
Abstract
Study Design:
Narrative review.
Objective:
To establish recommendations for the treatment of odontoid fractures based on current literature and the knowledge of the experts of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU).
Methods:
Narrative review of the literature. Analyzing treatment algorithms of German trauma and spine centers as members of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU).
Results:
There are many influencing factors leading to appropriate treatment of odontoid fractures such as age, bone quality, arthrosis, classification, and type of the fracture. Conservative nonoperative treatment is appropriate for stable undislocated displaced odontoid fractures. Anterior osteosynthesis with 1 or 2 screws leads to good results in the classical unstable type II odontoid fracture in patients with good bone quality. However, modifiers have been identified by the working group leading to higher complication and failure rates. For these cases, more stable constructs and/or posterior approaches are indicated.
Conclusions:
Operation seems to be standard treatment for odontoid fractures. However, in the aged population, conservative treatment should be considered as morbidity and mortality rise significantly in the group of >75 years. Conservative treatment may also be started within stable nondislocated fractures, but then regular controls have to be performed. If operation is indicated, many influencing factors have to be considered for appropriate approach and technique. The classification of Anderson and D’Alonzo is still standard. To create an adequate treatment algorithm, dislocation displacement and instability have to be identified. Stable odontoid fractures are treated conservatively non-operatively, but if so regular controls have to be performed. Unstable and/or dislocated displaced odontoid fractures are treated by anterior osteosynthesis with 1 or 2 screws. The technique is demanding and leads to elevated complication and failure rates if modifiers are apparent. In these cases, posterior instrumentation or fusion of C1 and C2 is favorable. In the aged population (>80 years), operative therapy is critical as postoperative morbidity complication and mortality rates rise significantly. As there is still some bias in the treatment algorithms, the working group recommends establishment of a prospective study to result in more objective statements.
Keywords
Introduction
Odontoid fractures are widely common and reported to account for up to 15% of all cervical spine injuries. 1 In the elderly population, this fracture type represents the most common cervical spine fracture and in the population older than 80 years, the most common spine fracture of all. 2 This fracture type is potentially serious due to the proximity of the medulla oblongata and the great mobility of the cranial-cervical junction resulting in a high risk of life-threatening neurological lesions. Injury treatment aims to reestablish stability of the atlanto-axial complex. Management options for odontoid fractures have expanded with advantages in imaging and surgical technologies, with a trend toward primary operative stabilization. 3 Initially strong indications with fracture displacement >5 mm, angulation >10°, and the presence of neurological deficits are widened also considering the potentially high morbidity, instability and secondary displacement in conservatively treated patients. 1,4 However, even operation results in nonunion rates of up to 33%. 5,6 In a recently published meta-analysis, posterior C1/2 fusion resulted in significantly higher fusion rates in the elderly. 3 In younger patients, the potential loss of C1/2 motion should be taken into account, thus anterior direct osteosynthesis or temporary posterior stabilization using Harms technique are better options in this patient group. Despite numerous published articles over the past 2 decades. The optimal treatment remains controversial as there are many contributing factors. The Spine Section of the German Society for Orthopaedics and Trauma (Deutsche Gesellschaft für Orthopädie und Unfallchirurgie, DGOU) has set up a working group to analyze strategies in German trauma and spine centers and is going to publish recommendations on the treatment of odontoid fractures.
Diagnostics
Patients history and clinical examination is documented by using a structured protocol, neurological deficits have to be documented using the scoresheets of the American Spinal Cord Injury Association (ASIA, http://asia-spinalinjury.org). Canadian C-Spine rules are recommended due to their high sensitivity. 7 With a detailed history and physical examination patients in the low-risk group can be cleared without further radiographic examinations. Conventional X-rays in 2 planes in combination with a special transoral view are still standard diagnostics for patients in the “low-risk” group with a suspected cervical spine injury after blunt trauma. Multislice computed tomographic (CT) scans with multidirectional reconstructions have to be performed in the “high-risk” group as it allows to evaluate fracture type and to assess the degree of instability in polytraumatized patients and after high-energy trauma. Flexion-extension X-rays guided by hand may give more information about potential instability. Magnetic resonance imaging (MRI) can give information about age of the fractures, ligamentous injuries, and status of the myelon. 8
Classification
Odontoid fractures have been divided into 3 major types according to the classification of Anderson and D’Alonzo. 9 Type I is an avulsion of the odontoid tip by the alar ligaments and is very rare. Type II occurs at the base of the odontoid process and represents the most common fracture type. Type III extends into the body of the axis and has good healing potential.
Type II fractures may show different directions of the fracture line and are classified by Eysel: horizontal (type A) and anterosuperior to posteroinferior (type B) direction is favorable for anterior screw osteosynthesis, whereas reverse fracture lines (type C) represent contraindications for anterior screw osteosynthesis. 10
Treatment Options
Collars and Halo Fixators
The use of collars and halo fixators remains controversial. Soft collars have no stabilizing function, thus we do not recommend them in the early phase. However, they may be used for nonoperative treatment in stable fractures after an initial phase with a hard collar. Hard collars (Philadelphia, for example) may be used in the first phase for unstable fractures until a decision for further treatment is made. It may be used for 6 to 8 weeks in cases where nonoperative treatment is indicated. Halo fixators are highly controversial as they are found to aggravate mortality and morbidity especially in the elderly patients mainly due to soft tissue and handling problems. It may serve in some case as rescue tool in the acute phase before decision about definitive treatment is made. 11 -15
Anterior Odontoid Screw Fixation
Initially described by Böhler, 16 osteosynthesis with 1 or 2 screws by an anterior approach is standard operative treatment in younger patients with good bone quality if adverse modifiers are absent (Table 2). Patients are operated on in supine position. With a minimal open incision, the preparation follows the anatomical structures for standard anterior approach to the cervical spine. Special cannulated systems may be used to protect soft tissues. A crucial step is the reduction of the fracture and maintaining the reduced position, for example, by using a Mayfield clamp. Positioning of guide wires is controlled by 2 C-arms (anteroposterior and lateral). Alternatively, carbon halo ring allows optimal reduction, which can be controlled by intraoperative 3-dimensional scan as well as the positioning of the guide-wires and the screws, respectively. While positioning the screws over the guide-wire X-ray control is crucial as guide-wire migration toward the medulla oblongata has absolutely to be avoided. 6 There is no clear evidence whether to use 1 or 2 screws. 17,18 The important detail is to reach the cortical bone on the odontoid tip to result in fracture compression. Cannulated partial threaded screws are preferred, double threaded screws show similar good results. We recommend using 2 screws (3.5-mm diameter) to secure rotational stability, especially in the elderly patients while 1 screw (4.5-mm diameter) is mostly sufficient in young patients with good bone quality. To assure better screw purchase even in osteoporotic bone the screws can be augmented with PMMA (polymethyl methacrylate). However, the number of treated patients is currently small and long-term outcome is unclear. 19,20
Anterior Transarticular C1/2 Stabilization
This technique may be used in elderly patients to secure reduction by transarticular stabilization of C1/2 if posterior approach is impossible and is regularly combined with odontoid screw(s). 21 Crucial part of this operative technique is the entry point and positioning of the screws from C2 onto C1 via the classical anterior approach. As in the posterior technique, the vertebral artery anatomy has to be analyzed in advance.
Posterior Transarticular C1/2 Stabilization and Fusion
First described by Jeanneret and Magerl, 22 the classical posterior fusion technique with bone graft is performed by open approach. This technique may be modified into a percutaneous cannulated posterior C1/2 stabilization. The crucial step is the reduction of the fracture and the positioning of the patient to maintain correct reduction. Care must be taken not to harm the vertebral artery as there is a large variety and the anatomical space for the screws is absolutely limited. 23,24 Preoperative CT scans or intraoperative 3-dimensional control is therefore mandatory. The percutaneous technique has been shown to reduce approach morbidity and to be safe for elderly patients. The open technique is accompanied by higher fusion rates but also by higher approach related morbidity especially in the elderly population. 12,25
Posterior Instrumentation (Harms/Goel)
C1/2 internal fixation by placing C1 lateral mass screws and C2 pedicle screws according to Harms/Goel is a valuable alternative to the Magerl technique. This technique was first described by Goel and Laheri 26 and allows good fracture reduction. It is the preferred method in cases where the Magerl technique is not possible and if one aims for a temporary stabilization. However, it is demanding, with the need of open approach in an anatomically complex region. The technique has been modified by Harms and Melcher 27 using polyaxial screw/rod systems.
Posterior Occipito-Cervical Stabilization and Fusion (C0-C3/4)
The presence of ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis (DISH), or complex injuries may alter the treatment algorithm and a C1/2 stabilization alone may be insufficient. In these cases, an occipito-cervical stabilization and fusion should be performed.
Specific Age-Related Conditions
In the younger population, odontoid fractures are usually the result of high-energy trauma (traffic accident, fall from height) whereas in the elderly, low-energy trauma is the major reason. Sometimes even no trauma is reported by the elderly patients and the fracture might be older. Osteoporosis, arthrosis of the C1/2 joints, and general condition of the patients are important modifiers especially in the elderly population for the treatment indication. Furthermore, high complication and mortality rates are reported in the elderly. 28
Nonunions
One major aim in the treatment of odontoid fractures is bony healing. However, some authors report on fibrous union with radiological stability to be considered as acceptable if not good outcome in the elderly population. 29 This type of nonunion has to be differentiated from atrophic and hypertrophic types associated with sclerosis, resorption, and cyst formation as well as poor outcome results. 30
Mortality in the Elderly Population
In geriatric trauma, the relationship between injury severity, comorbidities, and mortality is well studied. Early operative intervention to stabilize odontoid fractures in the elderly using appropriate stabilization techniques has been reported to substantially decrease mortality. However, in the population older than 75 years, this effect was not significant and in the patients ≥85 years, 3-month and 1-year mortality was reported to be higher in the operative group compared with conservative treatment. 2,30,31
Factors Influencing Treatment Indication
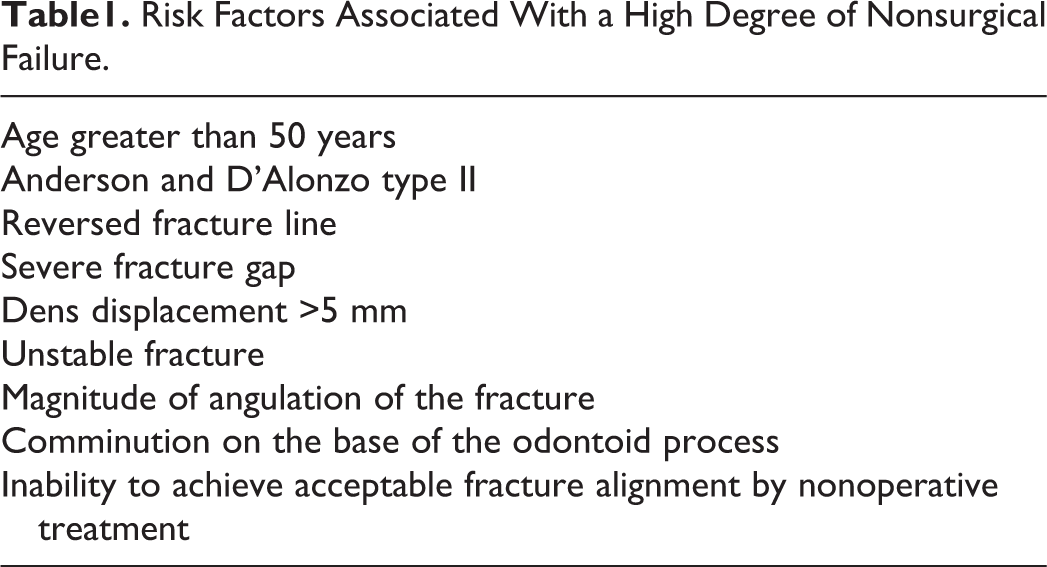
Fracture patterns and alignment are important in determining surgical compared with non-surgical treatment. Anderson-D’Alonzo type I as well as nondisplaced and stable type II and III fractures may be treated nonoperatively. For unstable and displaced fractures, high rates of nonunion and treatment failures are reported in case of conservative and inappropriate operative therapy. The risk factors associated with a high degree of nonsurgical failure are summarized in Table 1. Even for operative treatment, high nonunion rates are reported in the literature. Analyzing the possible reasons for surgical failure, inappropriate indications may be deteriorating. 3,4,13,30,32 -36
Risk Factors Associated With a High Degree of Nonsurgical Failure.
Treatment Algorithm
First step in the treatment algorithm (Figure 1) is the classification according to Anderson and D’Alonzo. Type I is exceptionally rare and can be treated nonoperatively using a hard collar for 6 to 8 weeks. However, this type may represent the avulsion fracture of the odontoid from atlanto-occipital dislocation and therefore be handled with care. Types II and III have to be analyzed according to the criteria instability and displacement. If one of the criteria is fulfilled, operative treatment is indicated and further analysis concerning modifiers has to be performed. For nondisplaced fractures, stability has to be tested using dynamic X-ray. Nondisplaced fractures without signs of instability can be treated nonoperatively using hard collar for 6 to 8 weeks.
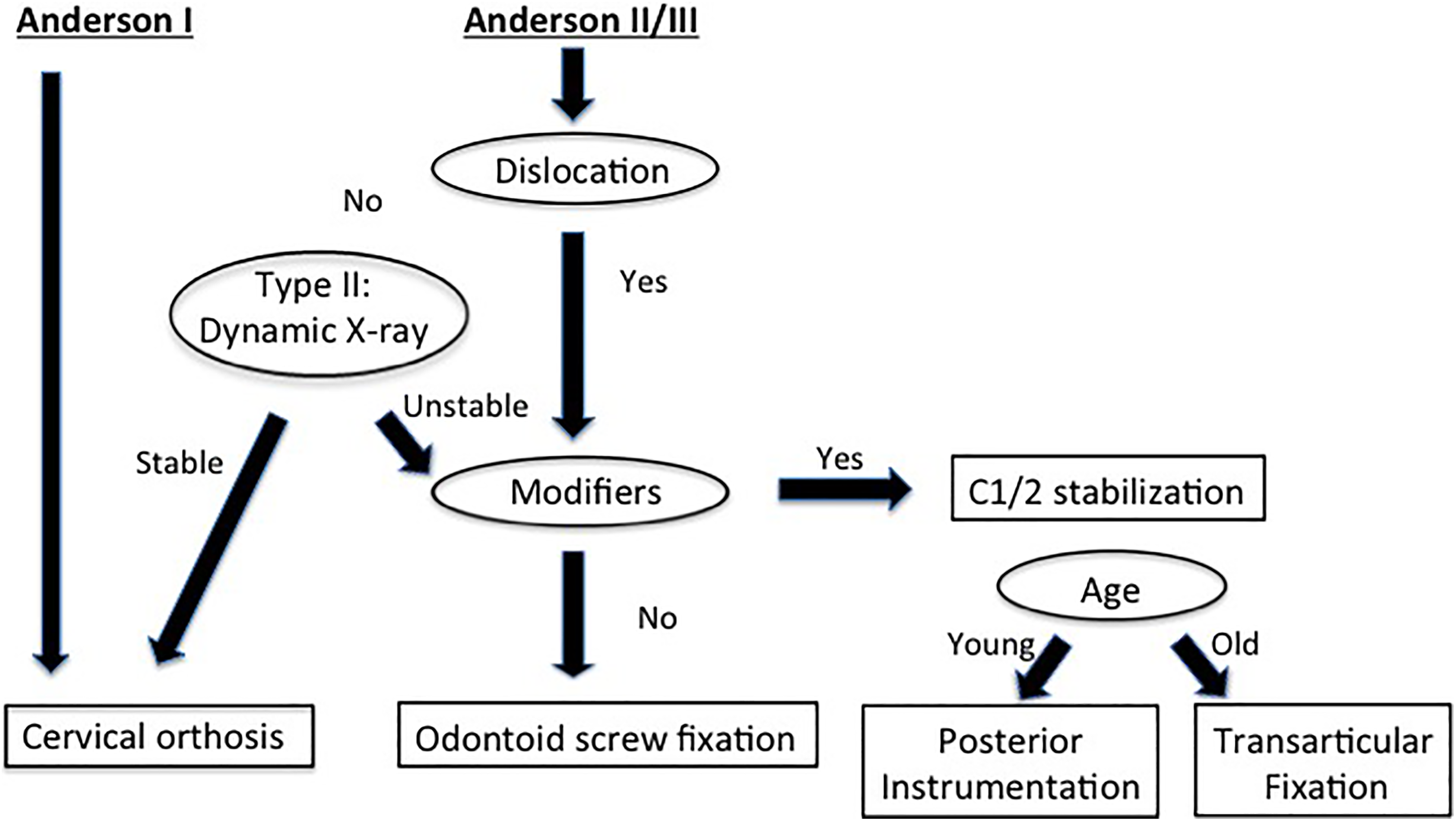
Algorithm for the treatment of odontoid fractures.
Once operative treatment is indicated, approach and technique have to be determined. Young patients with good bone quality are treated with direct osteosynthesis using anterior screw
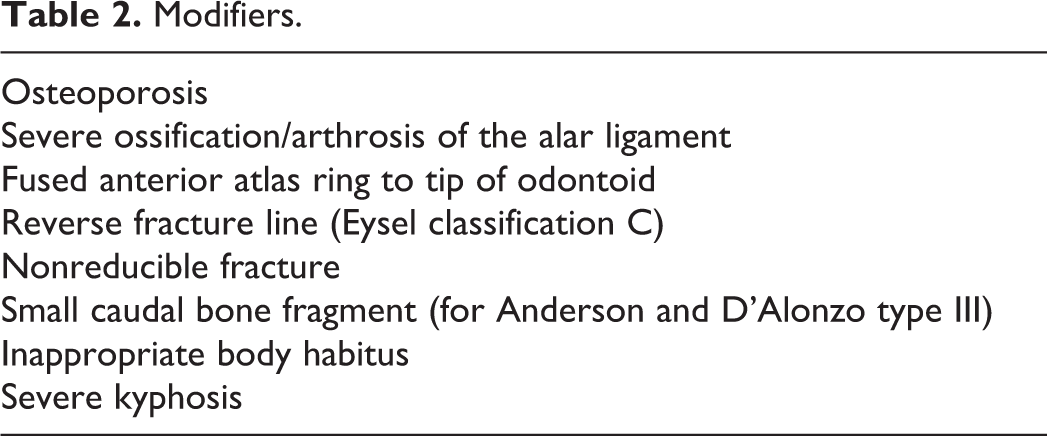
If one or more modifiers (Table 2) are present, posterior stabilization is the first choice. In younger patients, fusion and deterioration of the atlanto-axial joints should be avoided by using the temporary stabilization described by Harms and Goel. Implants can be removed after bony healing. In the elderly, C1/C2 stabilization with or without bone graft should be performed.
Modifiers.
Craniocervical fixation (C0-C3/4) is only indicated if anatomical variations or bad bone quality does not allow secure fixation of the C1/2 screws. Another reason may be the long lever arm below C2 because of fused segments, for example, ankylosing spondylitis.
Conclusion
Odontoid fractures are widely common. However, the optimal treatment remains controversial as there are many contributing factors. The Spine Section of the German Society for Orthopaedics and Trauma (Deutsche Gesellschaft für Orthopädie und Unfallchirurgie, DGOU) has set up a working group to analyze strategies in German trauma and spine centers. The resulting recommendations are the result of a narrative review of the literature, the analysis of a retrospective study in the participating trauma and spine centers and regular meetings of the working group. Operation is the standard treatment for unstable and displaced odontoid fractures and results in good outcome for correct indications and if adequate technique and approach is used. In the aged population, nonoperative treatment should be considered as morbidity and mortality rise significantly in the group of >75 years. However, the working group realized that there is still some bias in the treatment algorithms. Therefore, the final recommendation is to establish a prospective study to result in more objective statements.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.