (ASIA) Impairment Scale (AIS).
Results:
Twenty-one cases were operated by anterior approach with mean age 39.1 ± 13.8 years. The most common injury was at C4-5 (47.6%). Six out of 7 cases (85.7%) with preoperative neurological impairment showed late follow-up improvement by one or more grade in AIS. Complete anatomical reduction and imaging measures did not correlate significantly to the self-reported outcome measures. Median value of local segmental angle improved from −16° (−11° to −20) preoperatively to 0° (−7°) to 8°) at late follow-up. The cervical lordotic angle and Ishihara curvature index improved from 35° (29° to 43°) and 6.92 (−2.7 to 28.9) preoperatively, to 44° (33° to 51°) and 18.7 (−3.5 to 26.9) at the late follow-up, respectively. Step-off distance decreased postoperatively, however; complete reduction could not be achieved.
Conclusion:
Surgical treatment of lower cervical traumatic instability by anterior decompression and fusion is efficient regarding fusion state and patients’ satisfaction. The anterior approach can be recommended in cases with neurological impairment and in patients with medical comorbidities or when a short operative time—compared with combined approach—is preferred.
Keywords
Introduction
In 2013, the most common cause of spinal cord injury worldwide was cervical spine injury accounting for 43.9% to 61.5% of all cases. 1
Most patients with a cervical spine injury, were in their prime age and leading an active lifestyle prior to injury. With any traumatic spine injury, it is critical to assess the spinal stability. In case of subaxial cervical spine, this is commonly done using the 3-column theory. If only 1 column is disrupted, the risk of spinal cord injury is low because the other 2 columns can maintain the structural integrity of the spine. If 2 columns are injured, the cervical spine can move as 2 independent units with the potential to cause severe cord compromise. 2
Management of cervical spine fractures varies from external fixation, in the form of orthosis or halo fixation to surgical decompression and internal fixations based on the type of fracture, instability, or presence of cord compression. 3 The main objectives of surgical management of traumatic injuries to cervical spine are decompression of nervous structures and stabilization of the injured vertebral segment. This allows an early mobilization and recovery of the patient, treating associated injuries, boosts rehabilitation, and facilitates returning to their professional activities. 4
The options of surgical approach for unilateral or bilateral facet injuries include a stand-alone anterior or posterior approach, a combination of both and a staged anterior/posterior/anterior approach. However, there is substantial controversy regarding the most appropriate surgical management, 5 and literature suggests that it depends on approach preferred by the surgeon.
The aim of this study was to evaluate the early results of standalone anterior management of type C F4 subaxial cervical spine injuries. Type C is defined as translational injury in any axis, which includes injuries with displacement or translation of one vertebral body relative to another, in any direction. Injuries where the anterior and posterior vertebral elements are distracted, is classified as translational injuries. F4 injuries include injuries at the tip of the inferior articular process of the cephalad vertebrae rests on the superior tip of the superior articular process of the caudal vertebrae, or an injury resulting in the inferior facet of the cephalad vertebrae translating over the superior articular surface of the caudal vertebrae and remaining ventral to the superior facet of the caudal vertebral body. 6
Materials and Methods
This is a case series study conducted on patients with traumatic subaxial cervical spine instability at the trauma unit of a tertiary center from June 2017 to July 2019. This study was approved by the institutional review board of the university hospitals where it was conducted.
Inclusion Criteria
Acute traumatic cases of adult patients with subaxial cervical spine injury, presented to the Trauma Unit of a tertiary center with type C F4 cervical spine injury according to AO classification.
Exclusion Criteria
Patients with indications of cervical corpectomy and decompensated spinal canal stenosis and central cord syndrome without any evident instability were excluded from our study.
Preoperative Data
All the patients, who were presented with neurological impairments within 24 hours of trauma incidence received methylprednisolone. In the indicated cases, skull tongs were applied except in those patients whose neurological status could not be determined (such as sedated or intubated patients) and patients with concomitant upper cervical injury and MRI was not available, and patients with skull or brain injury. The following data was recorded: (1) detailed history (sex, age, mechanism of injury—whether it is low or high energy trauma, any comorbidities and occupation); (2) patients were classified based on AO subaxial cervical spine classification; (3) patients were assessed neurologically by the American Spinal Injury Association (ASIA) impairment scale (AIS); and (4) radiological examination.
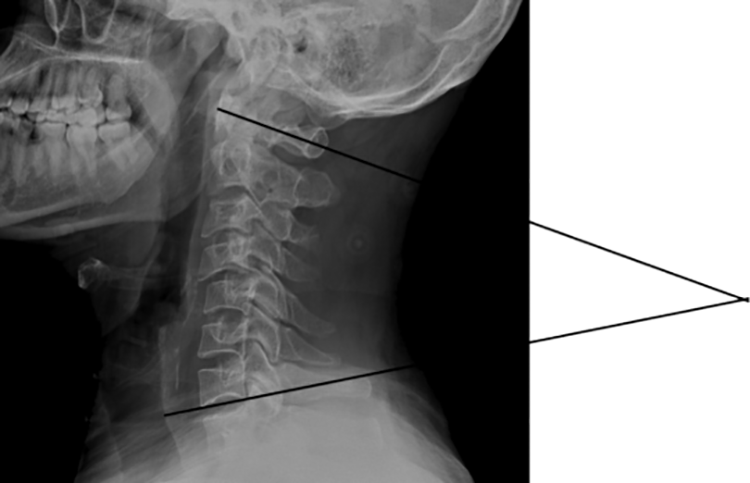
Following parameters were measured by X-ray on cervical spine (anteroposterior and lateral): (1) Local segmental angle formed between 2 lines; one extended from the upper end plate of the proximal vertebra to the injured facets and the other from the lower end plate of the distal vertebra to the injured facets (negative value was put for kyphotic status while positive one for lordotic status). (2) Ishihara curvature index: It is the ratio of the summation of 4 lines drawn from a point at the middle of posterior borders of C3, C4, C5, and C6 perpendicular to a straight line drawn from inferior-posterior borders of C2 to C7, over the length of the line from C2 to C7. (3) Cervical lordosis angle: It is the angle between a line drawn extending from the anterior tubercle of C1 to the posterior margin of the spinous process of the same vertebra, and other line drawn parallel to the inferior endplate of C7. (4) Step-off distance: It is the distance between the 2 lines tangential to the posterior vertebral body wall of the cephalic and caudal vertebrae, measured at the posteroinferior corner of the superior vertebra.
Computed tomography (CT) scan on the cervical spine was performed for evaluation of the bony structures, the extent of encroachment on the spinal canal by vertebral displacement or retro-pulsed bone fragments and the stability of facet joints.
Magnetic resonance imaging (MRI) was performed to evaluate spinal cord signal, canal compression, and disc status.
Operative Data
The intraoperative data, including operative time, blood loss, and intraoperative adverse events was recorded. Cases were operated by surgeons with variable levels of experience, including senior surgeons (more than 10-year experience) and junior ones (less than 10-year experience).
Reduction was achieved in a stepwise approach; first manipulation under fluoroscopy (achieved reduction in 11 patients), failing which open reduction using convergently positioned Casper screws was used to create local kyphosis at the dislocated segment (achieved reduction in 8 patients). In cases where, both these approaches failed a small Cobb periosteal elevator was inserted in the empty disc space to the posterior corner of the inferior vertebra, leveraging the upper vertebra (achieved reduction in 1 case).
Smith-Robinson approach 7 using either a transverse skin incision or a longitudinal one on the right side of neck was performed. A polyether ether ketone (PEEK) cage with bone graft (from the removed bone of the osteophytic endplates) and/or bone substitutes (10 patients local graft, 6 patients local graft + calcium hydroxyapatite, 5 patients calcium hydroxyapatite) were inserted following the discectomy. A locked plate was fixed to the proximal and distal vertebra to stabilize the injured segment. Care was given to use bicortical screws.
Postoperative Immobilization
External support was given with a rigid cervical collar for 3 weeks, followed by a soft one for another 3 weeks, according to our institutional recommendations.
Research Outcome Measures
Self-reported measures included Neck Disability Index (NDI), visual analogue scale (VAS), and return to work. Physiological measures:
Different radiographic measures were documented such as local segmental angle (Figure 1), Ishihara curvature index, cervical lordosis angle (Figure 2), and step-off distance (Figure 3).

Local segmental angle.
Cervical lordosis angle.
Step-off distance.
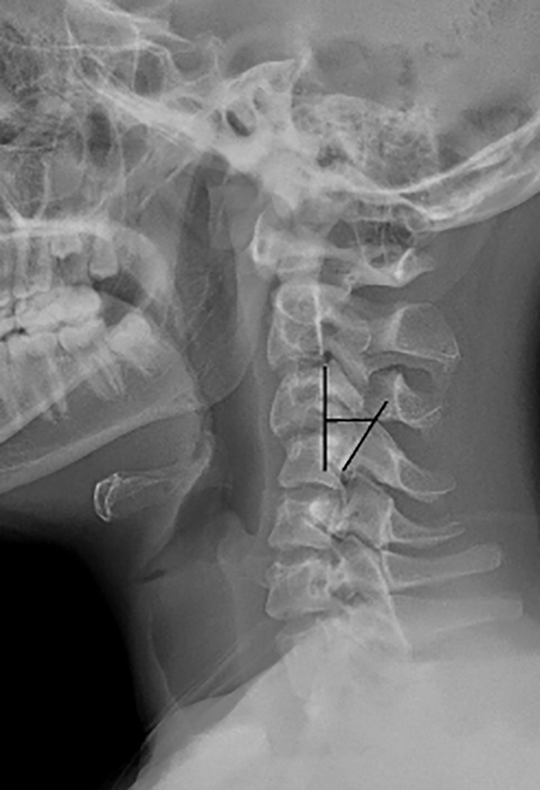
Fusion state was assessed by presence of crossing bone in anteroposterior and lateral X-ray films, mobility on dynamic films, cervical CT scan and measurement of interspinous movement (ISM). ISM is the difference (in millimeters) in the interspinous process distance between the flexion and extension cervical radiographs, used to measure interspinous motion, at each fused cervical level. The most identifiable landmark around the tip of the spinous process, at each level was employed for both the flexion and extension views, on the same monitor simultaneously (Figure 4).
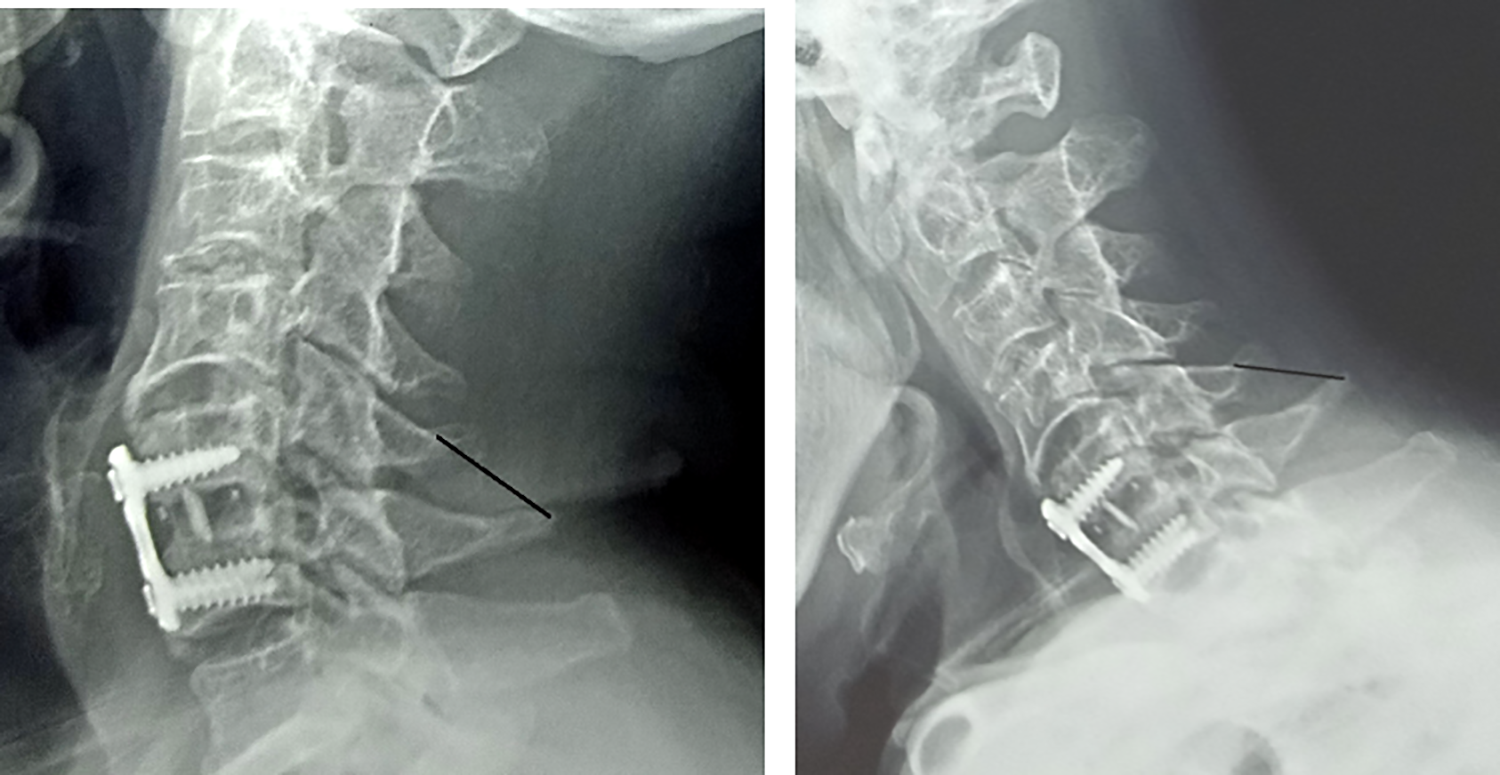
Measurement of interspinous movement.
Follow-up
Three follow-up visits were scheduled as following: after 6 weeks (early postoperative), for neurological examination and plain X-ray, after 6 months, for clinical and neurological evaluation, and after 12 months (late postoperative: for neurological examination and plain X-ray, dynamic films (flexion and extension views), cervical CT scan, NDI, and VAS.
All patients were adequately counseled about their injuries, management options available (including 360-degree fusion), and possible complications. A special consent form to participate in this study was signed either by patient himself or a first-degree relative in presence of a witness, in cases where patient was unable to sign. The research was approved by an independent institutional ethical committee.
SPSS version 20 was used for statistical analysis, including descriptive statistics and tests of significance (T test and chi-square).
Results
Patients’ Demographics
Twenty-one patients were included in this study; of whom 19 were males (90.5%). Their ages ranged from 17 to 60 years (mean 39.1 ± 13.8 years). Manual labor was the most common occupation among these patients.
Mechanism of Trauma
The most common cause of trauma was road traffic accidents (57% motor car accidents and 14% motor bike accidents).
Level of Injury
Twenty patients had single-level injury, and 1 patient had double-level injury. The most common injury level was at C4-5 (10 patients, 47.6%). Six patients had associated disc herniation where the injury level was C3-4 in 1 case, C4-5 in 2 cases, C5-6 in 3 cases. One case had injury at C4-5 associated with fracture C6 (A2 according to AO classification), for which a longer plate fixing C4-7 was done. In another case, the injury level was at C4-5, and associated with spinal canal stenosis at C5-6, for which double level anterior cervical discectomy and fusion was done.
Self-Reported Measures
The mean value of the subjective evaluation of NDI at late follow-up was 16.3% with a standard deviation of 11.3%. No significant correlation was found between NDI and late kyphotic angle. The median value of VAS for pain, at late follow-up was 0 with interquartile range of 0 to 2. Eleven patients (52.4%) reported that they returned to work, whereas 6 patients (28.6%) reported failure to return to their index job (3 of them due to neurological impairment). Furthermore, 2 patients (9.5%) returned to work but with constrained manual duties and 2 patients had never worked before their accidents.
AO Classification
One out of the 21 patients showed type A2 injury (coronal split or pincer fractures) in one level and type C injury in another. F4 subtype (pathologic subluxation or perched/dislocated facet) was detected in all patients; however, 1 patient revealed F4 subtype in one facet and F1 subtype (non-displaced facet fractures) in the other one. Thirteen patients (61.9%) had bilateral facet dislocation or subluxation, and 8 patients (38.1%) had unilateral facet subluxation (5 were on right side while 3 were on left side). According to case-specific modifiers category, M2 subtype (critical disc herniation) was detected in 5 cases (24%) while M3 subtype (stiffening/metabolic bone disease) was detected in one patient, who had diffuse idiopathic skeletal hyperostosis. Seven patients (33%) had N3 subtype (incomplete spinal cord injury).
Operative Data
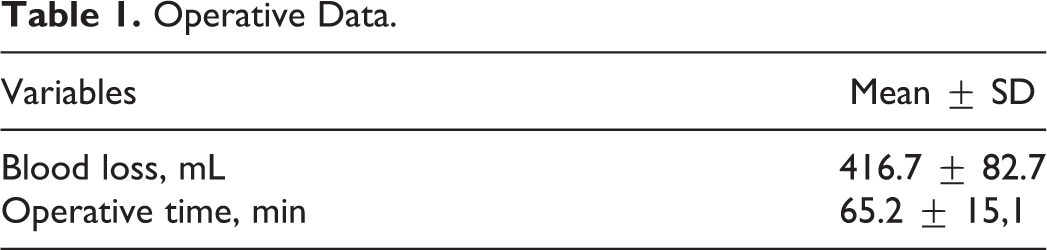
The median value and interquartile range of the period between admission day and the operation day was 3 days (range 2-4 days). Seventeen cases of 21 (81%) were operated upon by junior surgeons while only 4 cases (19%) were operated upon by senior surgeons. Other operative data (blood loss and operative time) is presented in Table 1.
Operative Data.
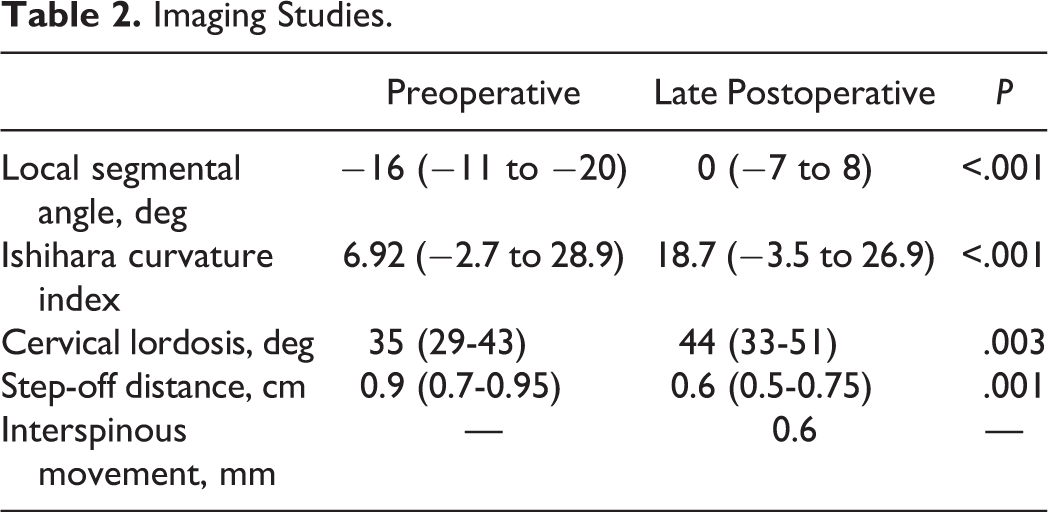
Imaging Studies (Table 2)
The median value and interquartile range are given in Table 2.
Imaging Studies.
Complications
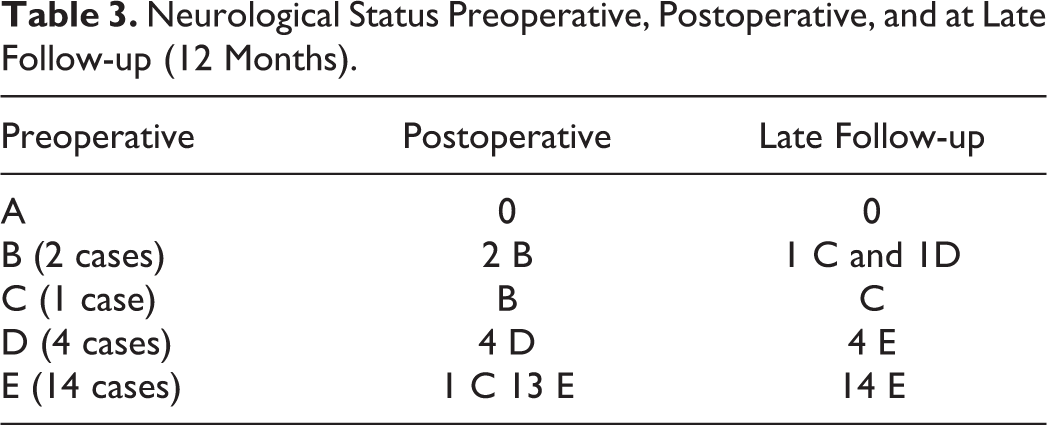
(1) Neurological complications: 2 (9.5%) patients deteriorated postoperation by 1 or 2 grades of AIS (one deteriorated from grade E to grade C, and the other from grade C to grade B); however, both of them improved during late follow-up. This deterioration might be attributed to the manipulations done, to achieve reduction. At late follow-up, 2 (9.5%) patients developed radiculopathy (both of them were grade D preoperatively) (Table 3). (2) Mechanical complications: only 1 case lost reduction at late follow-up; as a result, revision by posterior approach was planned. (3) Dysphagia: 3 patients (14.3%) complained of persistent dysphagia at late follow-up.
Neurological Status Preoperative, Postoperative, and at Late Follow-up (12 Months).
Discussion
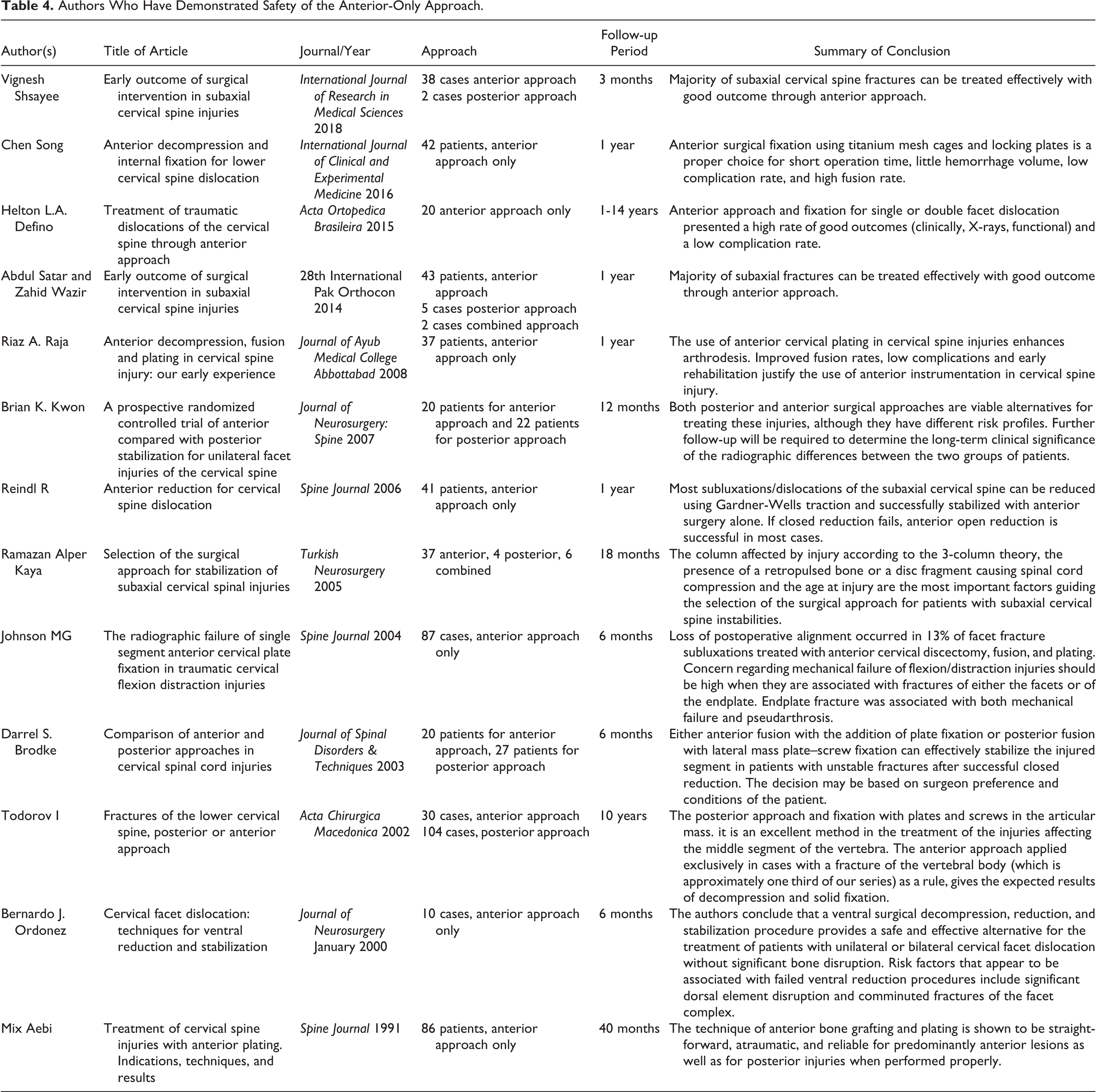
Subaxial cervical spine subluxations and dislocations represent a common injury pattern in active age group. Decision making regarding reduction and surgical approach is still controversial. The AO subaxial cervical spine injuries classification is the most recent universally accepted classification. Type C F4 injuries represent a complex injury pattern. Treatment goals are reduction, decompression, fusion, and stabilization. Different studies reported the use of anterior only approach for treatment of such injuries (Table 4). 4,8 -19 This study focuses on the treatment of complex Type C F4 injuries through anterior only approach. Also, we use the AO classification trying to standardize a common language to describe these injuries. The anterior approach allows easy decompression of the discoligamentous material, which is the most common cause of neurological deterioration in lower cervical spine trauma.
Authors Who Have Demonstrated Safety of the Anterior-Only Approach.
This study reports 21 patients with traumatic subaxial cervical spine injuries. All patients had type C F4 injuries according to the AO classification. Although the local segmental angle improved (increased) at late follow-up, the injured segment was not fully rectified and did not return to the normal lordotic state. This was independent of unilateral or bilateral facet dislocation, as no correlation was detected. On the other hand, there is no significant decrease in late follow-up of local segmental angle compared to early follow-up. Moreover, the normal lordotic state of cervical spine was restored, evidenced by the increase in cervical lordotic angle and Ishihara curvature index during the late follow-up compared to preoperative state. Partial reduction of the injured segment was achieved in all cases, as the step-off distance decreased postoperatively. However, complete reduction was not achieved as the median value of step off distance is 0.6 cm postoperatively, while the normal value should not exceed 0.35 cm. 20
In this study, the anterior approach alone was relatively safe in neurologically free patients with low risk of neurological affection postoperatively. As was shown, only one out of 14 neurologically free cases (7.1%) deteriorated postoperatively but improved at late follow-up. In the current study, 6 out of 7 cases (85.7%) with preoperative incomplete paralysis, showed late follow-up improvement by one or more grade in their AIS. Fusion was 100% documented with CT scan and ISM at the final follow-up. All patients had reported low scores of NDI and VAS. Also, 6 patients (28.6%) reported failure to return to work (three of them due to neurological impairment). Moreover, it was observed that complete anatomical reduction and accurate imaging measures do not correlate significantly to the self-reported outcome measures.
Although, the anterior approach alone can reduce a dislocated cervical segment, but it could not restore normal anatomical alignment in few cases. The results of Defino et al 4 were comparably better, as the reported local segmental angle at late follow-up was at range of 7.55° ± 5.09° of lordosis but there was a loss of 5° lordosis at late follow-up compared with early follow-up. Also, Gao et al 21 showed a better result of 5.2° ± 8.6° lordosis. Contouring of the plate before its application to the cage while performing anterior-only approach is recommended, in order to restore the normal segmental lordotic state.
When compared with data from the literature, no significant difference was noted between anterior and posterior approaches regarding neurological state. The study by Nakashima et al 22 on posterior approach for cervical fracture dislocations with traumatic disc herniation showed that 9 of 12 incomplete paralysis patients (75%) showed postoperative improvement by more than 1 grade in their AIS. In addition, Brodke et al 15 also showed no significant difference between the 2 approaches as 70% and 57% of patients with neurological impairment improved when treated with anterior approach and posterior approach, respectively.
In this study, the fusion state was detected mainly by 2 measures. The first was CT scan at late follow-up, in which the presence of bridging trabecular bone between the endplates and presence of pseudoarthrosis were assessed. The second method was the measurement of ISM on dynamic views, and the median value was 0.6 mm. Riew et al 23 systematically reviewed and recommended the ISM measured to be less than 1 mm, confirms fusion. Accordingly, this study confirmed good state fusion after anterior cervical discectomy and fusion at late follow-up, efficiently.
According to Kown et al, 12 comparison between the anterior and posterior approach depicted no statistically significant differences between the patients. This was supported by similar findings from Del Curto et al. 24
The mean operative time in this study was 65.2 ± 15.1 minutes, while mean blood loss was 416.7 ± 82.7 mL. It is known that the anterior approach takes shorter operative time than the posterior approach, as Kown et al 14 reported that the mean operative time was 103 minutes and the average blood loss was less than 100 mL in posterior approach. Similar results were also reported by Yukawa et al 25 on posterior approach, in which the mean operative time was 101 minutes and the mean blood loss was 190 mL. This confirms that the anterior approach, which takes less operative time, is suitable for patients who cannot withstand a long time of anesthesia and for those with neurological impairment, as time is a critical factor for them. Nevertheless, this study shows that the anterior approach leads to more intraoperative blood loss, compared to posterior approach; however, this might also depend on the surgeon’s experience.
Potential limitations of this study include the relatively small number of subjects in order to establish a significant correlation between the radiological findings and the type of injury or between the self-reported measures and the radiological findings. Moreover, the period of follow-up is short to give an accurate comment on mechanical failure or to detect any pathology that may appear in the adjacent segments.
Conclusion
Surgical treatment of subaxial cervical traumatic injuries by means of anterior reduction decompression and fusion is efficient regarding fusion state and the patients’ satisfaction. Compared with the combined anterior and posterior approach, the anterior-only procedure takes shorter time and appears to be less traumatic to patients. However, the angle of the injured segment does not return to its normal lordosis, and the full reduction is not achieved. Consequently, the anterior approach alone is recommended in cases with neurological impairment and in patients with medical comorbidities or when a short operative time is preferred.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.