
Abstract
This study of sleep changes in patients with cluster headache (CH) was conducted in view of the nocturnal predominance of this condition, the efficacy of oxygen and the fact that the attacks follow oxygen desaturation. Proposed mechanisms include impairment of carotid body activity secondary to hypothalamic vasomotor regulatory dysfunction. Sixteen patients with episodic CH and 29 healthy volunteers underwent nocturnal polysomnography. Five (31.3%) patients with episodic CH were found to have sleep apnoea (SA). Two patients with SA experienced two attacks during the study period. The attacks followed episodes of oxygen desaturation and were associated with REM sleep. In two patients with SA and CH, treatment with continuous positive airway pressure abolished their oxygen desaturation, sleep apnoeas and headaches. Our study confirmed the high percentage of CH associated with SA. We suggest that oxygen desaturation may be a trigger factor in some patients and play a role in the pathogenesis of CH.
Introduction
Cluster headache (CH), firmly established as the most excruciating chronic headache in intensity, is a rare syndrome and shows unique clinical features (1). Descriptions regarding the clinical features of this condition have been made for more than two centuries. Although extensive studies have been conducted, the pathophysiology of this condition remains obscure (2). One of the most striking features of CH is the periodicity of the attacks. The attacks are short-lived and followed by a pain-free interval. They also occur during cluster periods, on the same day, with predictable periodicity. Additionally, 50–60% of the attacks occur often or exclusively at night (3). The relation between headaches and sleep has been known for more than a century (4). Further studies showed an increased prevalence of obstructive apnoea syndrome in patients with CH compared with the general population, and that the attacks could be triggered by oxygen desaturation. In these cases, treatment with continuous positive airway pressure (CPAP) was shown to abort the cluster (5).
These studies may add information to the current pathophysiological hypotheses and, above all, offer other therapeutic options that might benefit the patients.
Hypothalamic involvement has been suggested in CH due to the periodicity of the CH, probably as a result of the circadian rhythm. This hypothalamic dysfunction is believed to cause autonomic nervous system involvement. Specifically, it is suggested that during the cluster period the activity of chemoreceptors would be impaired by the central inhibition of the sympathetic vasomotor tone and parasympathetic stimulation. Thus, CH may be the result of decreased sympathetic activity and stimulation of parasympathetic disinhibition in the carotid body. Attacks occurring as a direct result of these abnormalities are unlikely. Rather, they may occur as a result of physiological involvement combined with facilitating conditions, such as inhibition of respiratory muscles during the REM phase of sleep; bradycardia and hypoventilation in the nREM phase of sleep; use of vasodilator agents; altitude
Goadsby, using positron emission tomography, reported ipsilateral hypothalamic activation in patients during the attacks (7, 8). According to this author, these findings warrant the inclusion of CH in the category of neurovascular disorders.
Methods
Sixteen out-patients (14 male and two female, 26–55 years of age, mean age 40 years) were studied. Their clinical history was taken, they underwent neurological examination and the following tests: blood cell count, electrocardiography (ECG), computed tomography (CT) of the brain and nocturnal polysomnography. All patients met the International Headache Society criteria for the diagnosis of episodic CH. In accordance with the main objectives of the study, patients with concomitant heart disease, pulmonary disease or haematological disease were excluded, as the presence of these conditions would be likely to bias the results. The presence of significant brain CT abnormalities was also established as an exclusion criterion.
Upon questioning, none of the patients spontaneously reported snoring, daytime sleepiness or any other sleep disorder. Before the physical examination, the patients recorded their daytime sleepiness on a scale called Epworth scale. This scale uses a scoring system (0 = none, 1 = small, 2 = moderate, 3 = high) to record the odds of falling asleep in the following situations: reading while sitting, watching television, traveling by car during 1 h, lying down during the afternoon rest, talking with another person, while sitting after a dinner without alcohol ingestion, when the car stops for some minutes in traffic, and while sitting down, inactive, in public places (theatres, cinemas, etc.). The result is considered normal if the sum of the items described above provides a score not higher than 7. Scores above this value are associated with a high likelihood of sleep apnoea. This scale is not designed to determine the severity or the prognosis of the condition, but is a useful contributor for the indication of polysomnography (9). The polysomnographic studies included EEG, right and left electro-oculogram, submental muscle electromyograms, right and left anterior tibial muscles electromyograms, ECG, nasal and oral termistors for the evaluation of the airflow, thoracic and abdominal excursion and finger oximetry. The studies were evaluated by the same person. Apnoea was defined as complete airflow cessation for ≥ 10 s during sleep. Hypopnoea was defined as a reduction in airflow for ≥ 10 s, with chest excursions that led to a ≥ 4% oxyhaemoglobin desaturation, arousal, or awakening. The apnoea/hypopnoea index (AHI) was calculated as the number of recorded apnoeas and hypopnoeas divided by the total hours of sleep (10). Both are generally associated with desaturation and arousal, detected through the EEG. Oxygen desaturation is considered clinically significant when it is ≥ 4% inferior to the baseline saturation value of each patient (11).
Patients were seen during cluster periods, while using prophylactic medication on a regular basis. The medication was discontinued 1 week before the nocturnal polysomnography was conducted. Twenty-nine individuals were enrolled in the control group (26 male and three female, 19–59 years of age, mean 37 years). These individuals were comparable in terms of age and body mass index (BMI). There were more males than females. The patients did not complain of headache, or had any other physical abnormalities.
The data related to the study variables were analysed, and are presented in the following tables. The statistical analysis was conducted using the Wald χ2 used to assess the association among variables; Student's t-test to compare the means; and the non-parametric Mann–Whitney test to compare extremely variable measures of both samples. Pearson's linear coefficient of correlation (r) was used to assess the dependence among values of the variables. The significance level was established at a probability of 5% (P < 0.05).
Results
In patients with CH, the age of symptom onset ranged from 14 to 48 years, with a mean age of 30.9 years. Eight patients (50%) suffered from the pain mainly at night, but none of the patients suffered from the pain exclusively during sleep. The pain was most incident between 02.00 h and 03.00 h. The results of both groups were tabulated and categorized as group 1 (patients with CH) and group 2 (patients from the control group: Table 1, group 1; and Table 2, group 2.
Group 1
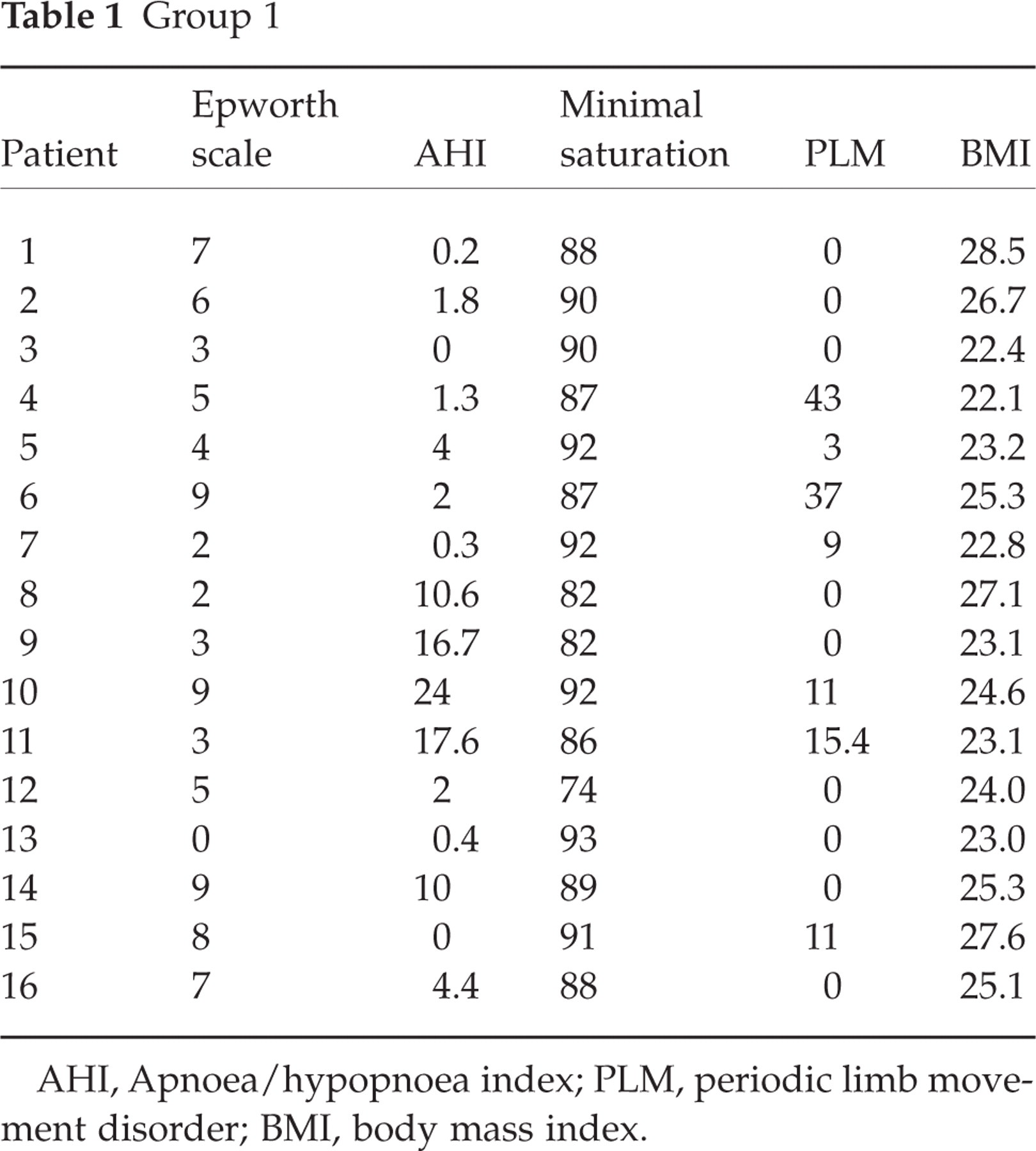
AHI, Apnoea/hypopnoea index; PLM, periodic limb movement disorder; BMI, body mass index.
Group 2

AHI, Apnoea/hypopnoea index; PLM, periodic limb movement disorder; BMI, body mass index.
According to the criteria of abnormality, of the 16 patients studied in the first group, five presented with SA (AHI > 5/h), corresponding to 31.3%. Of the 29 patients in the control group, three presented with SA, corresponding to 10.3% (P = 0.08). When the results obtained from the patients with CH (31.3%) were compared with those of the general population (2–4%), a significant difference was found (P < 0.05). The comparison with the control group was also significant (P = 0.08). There were only four patients in our study whose score in the Epworth Sleepiness Scale was higher than seven. Of the first group of patients, nine had values within this range, corresponding to 56.2%, vs. 13 patients in the second group, corresponding to 44.82%. The difference was not significant (P > 0.05). According to the criteria for PLM (Periodic Limb Movement Disorder), the normal and abnormal values were the following: in the first group, 10 normal and six abnormal values; second group, 21 normal and eight abnormal values. The non-parametric χ2 test was used (=0.47) (P = 0.49), and was considered non-significant. The evaluation of the sleep architecture showed an increase of stage 1 in patients with CH. The value of the t-test (=2.14) (P = 0.03) was considered significant. During REM sleep, the mean values and the standard deviations were x = 14.25, s = 6.2 in the first group; and x = 16.76, s = 6.5 in the second group. The value of the t-test was 1.25 (P = 0.21). This result is considered non-significant for the REM sleep. In terms of BMI, the means and standard deviations of the two groups were the following: first group –x = 24.62, s = 1.99; and second group –x = 24.26, s = 2.26. The value of the t-test (=0.53] (P = 0.60) is considered non-significant. When the non-parametric χ2 test was used, a × 2-value of 0.38 was found (P = 0.054), indicating the similarities between both groups. Two patients had two pain attacks, both during REM sleep and during desaturation.
Discussion
The results of this study support the presence of a higher percentage of sleep apnea syndrome (OSAS) among patients with episodic CH. Albeit not a rare condition, OSAS is usually more prevalent with increasing ages and BMI. The mean age of the patients included in our study was 30.9 years. This is not the most prevalent age group reported for OSAS. When our statistical results (31.3%) were compared with those described in the world literature (4%) (12) for the prevalence of OSAS in the general population, very significant results were found (P < 0.05). The comparison with the control group also showed significant results (P = 0.08). Kudrow et al., studying 10 patients with CH (five episodic and five chronic), showed an overall prevalence of OSAS of 60% in these patients, including all patients with the episodic form and one with the chronic form (3). Chervin et al. conducted a polysomnography study in 25 patients with CH, and found that 80% of these patients had sleep-disordered breathing (10). The BMI was not assessed, and this could have biased the statistical findings. The lack of control groups also impaired the analysis.
Our study reports only two attacks occurring during polysomnography in two patients with OSAS. Both occurred during REM sleep, after an episode of desaturation. These numbers, albeit limited, are consistent with those reported in the literature, which consider oxygen desaturation a trigger factor or a factor related to the pathophysiology of the disease. In our study, the sleep structure abnormalities found in patients with CH were not significant compared with those in the control group. However, a reduction in REM sleep was found in patients with CH, perhaps reflecting more episodes of arousal. An increased prevalence of PLM was detected among our patients; however, the comparison with the control group was not significant, and demonstrated an increase of PLM among all the study individuals. The sleep structure abnormalities found in the patients with CH in our study were not significant when compared with the control group, although the control patients showed a decrease in REM sleep. It is believed that these structural abnormalities can happen in the first night of a study due to the difficulties of the patients in adjusting to the new environment.
The attacks are usually associated with high altitudes, REM sleep and use of alcohol, histamine or sublingual nitroglycerin. All these factors may cause a state of hypoxaemia in the absence of a normal reflex chemoreceptor response. Thus, Kudrow proposed that, during the time in which the chemoreceptor activity remains abnormal due to the changes in autonomic activity, hypoxaemic stimuli acting over a deregulated threshold would cause a hyperactive reflex chemoreceptor response (13). This theory is supported by the efficacy of oxygen administration during the attacks. It seems that O2 inhibits the excessive excitability of chemoreceptors. Other authors believe that oxygen's vasoconstrictor activity in cranial and extracranial vessels would account for the improvement of the pain. The association with sleep apnoea emerged after analysing the polysomnographic findings, which showed that the attacks were triggered by episodes of desaturation.
Of the five patients with OSAS, two were treated with CPAP and their pain symptoms improved. Both were unresponsive to pharmacotherapy. After CPAP, both showed complete resolution of the pain. These patients have now been followed for 15 and 13 months, respectively. The first patient reported resolution for 1 year and the other patient reported resolution for 8 months. The time in remission seemed to have increased in both patients after treatment with CPAP. There is a similar case described in the literature (5). This finding might favour a new therapeutic option for these patients with CH associated with OSAS.