
Abstract
We report a case of bilateral three-level lumbar spondylolysis that was directly repaired by use of hook-screw technique. The patient complained of low back pain for 2 years that progressively worsened and was exacerbated with standing and walking. He also mentioned bilateral sciatalgia. The neurological examination was normal. Interestingly, we found bilateral lumbar spondylolysis in L3, L4, and L5 levels in imaging studies. After proving that spondylolysis was the source of the low back pain by local anesthetic agent injection, we used a direct technique for correction of spondylolysis by use of a hook-screw device plus decortications of lysis area and iliac crest autograft. We assessed the patient after surgery to evaluate pain recovery and fusion rate. The results were favorable and proved the efficacy of the hook-screw technique for treatment of symptomatic multilevel lumbar spondylolysis.
Lumbar spondylolysis is a bony defect in the pars interarticularis of the spine. It occurs in ~6% of the population and has been reported more commonly in men. 1 It occurs frequently in L5 pars interarticularis and can be unilateral or bilateral. Only a few cases of multilevel spondylolysis and its treatment have been reported in the literature.2–7 The origin of the pain could be in the tissues rich in nociceptive nerve endings in the looser posterior arch. Extra load exerted on the adjacent levels may cause disc degeneration, which is therefore an accompanying disorder of spondylolysis. 8 Most patients respond well to conservative treatment, although some need surgical intervention.
There are three techniques to correct pars interarticularis defects: decompression, arthrodesis, and direct repair. 9 Decompression has been the main approach for years, but it has a great disadvantage of overload on adjacent levels. The latter was introduced in 1968, and outcome has been appreciable in most cases without disc degeneration. 1 , 10 , 11 Because of defective tissue removal and fusion of pars defect, it seems a logically acceptable treatment at first glance. Young active adults are the main candidates for such a procedure. It may prevent back ligamentous and muscle injuries due to routine exposure for posterolateral fusion. The patient presented in this article is a very rare case of multilevel bilateral spondylolysis treated by a hook-screw technique, which has not reported so far.
Case Report
A 21-year-old man was referred to us with a 1-year history of low back pain. The pain evolved insidiously and progressed over time and was incompatible with comfortable everyday life. The pain was worse in the standing position and with flexion and extension and less in sitting and supine status. He did not complain of any constitutional symptoms. He remarked on bilateral back of thigh pain without radicular characteristics since 1 year previously. Physical examination revealed no significant finding. In lumbar spine X-ray examination and computed tomography scans, we found bilateral multilevel (L3, L4, L5) spondylolysis without any slip or scoliosis (Fig. 1). Magnetic resonance imaging showed no sign of slip or disc degeneration in the affected area (Fig. 2). A 3-month course of conservative treatment with nonsteroidal anti-inflammatory drugs was suggested, along with physical therapy and lumbar soft corset. The patient was symptomless after treatment, but 4 months later he again complained of a similar problem. The pain became more and more severe so that conventional conservative therapy had minimal effect and even referral to pain clinics and injection of anesthetics were unsuccessful in achieving acceptable and permanent results. The severity of pain disabled the patient. To prove the origin of the pain, with the guidance of fluoroscopy, local anesthesia (i.e., lidocaine and bupivacaine) was injected around all pars interarticularis defects. Again, the pain was relieved for 2 days, which reinforced the theory that the source of patient's pain was the spondylolysis. We were encouraged to perform a less invasive surgical technique for correction of defects.

Preoperative plain X-ray showing three-level bilateral spondylolysis: right oblique (A), lateral (B), flexion (C), and extension (D) views.

Preoperative T2-weighted sagittal magnetic resonance imaging showing no sign of slip or disc degeneration.
We used a conventional posterior midline approach to the lumbar spine. Paraspinal muscles were dissected subperiosteally and detached from the spinous process and vertebral lamina. This approach seemed to be wise because the instruments extended lateral to medial and a wide three-level exposure was necessary. A 6.5 × 45-mm multiaxial pedicle screw (USS-2 synthesis system) was inserted for the involved vertebrae under fluoroscopic guidance. Afterward, we performed decortication at the spondylolysis area to facilitate fusion. Then, we put a sublaminar hook in place and connected these two by a short appropriate rod (Fig. 2). Then, we interpositioned the iliac crest bone graft pieces between the two edges of lytic defects to facilitate fusion, and we tightened the nuts under compression. We used caution in order not to derange the apophyseal joint capsules. The total time of surgery was 3.5 hours with ~75 mL of blood loss.
Postoperatively, the patient remained neurologically intact and was allowed to sit and walk the day after surgery. He was discharged home 3 days after surgery with a lumbosacral brace. He was pain-free 6 weeks after the procedure and discontinued using the brace. He started physical therapy to strengthen the paraspinal muscular support. After a follow-up period of 2 years, there were signs of bony consolidation in five of all lytic defects (Fig. 3), and the patient was still pain-free.
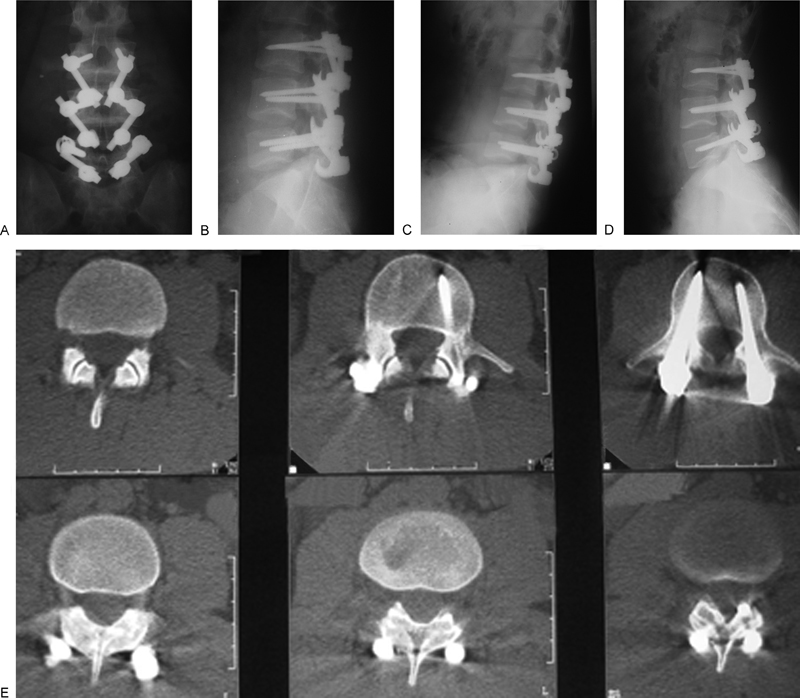
Postoperative plain X-ray about 2 years after surgery showing anteroposterior (A), lateral (B), flexion (C), and extension (D) views, and computed tomography scan (E).
Discussion
Pars defects are not uncommon and commonly present with low back pain, which usually could be managed conservatively. 12 , 13 When the source of the pain is the pars defect itself and hypermobility of the posterior column, direct repair of spondylolysis seems to be most effective and appears to be more logical than posterior spinal fusion to treat this disease in a small group of patients without disc degeneration or slip. This is the only truly reconstructive procedure in the spine. However, several reconstructive methods have been introduced. In 1968, Kimura 14 only used bone graft and prescribed a cast and long rest for fusion. In 1970, Buck 1 used a screw across the pars, and Nicol and Scott 15 used a wire surrounding lamina. In 1970, Louis 16 described a butterfly-shaped plate for temporary lumbosacral fixation. Morscher et al 17 created a screw-hook system that made it possible to repair the posterior arch and the bone graft under compression without the need for extensive dissection. This method required a special technique and, because of the weak instrument, needed a long-lasting brace. Recently, Songer and Rovin 18 used a sublaminar cable with the aid of pedicle screw. Pedicle screw direct repair confers immediate stability to the lumbar spine with a combination of autologous bone graft to provide better fusion. Existence of signs of disc degeneration or spondylolisthesis in imaging studies is a contraindication of this strategy. Because there is no overload on neighboring levels, there would be no degeneration of an adjacent level.
The complication rates due to various surgical technique or hardware failure have been reported to be 5.6 to 40% with Buck's technique, 14% with Scott's technique, and 44% with Morscher's technique. 3 , 12 Good to excellent clinical results were obtained in 60 to 90% of patients with Buck's operation, 80 to 90% with Scott's wiring technique, 75 to 90% with Morscher's hook-screw system, and 81 to 100% in the segmental pedicle hook-screw system. 10
The new technique that is described by Kakiuchi 13 and offered here appears to have some advantages. First, the strength of system (screw and hook) avoids the need for postoperational immobilization, and the patient can return to daily activities soon after surgery. Deguchi et al 12 demonstrated biomechanically that such a construct minimizes micromotion across the defect. Second, almost all surgeons are familiar with the principles of this technique. Third, bone grafting is not hindered by the hardware, and compression of the graft against the pars defect is easily possible. Fourth, hardware removal is not obligatory, because all adjacent segments remain free and no loss of segmental motion occurs as with fusion procedures. Fifth, the risk of adjacent-level disc degeneration diminishes by keeping the segmental motion. 3
However, by open placement of such a system, collateral damage of soft tissue may occur. 9 , 19 Various surgeons have searched for less invasive muscle-splitting lumbar techniques to reduce paraspinal tissues damage. Roca et al 10 concluded that pars direct repair is not suitable in patients older than 20 years old because of a low fusion rate. However, some authors reported good results in patients between 20 and 30 years of age. 20 Szypryt et al 21 showed that spondylolysis in patients older than 25 years is associated with more disc degeneration relative to the normal population. Indeed, the most common reason for pars direct repair was disc degeneration. Almost all authors agree that disc or facet degenerative changes are contraindications for direct pars repair. 10 , 14 , 22 If abnormal disc signal is detected in magnetic resonance images, arthrodesis should be considered instead of repair.
Our case was unique in that there were six spontaneous pars defects as three adjacent-level bilateral spondylolysis. We could not find any similar case of multilevel spondylolysis repaired by a hook-screw system so far. Although a 2-year period of follow-up sounds short for achieving convincing results, it was convenient for finding signs of bony consolidation in direct repair places. We can leave the instruments in place because flexion-extension images are satisfactory and motion of the spine is well preserved and the patient is obviously pain-free.
In conclusion, direct repair of pars interarticularis in multilevel spondylolysis by a hook-screw system appears to be an appropriate technique and superior to other treatment modalities.
Disclosures
Guive Sharifi, None
Amin Jahanbakhshi, None
Behnam Daneshpajouh, None
Abolfazl Rahimizadeh, None