
Abstract
Study Design
Retrospective evaluation of consecutively performed fluoroscopically guided cervical nerve root blocks.
Objective
To describe the incidence of injectate central epidural flow with respect to needle tip position during fluoroscopically guided extraforaminal cervical nerve root blocks (ECNRBs).
Methods
Between February 19, 2003 and June 11, 2003, 132 consecutive fluoroscopically guided ECNRBs performed with contrast media in the final injected material (injectate) were reviewed on 95 patients with average of 1.3 injections per patient. Fluoroscopic spot images documenting the procedure were obtained as part of standard quality assurance. An independent observer not directly involved in the procedures retrospectively reviewed the images, and the data were placed into a database. Image review was performed to determine optimal needle tip positioning for injectate epidural flow.
Results
Central epidural injectate flow was obtained in only 28.9% of injections with the needle tip lateral to midline of the lateral mass (zone 2). 83.8% of injectate went into epidural space when the needle tip was medial to midline of the lateral mass (zone 3). 100% of injectate flowed epidurally when the needle tip was medial to or at the medial cortex of the lateral mass (zone 4). There was no statistically significant difference with regards to central epidural flow and the needle tip position on lateral view.
Conclusion
To ensure central epidural flow with ECNRBs one must be prepared to pass the needle tip medial to midplane of the lateral mass or to medial cortex of the lateral mass. Approximately 16% of ECNRBs with needle tip medial to midline of the lateral mass did not flow into epidural space. One cannot claim a nerve block is an epidural block unless epidural flow of injectate is observed.
Introduction
Extraforaminal cervical nerve root block (ECNRB) is a diagnostic and therapeutic alternative in the management of cervical pain when the clinical and radiologic workup fails to provide an appropriate diagnosis and noninvasive measures have failed to provide relief of patients’ symptoms. 1 Fluoroscopically guided ECNRBs are relatively safe procedures in experienced practitioners’ hands utilizing a technically safe approach. 2 , 3 , 4 Precise needle tip positioning is critical, as improper placement diminishes the procedure's therapeutic and diagnostic potential while increasing the probability for complications. 3 The cervical nerve block guidelines established by the International Spine Intervention Society state that the optimal position of the needle tip “should lie opposite the sagittal midline of the silhouettes of the articular pillars. The needle should never be advanced beyond a vertical line connecting the uncinate processes.”5 Others have made similar statements. Windsor et al states that the needle tip should not be medial to the midportion of the pillar in a true anteroposterior view. 6 If a large spread into the epidural space is desired in a cervical extraforaminal steroid injection, the larger the foraminal size and the larger the injected volume, the higher degree of epidural flow. 7 But how can the likelihood of epidural flow during ECNRB be increased without increasing the injectate volume or selecting patients with larger neural foramina? The goal of this work is to determine the ideal needle tip position to maximize epidural flow of the injected material (injectate) during cervical extraforaminal nerve blocks. It may be claimed that computed tomography (CT)-guided blocks have replaced fluoroscopically directed ECNRBs, but it is the experience of the senior radiologic author of this article that fluoroscopically controlled cervical nerve root blocks (CNRBs) are still being performed. It is also the experience of the senior radiologic author that a cervical epidural block maybe claimed to have been performed, although no contrast was shown to have passed into the epidural space. That is the rationale for reviewing some older material to illustrate some persistent problems in performing and providing interpretations about CNRBs.
Materials and Methods
All patients who received a fluoroscopically guided ECNRB at our institution between February 19 and June 11, 2003, were included in the present retrospective study. Overall, 132 injections were performed on 95 patients, for an average of 1.3 injections per patient. The mean age of the patients at the time of injection was 48 years (ranging from 25 to 79 years of age); 51.5% of the patients were women, and 48.5% were men. The large majority of patients had symptoms related to either disk herniation or foraminal stenosis and had been referred by a single orthopedic spine surgeon. Blocks were performed either for verification of a pathologic nerve root level or to prevent or delay the need for surgery. The injections were performed by or under the direction of four attending radiologists in our radiology department. All four radiologists used a standardized technique, which was verified prospectively by the senior radiologist by means of a quality assurance review of all the injections.
For the procedure, each patient was placed in the lateral decubitus position with the side of interest elevated toward the patient's face. C-arm fluoroscopy was used to place a 25-gauge needle (usually a 2-inch and rarely a 3½-inch-long needle in patients with a very large neck or with a low position in the neck) into the extraforaminal area at the level of interest. The overhead fluoroscopy tube was angled toward the patient's face to show a very slight oblique entry site, so that the foramen of interest was barely profiled in a very shallow oblique view as described in literature. 3 The needle was inserted to slide along the anterior surface of the articular pillar (lateral mass) and was kept as posterior as possible to avoid the vertebral artery. To ascertain that the needle tip was not located in a vascular structure, myelographic contrast material, iohexol (Omnipaque 180 or 300; GE Healthcare, Princeton, NJ, United States), was injected prior to final injection of the anesthetic, medication, and contrast material mixture (injectate). Once the needle was positioned, 0.5 mL of methylprednisolone acetate suspension (Depo-Medrol 80 mg/mL; Pharmacia-Upjohn, Kalamazoo, MI, United States) with 0.5 mL of 2% preservative-free Xylocaine (Abbott Laboratories, North Chicago, IL, United States) and 0.5 mL Omnipaque 180 or 300, for a total volume of 1.5 mL, was injected. Images were made during and after injection to verify needle tip placement and to evaluate for extent of flow of the injectate. Contrast was added to the final fluid injected to better evaluate extent of injectate flow, rather than just watch washout of the test-injected contrast material. Due to the fact that different persons performed the procedures and requests varied from asking for a nerve block or for a foraminal epidural, the depth of the needle tip varied among the patients.
A duplicate fluoroscopic record of each procedure was obtained prospectively as part of our standard quality assurance protocol. An independent observer (K.R.S.) who had not been involved in the procedures reviewed a prospectively kept database on all patients who had undergone cervical nerve blocks during the study period. Radiographs were reviewed, and the needle position in the frontal view was noted and labeled. Uncertainties about needle position were resolved by means of a consensus between the independent reviewer and the senior radiologist author (L.A.G.).
On the frontal view, needle depth was measured with use of the lateral mass as a marker. Needle tips that were peripheral to the lateral border of the lateral mass were labeled as being in zone 1 (Fig. 1). Needle tips overlying the lateral mass but lateral to the midline were labeled as being in zone 2. Needle tips overlying the medial half of the lateral mass but within the lateral mass were labeled as being in zone 3. Needle tips at the medial cortex of or medial to the lateral mass were labeled as being in zone 4. Needle tips that were on the boundary between zones were labeled as being within the deeper zone.
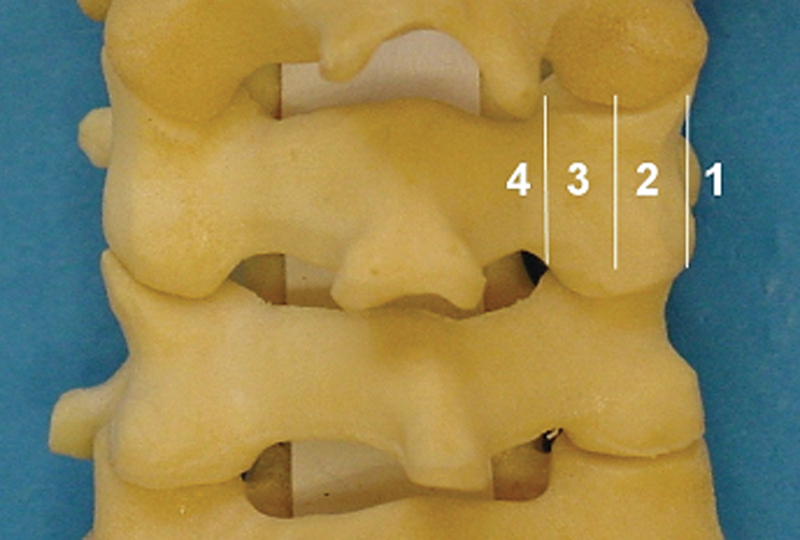
Cervical spine model demonstrating various frontal zones. Zones 1 through 4 are described in the text. (Reprinted with permission from Ma D, Gilula LA, Riew KR. Complications of fluoroscopically guided extraforaminal cervical nerve blocks. An analysis of 1036 injections. J Bone Joint Surg Am 2005;87:1025–1030.)
On the lateral view, ideal needle tip placement (defined as placement directly on the anterior edge of the lateral mass) was labeled as zone A (Fig. 2). Needle positions that were within two needle-tip diameters anterior to zone A were labeled as zone B. Positions further anterior than zone B were labeled as zone C (Fig. 2). Radiographs with inadequate lateral views were labeled U. Radiographs were labeled inadequate if the bilateral lateral masses did not overlap each other by at least 50%.
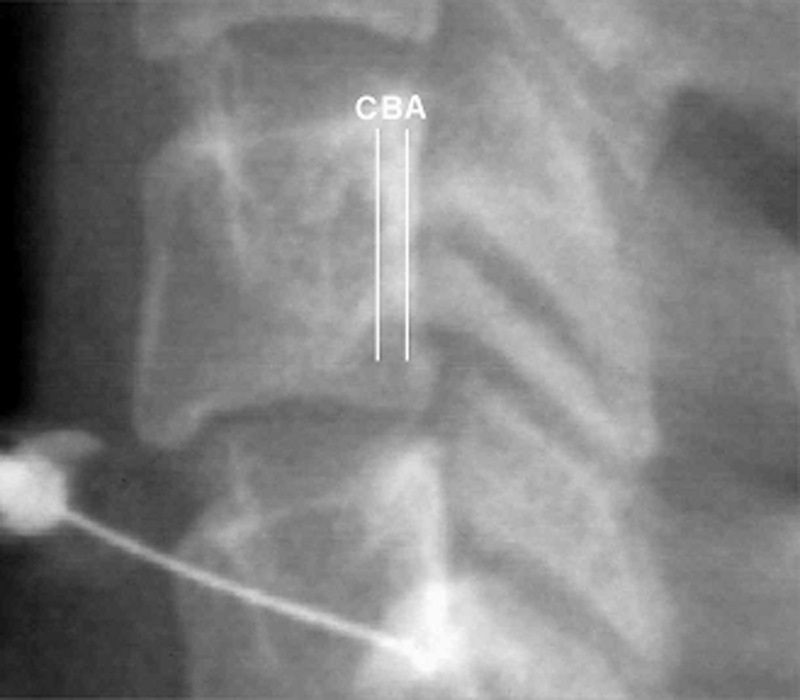
Lateral cervical spine fluoroscopic spot image demonstrating various lateral zones. Zones A, B, and C are described in the text. (Reprinted with permission from Ma D, Gilula LA, Riew KR. Complications of fluoroscopically guided extraforaminal cervical nerve blocks. An analysis of 1036 injections. J Bone Joint Surg Am 2005;87:1025–1030.)
Institutional review board approval was obtained for this retrospective study.
Results
Frontal and lateral fluoroscopic spot images were reviewed to assess for central epidural flow. There was uncertainty regarding the degree of central epidural flow utilizing frontal and lateral fluoroscopic spot images in six injections. No injections were classified as zone 1. In zone 2 (n = 45), 13 injections demonstrated central epidural flow and 32 were without central epidural flow. Therefore, 28.9% of zone 2 injections had an epidural effect. In zone 3 (n = 74), 62 injections demonstrated central epidural flow and 12 were without central epidural flow (Fig. 3). Therefore, 83.8% of zone 3 injections had an epidural effect. In zone 4 (n = 7; Fig. 4), all 7 injections demonstrated central epidural flow and therefore had an epidural effect. Therefore, there is a statistically significant difference in epidural flow of the injectate comparing zones 3 + 4 with zone 2 (p < 0.01). With regards to needle tip position in the lateral view, inadequate lateral fluoroscopic spot images were obtained in 20 injections. In zone A (n = 97), 64 injections demonstrated central epidural flow and 33 were without central epidural flow. Therefore, 66.0% of zone A injections had an epidural effect. In zone B (n = 6), 5 injections demonstrated central epidural flow and 1 was without central epidural flow. Therefore, 83.3% of zone B injections had an epidural effect. In zone C (n = 3), 1 injection demonstrated central epidural flow and 2 were without central epidural flow. Comparing zone A with zones B + C, zone A (66.0%) appears better than zones B + C (66.7%); however, there was no statistically significant difference with respect to epidural flow.
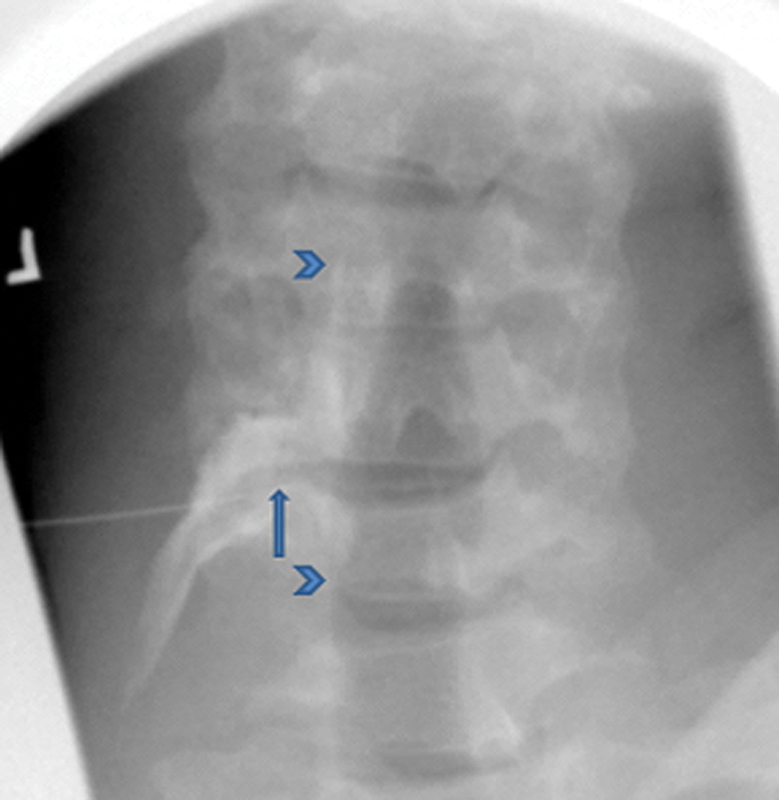
Frontal radiograph of the cervical spine with needle tip in zone 3 (arrow) demonstrating epidural flow of the injectate (arrowheads).
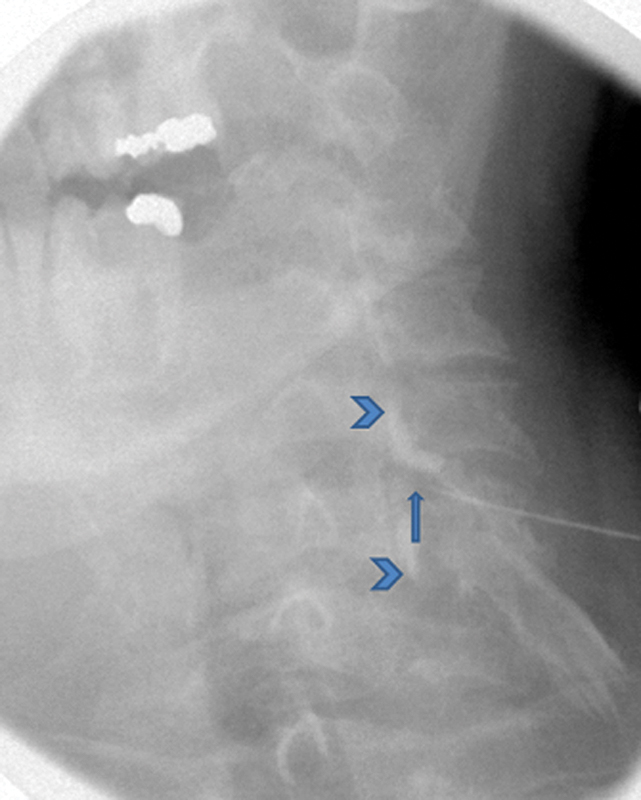
Frontal radiograph of the cervical spine with needle tip in zone 4 (arrow) demonstrating epidural flow of the injectate (arrowheads).
Discussion
Transforaminal epidural steroid injections are widely utilized for the treatment of cervical disorders. Although they can be clinically beneficial, lateral placements of the needle tip can result in failure of epidural spread to the offending area of pathology. However, it is not proven that epidural flow of injectate in the cervical spine improves clinical outcome or leads to longer pain relief compared with injectate placed lateral to the epidural space. Cervical nerve blocks can be associated with catastrophic complications, including stroke, death, and paralysis when the injectate is inadvertently placed into the vertebral artery, neural tissue, or intradural space. A needle that is placed too lateral to the foramen may not result in substantial epidural spread of the injectate, whereas one too medial might increase the risk of perforating the dura, and if too anterior, may injure the vertebral artery. Critical to increasing the success and minimizing the complication rates is accurate placement of the needle tip and verification of injectate flow with contrast material. Despite this, we are unaware of any study that has evaluated the ideal position of the needle tip to ensure epidural spread when attempting to or claiming to perform a transforaminal epidural injection.
This work was performed because in the personal experience of the senior author, injectate did not always pass epidurally with foraminal and extraforaminal nerve blocks. Also, despite the fact that procedures performed by others outside and inside this institution were said to have been epidural injections, images obtained did not show passage of injectate into the epidural space. Finally, unless one uses contrast with the steroid injectate, there is no proof that the final injectate actually went into the epidural space.
It may be questioned why cases from 2003 were used rather than more current cases. In 2003 all these cases were pulled and analyzed. Due to change in personnel doing this research work, this project was never completed. The senior radiologic author has personally observed continued problems with persons claiming epidural blocks where no proof was evident in the fluoroscopic images. Therefore, the value of publishing this work is pertinent to cervical nerve blocks still being performed. Furthermore, the injection technique of the senior author had not changed in all these years, with the exception of a change in the type of steroids used and some alterations in the method of delivery of the injectate. Hence, this older collection of cases is still applicable in today's practice.
In this study, there was a statistically significant increase in central epidural flow when the needle tip on the true anteroposterior view was medial to the midline of the articular pillars (lateral masses) with a constant volume of injectate. This work also suggests that if one desires to perform a selective transforaminal cervical nerve block with little to no epidural flow, the needle tip should be kept lateral to the midline of the articular pillar. Even if the needle tip on the true frontal view was medial to the midline of the pillar or in zone 3, 16.2% of the injections did not demonstrate epidural flow. Therefore, digital subtraction fluoroscopy utilizing a small volume of dense myelographic contrast (Omnipaque 300) prior to steroid and local anesthetic mixture delivery is strongly recommended to eliminate the chance for intra-arterial administration and confirm central epidural flow (if desired). Digital subtraction fluoroscopy during placement of final injectate is also recommended to verify continued flow of injectate outside of vascular structures into the epidural space.
Reports of catastrophic complications in the literature and current procedural standards might sway a practitioner away from passing the needle medial to midline of the articular pillars.5,6, 7 , 8 , 9 , 10 However, it has previously been reported that there is no significant difference between the rates of catastrophic complications associated with zone 3 + 4 injections and zone 2 injections (frontal view). 2 The needle tip position on the lateral view seems less important with regards to central epidural flow. However, more anterior positioning of the needle tip as seen on lateral view images was associated with an increase in minor complications. 2
Obtaining a magnetic resonance or CT exam prior to performing a cervical nerve block is commonly done, and such an exam may show the rare case where a large lateral outpouching of the spinal sac in the potential site of needle placement may present a potential complication. However, as patients are referred from a variety of physicians in and outside of our institution, such exams are not always available for our review, and in an occasional case a magnetic resonance or CT study may have not been performed. This remains our approach to performing such blocks to current date.
Although during this study, a different steroid was used than in our current practice, the total volume of injectate has not changed. It is our current practice to follow suggestions in prior literature to use only water-soluble steroids rather than particulate steroids and to use subtraction imaging during both the test dose of contrast and the final injectate placement (1 mL of dexamethasone 10 mg/mL [dexamethasone sodium phosphate injection: Baxter Healthcare Corporation, Deerfield, Illinois, United States] plus 0.25 mL lidocaine 4% plus 0.25 mL Omnipaque 300 for a total volume of 1.5 mL). 3 Examples in the literature agree with what this article demonstrates as epidural flow of contrast. 3 ,4,5,6 However, we could find only one article where the authors added contrast to the final injectate to verify where the final flow of injectate spread. 3 Washout or disappearance of the initial test contrast may represent flow of final injectate into or outside of the epidural space, but, in the anecdotal experience of the senior radiologist author, such washout commonly may result from flow into vascular structures. Therefore, if a test contrast placement is satisfactory, later placement of final injected fluids may not always flow into the suspected and desired space. This may be due to slight needle tip movement during injections from the pressure of fluid passing through the needle, or from slight needle tip movement if one changes the syringe attached to that needle between the test and final injection.
We could find no articles relating needle tip position to the final position of injected fluids. Indeed, keeping the needle tip lateral to the midline of the pillar (our zones 1 and 2), as suggested by guidelines for performing fluoroscopically guided cervical nerve blocks,5 resulted in epidural flow in only 28.9% of injections in this study. The reason to keep the needle tip lateral to the midline of the articular pillars is to keep it away from the common position of the vertebral artery.5 However, by keeping the needle parallel to the anterior surface of the pillar and posterior to the vertebral artery, one can carefully pass the needle centrally, even to the medial edge of the articular pillar. The needle should always be lateral to the uncinate process to avoid the thecal sac.5 In some patients the medial border of the articular pillar will be in the same plane as the uncinate process. There was epidural spread of the injectate in 83.8% of our cases with the needle tip medial to the midsagittal plane of the articular pillar. But the only needle tip position that always resulted in epidural flow was at the medial edge of the articular pillar (zone 4). A contraindication to placing the needle tip centrally is the rare patient who has large lateral subarachnoid recesses or sacs as shown on magnetic resonance imaging.
The main weakness of this study is that a larger number of cases were not included. Only 7 of the 132 nerve blocks had the needle tip in zone 4; however, 100% of those 7 cases showed epidural flow. Many more cases (62 or 83.8%) had the needle tip medial to the midline of the pillar or in zone 3, which showed epidural flow. This work shows that needle placement lateral to the midplane of the articular pillar, the site supported by literature, commonly will not result in epidural spread of the injectate.5,6 Therefore, if epidural spread is desired, we feel that it is helpful to establish an ideal location that can be utilized in the majority of cases.
An additional shortcoming of this work is that outcomes of the blocks were not available. Although the large majority of the patients were referred from a single orthopedic spine surgeon, patients were referred from a variety of referring physicians who had no standard method of recording follow-up. Also, due to the retrospective nature of this study, standardized follow-up was not performed.
As mentioned in the introductory comments, some people may no longer perform CNRBs and foraminal epidurals under fluoroscopic control. However, in the anecdotal experience of the senior radiologic author, such blocks are still being performed with fluoroscopic control as well as with CT guidance. The main reason for using these cases from an older period of time is that the conclusions from studying these older cases are still applicable to blocks being performed today in many departments around the world. In our current practice, we do not use CT guidance for routine cervical nerve blocks. The current practice of performing cervical nerve blocks by radiologists in our department is to use the method described by Schellhas et al, 4 as it has seemed to be less technically demanding than the technique used by the senior radiologic author in this article. However, we feel that the addition of contrast to the final injectate is valuable to verify the distribution of the injectate.
The information in this article is currently clinically relevant in that it identifies a needle tip location that maximizes the likelihood of passing injected material epidurally from a transforaminal approach. If epidural flow is desired, one can identify the ideal position for each individual patient by doing repeated fluoroscopically monitored contrast injections and continued further medial tip placements. However, that practice will increase the amount of radiation for both the patient and the injectionist. Injecting material from a position lateral to the midplane of the articular pillars provided epidural flow in only 28.9% of injections. Our data suggest that to insure epidural spread in 100% of the cases, one has to place the needle in zone 4, the most medial zone. We recommend starting with the needle tip medial to the midplane of the articular pillar (zone 3), because that resulted in epidural flow in 83.8% of cases. This has the potential to result in decreased radiation exposure, as well as the frequency with which one would need to pass the needle into zone 4 to get epidural flow. Although we did not observe any complications in the seven cases that we examined, this is a small number. Although intuitively it is clear that the risk of complications could potentially be increased with a more medially placed needle tip, that was not the situation in one published study that analyzed 1,036 cervical blocks. 2 It is our firm belief that placement of a needle tip centrally has to be performed with care, keeping the needle posterior and parallel to the anterior surface of the articular pillar. If there is no desire or need to place injectate into the epidural space, the needle tip can be placed anywhere lateral to zone 4. However, one should not state that a foraminal epidural block has been performed unless injectate can actually be seen in the epidural space. Nevertheless, to be sure that the injectate reaches the offending pathology, and if an epidural effect is desired, the needle may need to be placed close to or in zone 4.
In conclusion, having the needle tip near or at the medial border of the pillar maximizes the likelihood of obtaining intraforaminal epidural flow of the injected material. One should not state that an epidural block has been performed unless injectate is demonstrated in the epidural space. Finally, it is our strong belief that only by using contrast material mixed with the final injectate can one more objectively prove the extent of the injectate flow, as opposed to merely watching the washout of the contrast material placed in the test injection.
Disclosures
None
Footnotes
Acknowledgment
We express our appreciation to Daniel Ma, MD, and Thomas Pilgram for their help with this work.