
Abstract
Study Design:
Systematic review.
Objective:
Anterior-alone surgery has gained wider reception for subaxial cervical spine facets dislocation. Questions remain on its efficacy and safety as a stand-alone entity within the contexts of concurrent facet fractures, unilateral versus bilateral dislocations, anterior open reduction, and old dislocation.
Methods:
A systematic review was performed with search strategy using translatable MESH terms across MEDLINE, EMBASE, VHL Regional Portal, and CENTRAL databases on patients with subaxial cervical dislocation intervened via anterior-alone approach. Two reviewers independently screened for eligible studies. PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) flow chart was adhered to. Nine retrospective studies were included. Narrative synthesis was performed to determine primary outcomes on spinal fusion and revisions and secondary outcomes on new occurrence or deterioration of neurology and infection rate.
Results:
Nonunion was not encountered across all contexts. A total of 0.86% of unilateral facet dislocation (1 out of 116) with inadequate reduction due to facet fragments between the facet joints removed its malpositioned plate following fusion. No new neurological deficit was observed. Cases that underwent anterior open reduction did not encounter failure that require subsequent posterior reduction surgery. One study (N = 52) on old dislocation incorporated partial corpectomy in their approach and limited anterior-alone approach to cases with persistent instability.
Conclusions:
This systematic review supports the efficacy and success of anterior reduction, fusion, and instrumentation for cervical facet fracture dislocation. It is safe from a neurological standpoint. Revision rate due to concurrent facet fracture is low. Certain patients may require posteriorly based surgery or in specific cases combined anterior and posterior procedures.
Keywords
Introduction
Subaxial C3-C7 cervical spine facet dislocations constitute approximately 10% of all subaxial cervical spine injuries, 40% of which is associated with neurological insult. 1 Anterior stand-alone interbody bone grafting and fusion of subaxial cervical spine fracture dislocation was recognized and widespread following reports by Bailey and Badgley (1960), Cloward (1961), and Verbiest (1962). 2 It was further refined by Bohler (1964), Orozco (1970), Tschern (1971), Senegal (1971), and Gassman and Seligson (1983) with the introduction of plate and screws to tackle earlier complications related to secondary deformity and graft extrusion. 2 The extent of anterior approach included direct anterior open reduction of posteriorly dislocated facets following removal of the disc. 3
Anterior-alone approach is surgically less traumatic owing to its blunt interplane dissections. Infection rate (0.1% to 1.6%) is lower compared with the posterior approach (16%). 4 Direct access to the injured intervertebral disc enables decompression via discectomy. Anterior surgery provides ease of natural supine positioning in contrast to prone positioning in the posterior approach. This minimizes secondary insults in patients with respiratory compromise or other internal organ injuries.
Biomechanical human cadaveric studies, however, advocated anterior surgery for cases devoid of facet fractures. 5,6 Simulated corpectomy cases with intact posterior elements showed superior stability, implying that the severity of posterior elements’ fractures and ligamentous disruption may preclude anterior unicortical screws and plating alone. 5,6 The nature of cervical facet dislocations makes it difficult to study the injuries experimentally. Despite normalization of age and attempted duplication of the clinical injury, these biomechanical simulations used osteoporotic cadaveric specimens that may not accurately represent cervical traumatic facet injuries. Inherent weaknesses of these studies is the lack of normal muscle and ligamentous support of the specimens and the fact that testing occurred in a controlled environment that unfortunately may not accurately duplicate the actual clinical injury.
We conducted this systematic review to analyze the available literature in an attempt to resolve the controversy concerning whether or not anterior stand-alone reduction and stabilization of the cervical spine can be safely and effectively treated following traumatic disruption of the posterior ligamentous column with concurrent facet dislocation by answering the following questions:
Does the anterior-alone approach provide sufficient stability in the treatment of subaxial cervical dislocation with concurrent facet fractures?
Can the anterior-alone approach be employed to perform a successful open reduction of subaxial cervical spine dislocation safely?
How efficacious is the anterior-alone approach in the treatment of unilateral and bilateral subaxial cervical spine dislocation?
How feasible is the anterior-alone approach in treating old subaxial cervical spine dislocation?
Objective
This review aims to determine how the all-encompassing anterior cervical approach can be employed as the sole surgical entity in the operative stabilization of traumatic cervical facets dislocation within the contexts of concurrent facet fractures, anterior open facet reduction—with or without prior attempt of closed traction and reduction, unilateral versus bilateral dislocation, and old dislocation.
Primary Outcomes
Fusion
We denoted fusion or nonfusion attained at final follow-up across the dislocated level treated anteriorly as a marker of efficacy. Spinal stability following successful facet joint reduction and fixation permits effective spinal segment fusion.
Revision Surgery Secondary to Implant Failure
We assigned failure related specifically to implant inserted over the dislocated level in which further retention of such implant would impede stability and fusion and result in untoward clinical consequence to the patients.
Secondary Outcomes
Postoperative Neurological Status
We did not set out to analyze the extent of neurological recovery due to the inherent nature of this injury, which is associated with varying degrees of neurological insult. Instead, we were concerned with whether there was any neurological deterioration following surgery in order to determine if an anterior-alone approach was safe from a neurological standpoint. The primary intent of surgery was to achieve stability and enable early rehabilitation.
Infection Rate and Other Anterior-Related Complications
Infection rate and other complications pertinent to anterior-alone surgery were also evaluated to review the efficacy and safety of this approach.
Method
This systematic review has been registered on PROSPERO (Registration Number: CRD42018116980). 7 -11 Formal National Medical Research Registration was obtained (NMRR-18-3075-44 894). Institutional review board waived approval for this review based on its study design. Items within PRISMA-P 2015 (Preferred Reporting Items for Systematic Review and Meta-Analysis–Protocols) checklist were adapted to formulate the following methodologies. 12 Bibliographic databases Ovid-Medline, Ovid-EMBASE, CENTRAL, and VHL-Regional-Portal were searched using controlled vocabulary MESH terms that were translatable and customized for use across databases (Supplemental Appendix 1). No time limit and no language restrictions were imposed in the search strategy (Supplemental Appendix 2).
Two reviewers independently screened titles and abstracts retrieved based on predefined inclusion and exclusion criteria (Supplemental Appendix 3). The review included all types of study designs except case series and case report that focused on traumatic subaxial cervical spine facets dislocation in adults aged 18 years and older. Population with spondyloarthropathies, namely, ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis, and rheumatoid arthritis, were excluded. Screenings of studies in the non-English language(s) were translated via Google Translate. 13 Full texts were sought in the event of ambiguity. Discrepancy was resolved through discussion between the reviewers. Non-English language(s) studies did not meet the inclusion criteria of this review.
The search strategies yielded a total of 1118 records. A total of 949 records remained after removal of duplicates. A total of 903 studies were excluded following the screening of titles and abstracts. Full texts of 46 studies were assessed for eligibility. Thirty-seven studies were excluded. Nine retrospective studies fulfilled all inclusion criteria and were included in this review 4,14 -22 (Supplemental Appendix 4). No additional relevant studies were retrieved during the rerun of search strategies prior to data analysis.
Data management utilized Zotero software program as referencing manager. Data from selected studies was subsequently extracted from full text retrieved online according to the domains specified within the pro forma in relation to study and participant characteristics, interventions, and outcomes (Supplemental Appendix 5).
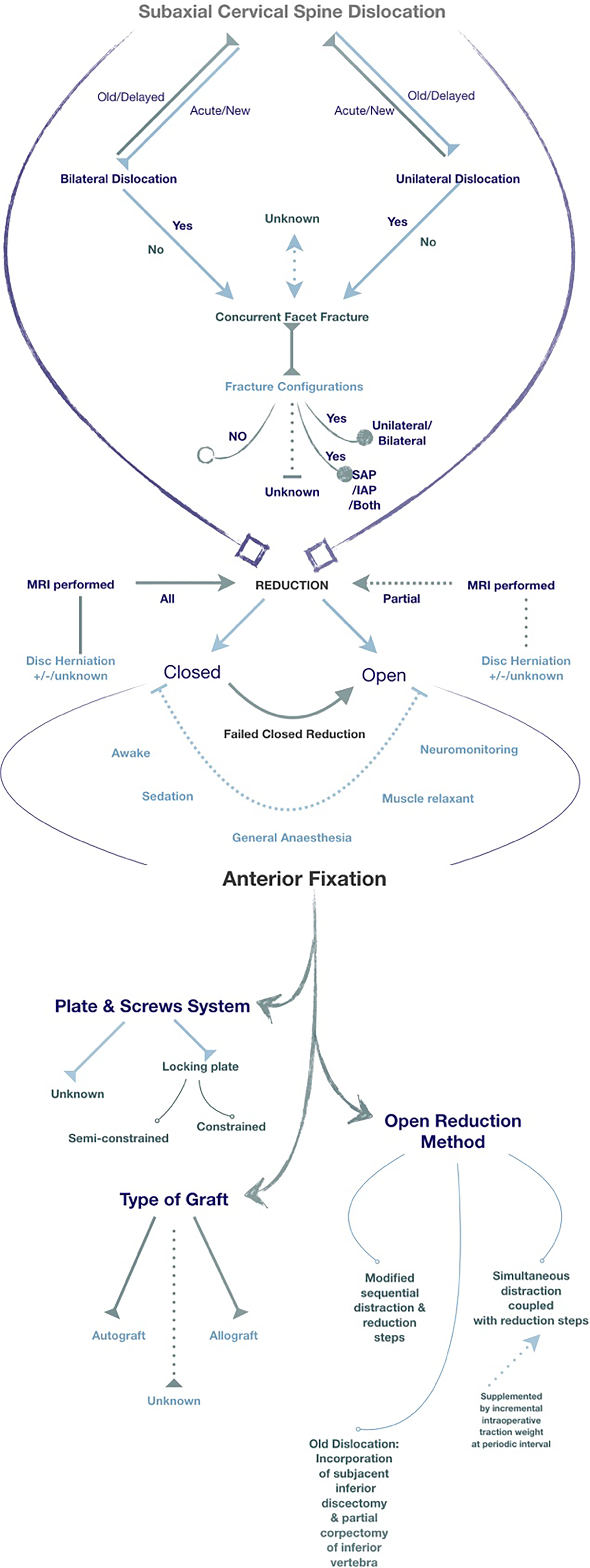
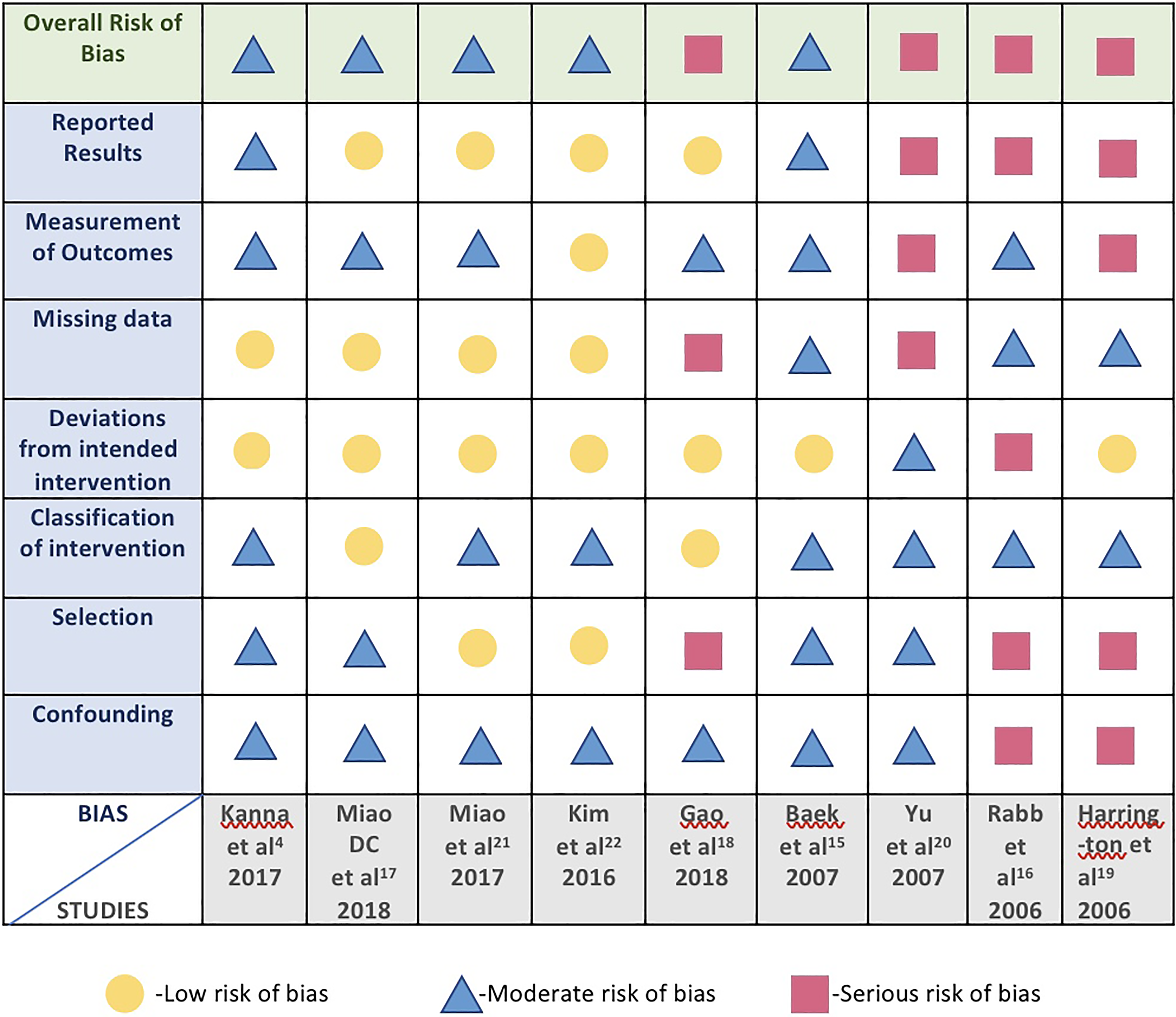
A narrative synthesis for the review was performed. Data concerning the outcomes across the contexts specified was appraised alongside a tabular narrative summary. Quantitative meta-analysis was not performed due to substantial clinical heterogeneity across the studies retrieved (Figure 1). 4,15 -22 Individual studies were assessed for risk of bias with ROBINS-I tool. 23
Results (Tables 1 and 2)
Primary Outcomes
Fusion
In this review, nonunion was not encountered. All studies reported fusion across all contexts analyzed. Anterior cervical fusion surgery adapts Wolffs’ law load sharing principle of axial compression onto the interbody graft with eventual incorporation and fusion across 2 subjacent end-plates. 24 Constrained plate system that was intended for rigid fixation in the traumatic setting to prevent screws back out via screws-to-plate locking mechanism had been criticized for predisposition to pseudoarthrosis, as the vertebral bodies affixed to the rigid construct were shielded from physiological axial stress loading onto the graft. Semiconstrained translational and rotational systems that were later designed to counteract the shortfalls of the constrained system also faced the critique of increased hardware failure and did not demonstrate a significant difference in the rate of fusion. 25 The plate systems used in the studies of this review were not homogenous. Three studies reported the use of locking plates with unknown fully constrained or semiconstrained locking mechanism. 4,18,21 One study 16 had a mixture of both while another study utilized semiconstrained alone. 22 The remaining 4 studies did not specify the types of plate used. 15,17,19,20 Autologous versus allograft interbody graft were also weighted for their differential superiority to fusion. Kim et al 22 in their comparison on dislocation cases treated with autograft versus allograft obtained solid fusion in both groups. Similar results were observed in Kanna et al 4 and Rabb et al 16 in which the types of graft used were reported in their surgical demographics.
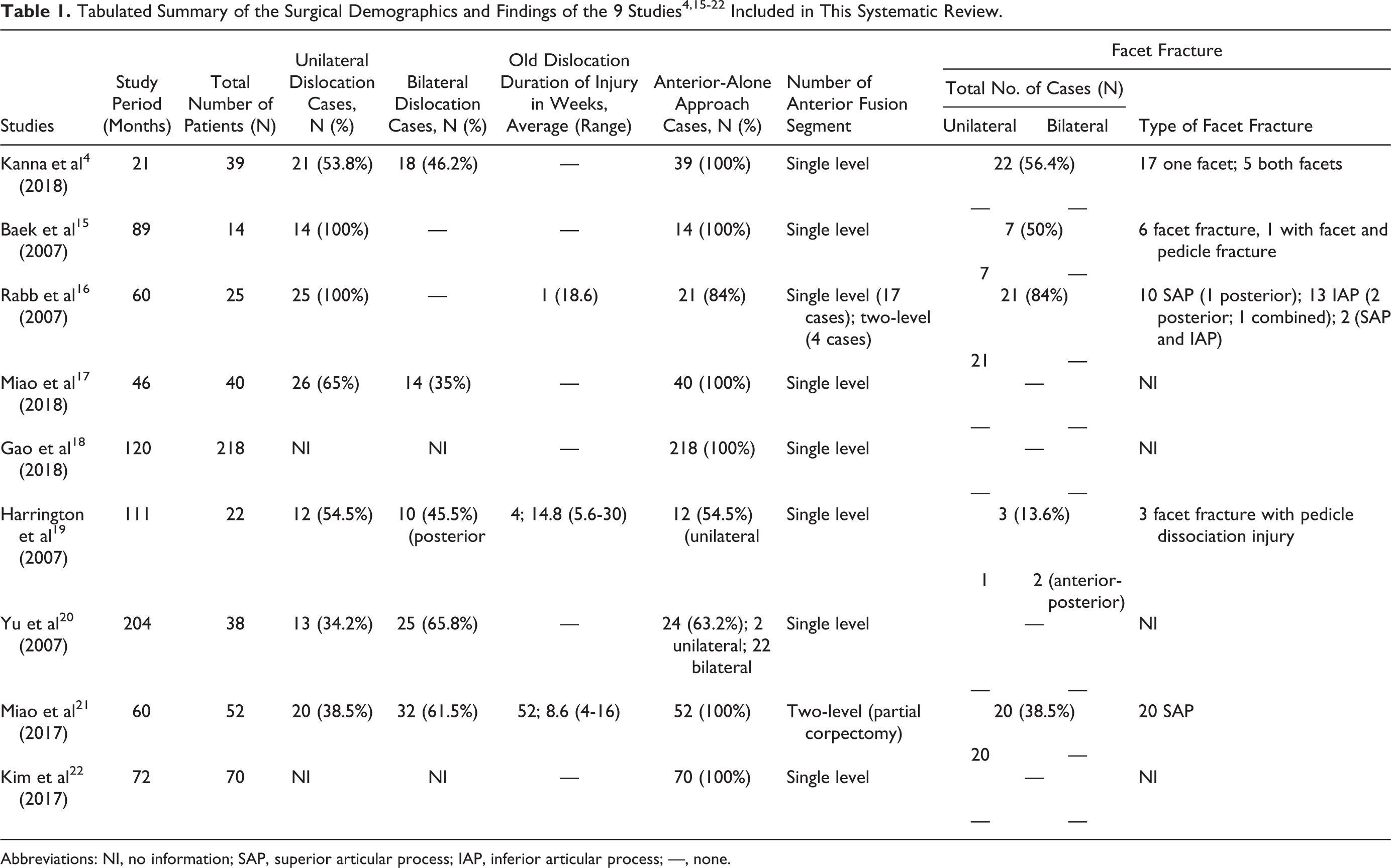
Abbreviations: NI, no information; SAP, superior articular process; IAP, inferior articular process; —, none.
Tabulated Summary of the Surgical Demographics, Findings, and Outcomes of the 9 Studies4,15-22 Included in This Systematic Review.
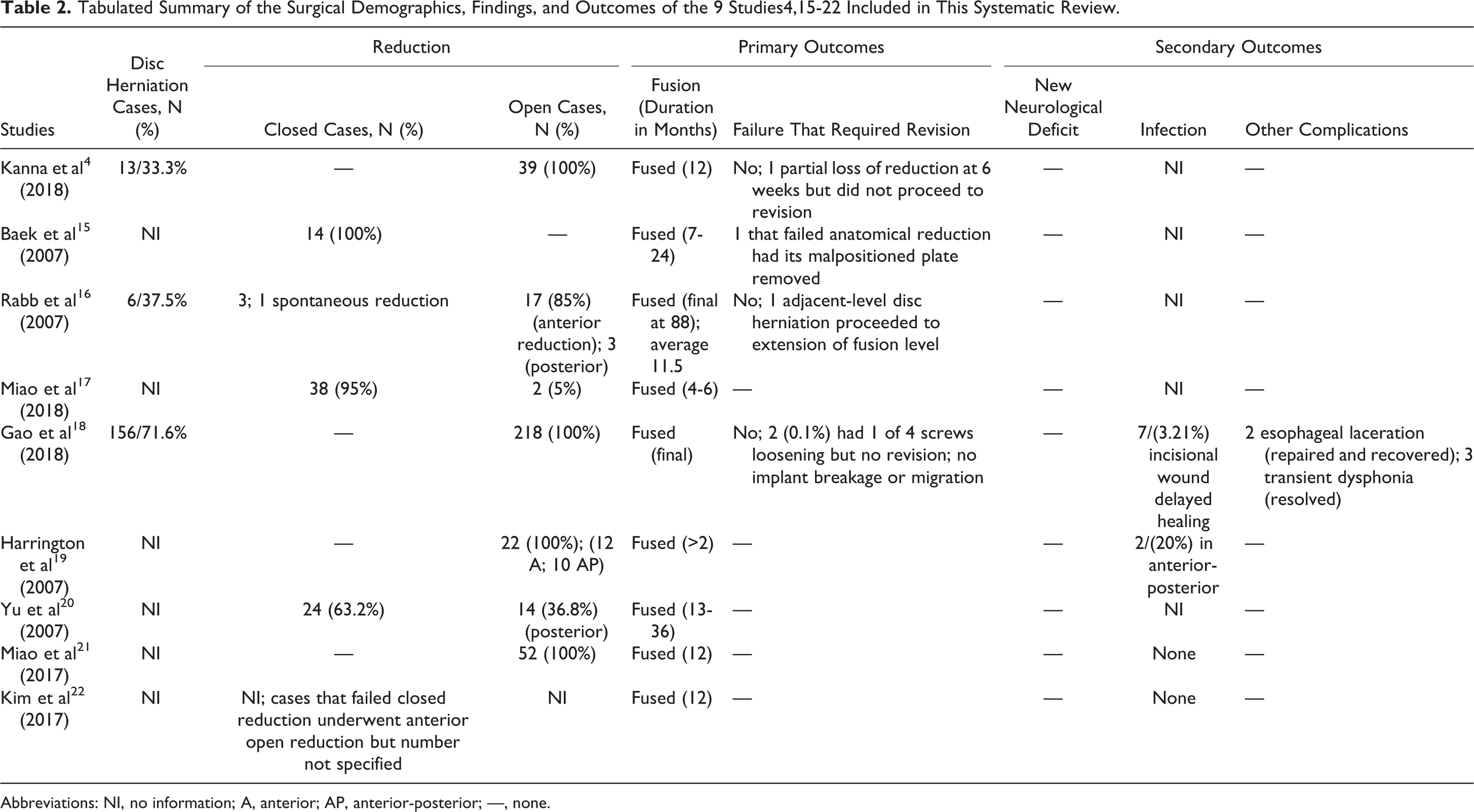
Abbreviations: NI, no information; A, anterior; AP, anterior-posterior; —, none.
No standard nomenclature or gold standard exists to assess fusion in the cervical region. Heterogeneous usage of plate systems and interbody grafts led to the suggestion of computerized quantitative analysis to determine a clinically relevant threshold for fusion. 25 General consensus across the studies included in this review, however, denoted fusion by radiological bridging trabeculae, absence of a radiolucent gap between the graft and end-plate junctions, and less than 2 mm motion in dynamic flexion-extension lateral radiographs. 26 Despite the initial perception of an absent or doubtful radiological union, subjective interpretations continued to observe eventual clinical fusion as patients remained asymptomatic throughout.
Revision Surgery Secondary to Implant Failure
Baek et al 15 encountered plate malpositioning in a case of unilateral facet dislocation with inadequate reduction due to fracture fragment between the facet joints. The plate was removed following fusion. Rabb et al 16 performed a subsequent extended fusion on 1 case with adjacent degenerative disc herniation. Missed disc herniation on the index care episode was not considered as failure.
Secondary Outcomes
Neurological Status
Heterogeneity of preoperative and postoperative neurological recovery are confounded by a multitude of factors. One is the inherent nature of the extent of preexisting neurological insult, which if present, preclude meaningful clinical correlational significance. In this review, anterior-alone approach for subaxial cervical dislocation was safe from a neurological standpoint as no new neurological deficit was observed across all contexts analyzed.
Infection
Gao et al 18 encountered 7 (3.21%) delayed incisional wound healing while 2 out of 10 (20%) within the anterior-posterior group in Harrington et al 19 were complicated with wound leakage and superficial wound infection. Miao et al 21 and Kim et al 22 reported no complication related to wound infection. The remaining 5 studies did not mention on issues pertaining to infection. 4,15 -17,20
Other Complications
No other studies in this review except Gao et al 18 reported inadvertent esophageal laceration as a result of excessive retraction and brusque soft tissue handling. No esophageal fistula or dysphagia ensued following intraoperative repair. Three had transient dysphonia due to recurrent and superior laryngeal nerve neuropraxia that resolved at 3 to 6 months.
Discussion
Does the Anterior-Alone Approach Provide Sufficient Stability in the Treatment of Subaxial Cervical Dislocation With Concurrent Facet Fractures?
In our review, all cohorts from the 5 studies 4,15,16,19,21 with concurrent facet fracture (N = 71) went on to attain fusion. Low failure rate of 0.01% was demonstrated. One case could not attain anatomical closed reduction due to bony fractured fragments in between the dislocated facet. 15 The malpositioned plate was removed after fusion. In contrast, the literature reported a statistically significant correlation between facet fracture with radiographic failure (13%; 11 out of 87). 27 The authors, however, acknowledged that it was beyond the scope of their study to determine the clinical significance of their radiographic failure despite statistical findings as fusion rate was not assessed and no follow-up ensued at the point of radiographic failure. 27 Also, there was a paucity of facet fracture variants delineation, both in the existing literature and the studies reviewed. Of the 2 studies in this review that reported horizontal variant of facet fracture with pedicle dissociation injury (N = 4), 50% involving unilateral dislocation underwent single-level fusion. 15,19 The remaining 50% with bilateral involvement had combined anterior-posterior surgeries that were decided pre-operatively. 19 Shanmuganathan et al 28 suggested 2 contiguous segments fusion for this fracture variant to improve stability as the loss of vertebral body continuity from the posterior facet was thought to compromise optimal anatomical reduction via the anterior approach. The disparate success and feasibility of our study findings could be attributed to preservation of contralateral vertebral body-pedicle continuity in unilateral dislocation cohorts. The studies, which reported facet fracture involving superior articular process or inferior articular process, or both, did not specify the exact fracture variant. 4,15,16 If, according to the vertical or oblique fracture variant, as described by Sim et al, 29 whereby more than half the height of facet fracture impaction is considered stable, a question in reversal may be postulated as to how much of articular pillar’s volumetric dimension has to be fractured to either require 2 segment fixation, as seen in Rabb et al 16 cohort, or preclude anterior single-segment treatment altogether. The low rate of failure in this review attested to the relative stability of this second variant, as demonstrated by the fusion that was attained in the case of Baek et al 15 despite malpositioned plate due to incomplete anatomical reduction.
Can the Anterior-Alone Approach Be Employed to Perform a Successful Open Reduction of Subaxial Cervical Spine Dislocation Safely?
Seven studies (N = 350) in this review revealed successful and safe anterior open reduction without posterior revision and neurological deterioration. 4,16 -21 Of these, 99.4% did not attempt prior closed traction and reduction. 4,18,21 A total of 68.4% from 4 studies (N = 117) proceeded with anterior approach only after successful closed traction and reduction. 15 -17,20 In effect, both closed and anterior open reduction are indirect reduction as the facets cannot be visualized within the surgical field but rather through fluoroscopy. Discectomy decompression in anterior open reduction, however, confers an advantage in reducing the force needed to attain the drafting distance, as described by Miller et al, 30 to distract the facets to a perched position in that of closed traction and reduction. In contrast to our review findings, 1 out of 10 in Ordonez et al 31 and 2 out of 8 in Reindl et al 32 could not be reduced via the anterior approach. Failure of reduction was attributed to complex comminuted facet fractures and the observed pedicle-body facet fracture discontinuity respectively. Additionally, Reindl et al 32 included subjects with cervicothoracic C7-T1 dislocations and preexisting ankylosed spine in their cohorts, which could have increased the heterogeneity of the study population. In our review, Kanna et al 4 attributed their successful open reduction to their extended decompression beyond the posterior longitudinal ligament (PLL) and uncovertebral joint despite the presence of facet fractures. They also highlighted the pertinent derotatory maneuver via modified Caspar pin placement perpendicular to the plane of dislocated vertebra to counteract the rotatory vector in aiding the reduction of unilateral dislocation, which has been shown to require greater weight and difficulties in closed reduction. 29,33
Concerning the safety of anterior open reduction, no neurological deterioration was encountered across all the studies in this review. Prior to the report by Eismont et al 34 on neurological catastrophe following closed reduction, magnetic resonance imaging (MRI) was not weighted as a prerequisite to look for herniated disc before reduction. While they were later commented for performing the procedure under general anesthesia instead of awake reduction, the exact causes of such deficits remained uncertain. Some attributed it to overdistraction, preexisting noncontiguous lesion, epidural hematoma, and cord edema. 34,35 Anterior discectomy context affords direct decompression of the injured cord. Nonetheless, closed traction and reduction still serves as a measure of indirect decompression as soft disc herniation had been observed to reduce back into place. 36 Residual cases with disc herniations that remained, as well as new disc herniations reported in postreduction MRI, were shown not to be related to any adverse neurological outcomes. 32,36,37
How Efficacious Is the Anterior-Alone Approach in the Treatment of Unilateral and Bilateral Subaxial Cervical Spine Dislocation?
Unilateral dislocation differs from a mechanistic standpoint compared to bilateral dislocation. In vitro study model demonstrated consistent unilateral dislocation even when the supraspinatous, interspinous, and PLL were intact. 33 Bilateral facet dislocation, however, involves substantial discoligamentous injuries due to failure in withstanding the distractive tensile load. Quasistatic tensile modulus loading test showed that the posterior annulus is consistently weaker than anterior annulus across all loading strength and direction. 38 In hyperflexion injury, the posterior annulus disintegration renders disc insults with or without nucleus herniation. 39 Concern thus arises over the stability of the anterior-alone approach in withstanding the marked posterior tension band injury in bilateral dislocation compared to unilateral dislocation. In this review, unilateral dislocations that underwent the anterior-alone approach demonstrated a low failure rate of 0.86% (N = 1 out of 116). 4,15 -21 Baek et al 15 did not detail if PLL was decompressed during anterior discectomy in the case that failed closed anatomical reduction, as shown to be likely intact in in vitro study. 33 Meanwhile, 1.16% (1 out of 86) 4,17,20,21 of bilateral facet dislocations encountered partial loss of reduction at 6 weeks but did not proceed to revision surgery as the patient remained asymptomatic and went on to attain fusion at final follow-up. 4 It was not certain if the bilateral dislocation had concurrent facet fracture. Two other studies did not describe any associated facet fracture. 17,20 Within the given contexts in this review, anterior-alone approach is efficacious in bilateral dislocation without extensive facet fractures. Be it closed or open reduction, discectomy followed by interbody structural grafting and plating in both unilateral and bilateral dislocations translate to attainment of optimal fusion alongside the added benefit of maximal direct decompression. 40 Fusion afforded by interbody graft cross-sectional bed synthetically seeks to mimic and replicate compressive load that can be applied to that of the innate intervertebral disc. As fusion and stability act on each other in a synergistic manner, restoration of near-physiological lordosis anteriorly aids in stabilizing the motion segment if facet reduction is adequately achieved. A mechanically sound anterior-alone fixation may well rival the rigidity of that of the posterior approach as the preservation of both intrinsic and extrinsic posterior muscles in the anterior approach lends support in flexion by its physiological restraint and contraction. The low occurrence of failure in the studies reviewed attests to the efficacy of this approach as the role afforded by the posterior musculature cannot be tested with biomechanical studies, as all specimens have to be stripped off its muscles, leaving only bones and ligaments. 41,42
How Feasible Is the Anterior-Alone Approach in Treating Old Subaxial Cervical Spine Dislocation?
In contrast to the combined anterior-posterior approach commonly performed in old dislocation, Miao et al’s cohort (N = 52) successfully underwent anterior-alone approach but conceded to the limitation of this approach to cases with persistent instability on dynamic radiographs. 21 Following extensive anterior decompression with partial corpectomy, the residual mobility allowed distraction of posterior scar contracture to attain a parallel realignment between subjacent end-plates. The authors discounted absolute need of anatomical reduction as they believed that segmental alignment coupled with greater volumetric anterior column support afforded sufficient clinical stability for fusion to take place within the acceptable parameter. Nonetheless, the authors acknowledged the importance of anticipating combined approach in the event that obstacles should arise intraoperatively.
Weaknesses of the Study
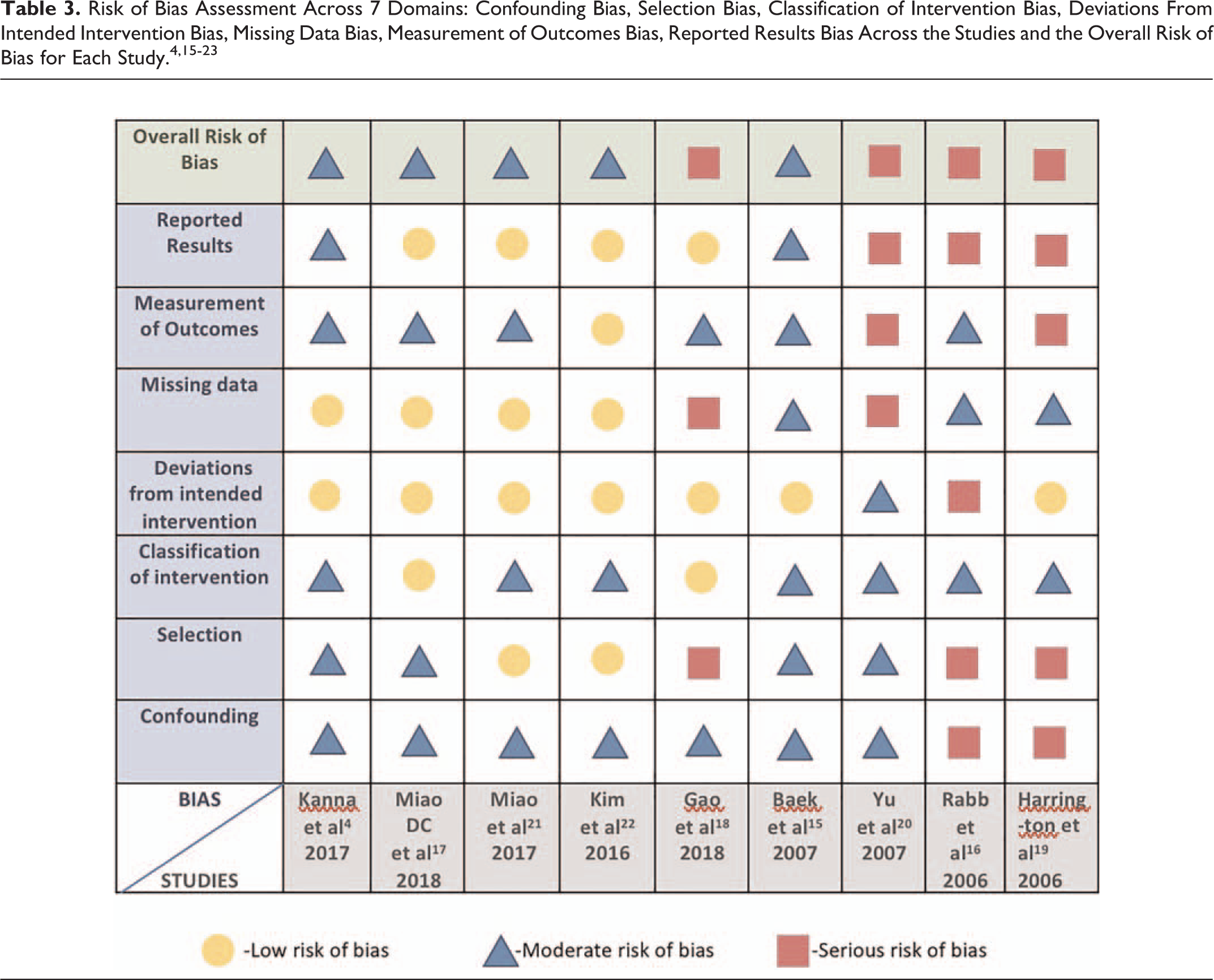
Overall, there is a substantial degree of bias throughout this study, given the heterogeneity of the samples (Table 3, Figure 1). Clinical heterogeneity is regarded as an impediment to well-conducted studies. Perhaps heterogeneity in this review offers insights into the reception of this injury by surgeons across the board. Recruitment of large numbers of subjects is confronted with differing demographics in different regions worldwide. Challenges pervade as certain regions still face difficulty in accessing a Level 1 trauma center, patient transfer, and the varying level of infrastructures and facilities. In a difficult-to-study realm with striking clinical significance such as this, long latency period from the time of surgical treatment to eventual study period and publication lacked synchronization as changes in detail elements of surgical approaches may have taken place as surgical communities continue to refine them through time. Collation of patient records spanning more than a decade long in 2 studies resulted in a substantial number of missing data due to lost-to-follow-up and incomplete records. 18,20
Risk of Bias Assessment Across 7 Domains: Confounding Bias, Selection Bias, Classification of Intervention Bias, Deviations From Intended Intervention Bias, Missing Data Bias, Measurement of Outcomes Bias, Reported Results Bias Across the Studies and the Overall Risk of Bias for Each Study. 4,15 -23
Clinical Relevance and the Impact of This Study on Clinical Practice
Although we did not analyze the extent of neurological recovery in this review, the STASCIS trial showed improved neurological outcome with early decompression being performed within 24 hours of injury. 43 Closed awake traction and reduction of facet dislocation decompress the spinal cord as the discs have been shown to be reduced back into place. 36 This form of indirect decompression is relevant in logistic settings wherein the spine surgeons are not immediately available. We recommend that anterior open reduction may be employed in centers with readily available spine surgeons as this review has shown that anterior-alone approach is feasible and safe from the neurological standpoint. Importantly, anterior discectomy directly decompresses the spinal cord and aids in facet reduction. Direct anterior decompression can reduce the delay in time to surgery as some centers still face prolonged waiting time for MRI to be performed. Adequate follow-up is necessary as our review showed that radiographic failure may not be tantamount to clinical failure as follow-up through time revealed fusion despite some initial hardware malpositioning. We acknowledge that the number of studies in this systematic review may be rather small to propose that this approach is infallible. Delineation of facet fracture configurations in relation to its volumetric disruption and presence of isolated articular mass fracture due to pedicles-body discontinuity in future studies may better inform the extent of fixation needed to improve stability, either by 2 rather than 1 level anterior approach or its alternative counterparts. We do not intend to dismiss the roles of posterior and/or combined anterior-posterior approaches in this realm as failure to achieve reduction of the dislocation via the anterior approach will require the surgeons to resort to anterior-posterior-anterior surgeries.
Conclusion
The systematic review of the currently available cervical trauma literature supports the efficacy and success of anterior reduction, fusion, and instrumentation for facet fracture dislocations. It is safe from a neurological standpoint. Nonunion was not encountered. Revision rate due to concurrent facet fracture is low. Certain patients may require posteriorly based surgery or in specific cases combined anterior and posterior procedures.
Supplemental Material
Supplemental Material, Appendix_1_to_5 - Anterior-Alone Surgical Treatment for Subaxial Cervical Spine Facet Dislocation: A Systematic Review
Supplemental Material, Appendix_1_to_5 for Anterior-Alone Surgical Treatment for Subaxial Cervical Spine Facet Dislocation: A Systematic Review by Wendy Lee and Chung Chek Wong in Global Spine Journal
Footnotes
Authors’ Note
This research was undertaken as part of the third year of the MSc in Surgical Sciences, University of Edinburgh (W.L.).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.