
Abstract
The aims of the present study were to evaluate the prevalence of headache and the frequency of different headache syndromes in patients with Behçet's Disease (BD) without neurological involvement and to investigate the relationship with other clinical, and behavioural variables. Twenty-seven BD patients and 27 control subjects underwent a validated semistructured questionnaire based on the International Headache Society criteria. Levels of anxiety and depression, disease activity, and current medication were collected. Headache occurred in 88.9% of BD patients. There was no difference in the prevalence of the different headache syndromes between BD patients and controls. Only migraine without aura (MwA) was significantly more frequent in BD patients than controls (44.4% vs. 11.1%, respectively, P = 0.013). No relationship was found between MwA and clinical, and behavioural variables. Among headache syndromes, MwA showed the highest frequency in BD. A vascular or neuronal subclinical dysfunction could justify this association. A careful interview for migraine might be included in the diagnostic work-up of BD.
Introduction
Behçet's disease (BD) is a multisystem vasculitis, characterized by the clinical triad of recurrent oral and genital ulcerations and recurrent uveitis (1). The major causes of disability comprised ocular, vascular and neurological involvement (neuro-Behçet) (1, 2).
Headache has been described in BD patients with or without neurological involvement (3–5). However, as far as we know, no systematic data have been reported; furthermore, the exact prevalence of headaches in BD is still unknown. Previous studies reported a headache prevalence ranging from 8 to 70%(3–5). This variability can be explained mainly in terms of criteria used to define headache type. Moreover, previous studies have failed to rely on the current International Headache Society (IHS) criteria for headache syndromes.
The aim of this study was to assess the prevalence of headache syndromes in a group of BD patients without overt neurological involvement using a questionnaire based on the IHS criteria. In addition, we examined the relationship between headache type and clinical variables (disease duration, disease activity, current medication), and anxiety and depression levels.
Methods
Twenty-seven consecutive BD outpatients (14 male, 13 female; mean age ± sd 33.2 ± 8.6), fulfilling the criteria of the International Study Group for Behçet Disease (6), were studied. Age at onset of disease ranged from 10 to 45 years with a mean of 27.2 ± 8.4. Disease duration (in months), defined as the interval between the time of onset of symptoms attributable to BD and the time of assessment, ranged from 12 to 300 months with a mean of 72.8 ± 62.9. For each patient, disease activity was assessed by using the BD Current Activity Form (BDCAF) (7), a standardized index scoring major clinical features of the disease in the month preceding the examination according to the duration of symptoms. Patients reported a mean BDCAF score of 7.2 ± 5.0 (range 0–18); current clinical features included arthritis or arthralgia (44.4%), fatigue (40.7%), oral aphtae (33.3%), gastrointestinal involvement (22.2%), genital ulcerations (18.5%), skin lesions (18.5%) and uveitis (3.7%). Detailed information on current medications was collected for each patient. Sixty-seven percent of BD patients were receiving prednisone, 56% colchicine, 22% cyclosporin A, 11% ciclophosphamide and 4% nonsteroidal anti-inflammatory drugs. For each patient, previous history did not reveal symptoms of neurological involvement, and neurological examination was normal as well as brain CT scan.
Twenty-seven healthy subjects matched for age and gender (14 male, 13 female; mean age ± sd 33.4 ± 9.1), drawn from the hospital staff and without any known medical or surgical problems, were used as controls. All participants gave their informed consent to the study.
Patients and controls were administered a semistructured questionnaire for headache, based on IHS criteria, previously used for epidemiological purposes (8). It included questions about age of onset of headache, frequency, duration, severity, and accompanying symptoms. Frequency of attacks was coded as follows:
(a) several times a week;
(b) about once a week;
(c) about once a month or less than once a week;
(d) several times a year.
Duration of attacks was measured in hours. Severity of headache attacks was classified as:
(1) mild (not affecting daily life activities);
(2) moderate (reducing daily life activities);
(3) severe (requiring bed rest).
Patients were also asked about migraine family history.
To assess levels of depression and anxiety, patients and controls were evaluated with two self-rating psychological scales, the Zung Anxiety (ZA) (9) and Depression (ZD) (10) scales.
Student t-test and χ2 test were used for comparison of quantitative and qualitative data, respectively. Multiple regression analyses, controlling for age and gender, were conducted to evaluate the possible relationship between headache and BDCAF score, and anxiety and depression levels. Differences were considered significant when P≤ 0.05.
Results
As shown in Table 1, headache was more common in BD than in controls, although this difference approached statistical significance (Fisher's exact two-tailed test P= 0.054).
Prevalence of headache syndromes in patients with Behçet's disease and in controls
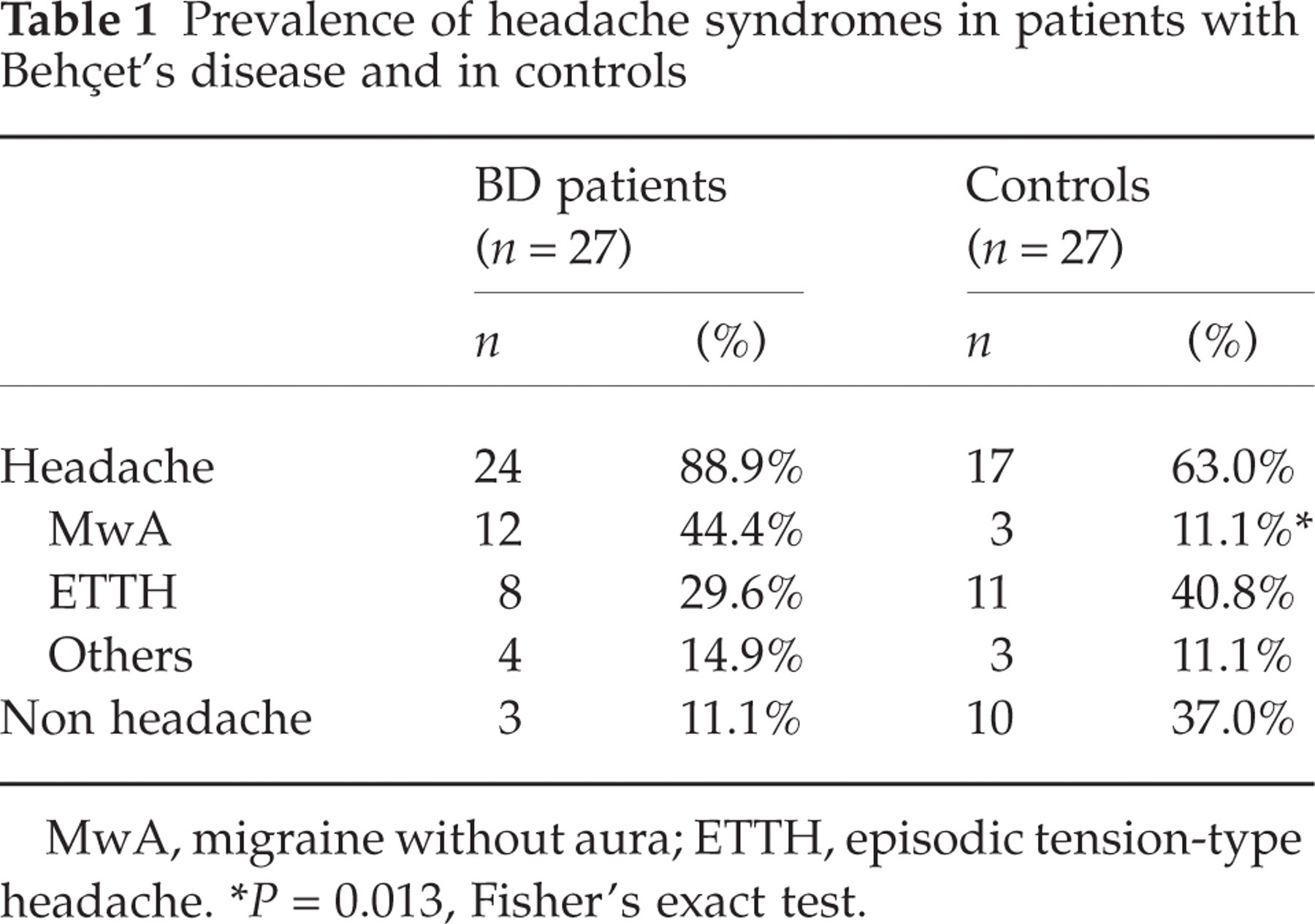
MwA, migraine without aura; ETTH, episodic tension-type headache.
∗ P= 0.013, Fisher's exact test.
Basing on IHS criteria, subjects were divided into 4 groups: migraine without aura (MwA, IHS 1.1), episodic tension-type headache (ETTH, IHS 2.1), other headaches, and headache free (Table 1). There were no differences between patients and controls in the frequency of ETTH and other headaches (3 patients had migraineous disorder (IHS 1.7), and one patient reported headache as probable side-effect of cyclosporin). Concerning MwA, its prevalence in BD was significantly higher than in controls (Fisher's exact two-tailed test P= 0.013).
The age of onset of headache was similar in BD patients (23.8 ± 7.4, range 12–43) and controls (23.6 ± 9.3, range 10–43).
The onset of MwA attacks was before the onset of BD in 4, and 1 years after the onset of the syndrome in 2 patients. In the remaining 6 patients, MwA began with the onset of BD (i.e. within three months of the disease onset).
A family history of migraine was evident in 50% (6/12) of BD patients and in 100% (3/3) of controls, although this difference was not statistically significant.
Concerning behavioural measures, significant differences between patients and controls were found on the ZA (mean ± sd of 36.4 ± 10.3 vs. 26.6 ± 6.3, respectively, t = 4.63, P < 0.0001) and on ZD (33.4 ± 9.6 vs. 25.7 ± 4.6, respectively, t = 3.8, P < 0.0004).
Due to the fact that among different headache syndromes only migraine prevalence was significantly different between patients and controls, regression analysis was conducted only in migraineurs. After regression analyses, no relationship was found between both migraine diagnosis and characteristics of migraineous attacks (frequency, duration, and severity) and disease duration, BDCAF, ZA and ZD scores, and types of medication used.
Discussion
In a group of 27 patients with BD without overt neurological involvement, we found a headache prevalence of 88.9%. However, compared with controls the frequency of headache was not significantly different, even approaching statistical significance. Concerning headaches distribution, only MwA resulted significantly more frequent in patients than in controls.
We are aware of only three others studies reporting data about headache prevalence in BD (3–5). Wechsler et al. (4) found a prevalence of about 22% in 31 BD patients. In a cohort of 46 BD subjects referred for neurological examination to their department, Serdaroglu et al. (3). described a prevalence of headache of about 56%, of which about 37% with migraineous headache. A recent study of the same Turkish group (5) reported a similar prevalence (63%) of headache, 30% of which with migraine-like headache. We found a higher prevalence of headache than previously reported. This difference could be attributed to the nature of previous studies, not designed to evaluate headache prevalence in BD but mainly focused on features of neurological involvement in BD. For this reason, none used IHS criteria for headache, or adopted a control group. In the present study, we adopted IHS criteria for headache, used a control group matched for age and gender, and controlled for several demographical, clinical and behavioural variables.
We found a very high prevalence of MwA in BD. Three evidences suggest a possible relationship between migraine occurrence and BD presence. Firstly, in the most of BD patients MwA onset was closely related to disease onset. In fact, 66.7% of patients developed migraine at the same time of BD onset or 1 years after the appearance of disease symptoms. However, both patients and controls reported similar age of onset of headache attacks, thus not excluding that migraine and BD share common ages of onset. Secondly, only in 50% of BD patients with MwA there was a positive family history for migraine while it was present in all migraineurs controls, thus probably excluding a genetic predisposition for migraine onset in BD, even if this sample (n = 3) was too small to draw firm conclusions. Lastly, we found no association between migraine and its characteristics and disease duration, disease activity, and current medication, all factors that might act to precipitate migraine in susceptible individuals. Similarly, even if BD patients showed significant high levels of anxiety and depression, probably reflecting the psychological stress of a painful chronic illness such as BD, the presence of these disturbances did not relate with migraine presence.
The pathogenesis of migraine in BD is open to discussion. It has been suggested that small vessels disease, characterizing several multisystemic vasculitis, such as systemic lupus erythematosus, Sjogren's syndrome, scleroderma but also BD, may cause cerebrovascular dysregulation, leading to migraine (11). However, we did not find any relationship between disease activity and the frequency, duration, and severity of migraineous attacks. The lack of this association could be attributed to the cross-sectional design of the study. In fact, a longitudinal evaluation might allow us to relate the fluctuations in disease activity, typical of a relapsing-remitting disease as BD, with the characteristics of headache attacks.
An alternative intriguing hypothesis could rely on anatomo-radiological data. It is well known that the most common region involved in BD is the brainstem (2), a subcortical area recently proposed as the ‘migraine generator’ (12). The finding of a subclinical cortico-subcortical involvement in BD patients without neurological symptoms and signs, as recently described by a functional neuroimaging study (13), could support this hypothesis.
Despite the rigorous methodological approach, our study deserves a number of shortcomings. The cross-sectional nature of our study, the lack of a brain MRI examination, and the limited number of patients included make it difficult to draw definite conclusions from our data.
In conclusion, the present study shows that 88.9% of BD patients complained headaches; of these, 50% suffered from MwA. The high frequency of migraine cannot be explained in terms of demographical, clinical, and behavioural variables, probably accounting for a vascular or neuronal subclinical dysfunction. In this view, as previously evidenced by clinical and neuroimaging reports (13, 14), migraine as the first neurological symptom of BD could herald neurological involvement. We suggest to include a careful interview for migraine in the diagnostic work-up of BD. Neuroimaging and longitudinal data are necessary to confirm this issue.
Footnotes
Acknowledgements
This study was supported in part by a MIUR grant to R. Camarda. Most of all our thanks go to the patients and controls.