
Abstract
The objective of this study was to estimate prevalence of headache and body pain among patients referred for suspected sleep apnoea syndrome compared with the occurrence in a large population-based study (the Nord-Tr⊘ndelag Health Study). Between 1995 and 1998, ambulatory polysomnography was successfully performed in 421 consecutive patients, 324 of whom completed a questionnaire about sleep-related habits, headache and body pain. Headache and neck pain were more likely among patients admitted for polysomnography compared with the general population (n = 41 340). In the multivariate analyses, this association was mainly restricted to those with frequent complaints (≥7 days per month). Chronic headache (headache ≥ 15 days per month) was seven times more common among individuals with and without confirmed obstructive sleep apnoea syndrome than in the general population. There was no linear dose-response relationship between headache and neck pain and severity of apnoea or oxygen desaturation. Thus, hypoxia per se is less likely to explain the high headache prevalence among patients admitted for polysomnography.
Introduction
Obstructive sleep apnoea syndrome (OSAS) is defined as repeated episodes of obstructive apnoea and hypopnoea during sleep, with sleep disruption and excessive daytime sleepiness as common consequences (1). Sleep apnoea patients are also at increased risk for hypertension, and for cardiovascular and cerebrovascular events (1–3). Snoring is a common symptom, but only a small minority of snorers have OSAS. In an unselected population, approximately one out of five subjects were snoring every or almost every night (4), whereas OSAS affects only 1–4% of adults (5–7).
Controversy exists regarding the relation between headache, snoring and sleep apnoea. Headache was more frequent in snorers than in the general population in some studies (8, 9), but others failed to confirm this (10). An association between OSAS severity and headache has not always been found (11).
The aim of the present study was to evaluate the prevalence of headache, neck pain, and pain in other parts of the body among patients admitted for polysomnography with and without confirmed OSAS compared with the general population. We also wanted to examine a possible relation between prevalence of headache, neck pain, and other pains with severity of apnoea and oxygen desaturation measured by polysomnography.
Materials and methods
Between 1995 and 1998, ambulatory one-night polysomnography was successfully performed in 421 consecutive patients (92 women, 329 men) referred for suspected OSAS to the sleep laboratory of Trondheim University Hospital. Out of these 421 patients, a total of 324 (77%) (70 women and 254 men) responded to a 48-item self-administered questionnaire concerning sleep habits, sleep-related symptoms, headache and pain in other parts of the body. A total of 303 (94%) reported snoring during sleep, and 289 (89%) reported daytime sleepiness.
The first headache question, ‘Do you suffer from headache?’, had five response alternatives: ‘Daily, more than 14 days per month, 7–14 days per month, less than 7 days per month, and no headache complaints’. Individuals who confirmed they suffered from headache were asked to fill in questions about frequency, onset, duration, temporal pattern, localization, pain characteristics, accompanying features, and triggering factors. All participants had to answer the question ‘Have you bothersome pain located in other body regions (back, neck, muscles or joints)?’, and they were given similar five response options as for the initial headache question. Subjects with pain were also asked to specify the localization of this pain. Based on headache frequency, headache sufferers were divided into three levels: those with headache frequency of < 7 days per month, with headache frequency between 7 and 14 days per month, and with headache frequency of> 14 days per month.
Individuals who did not complete the form were insignificantly older (48.2 vs. 45.6 years, P = 0.08) and more obese (body mass index (BMI) 28.6 vs. 27.6 kg/m2, P = 0.17) than those who answered the questionnaire. However, the apnoea index (AI) did not differ (10.4 vs. 10.0/h, P = 0.84).
For each sleep study, the Oxford MPA-2 system was used. The electroencephalogram (C4-A1 derivation; International 10–20 system), two-channel electro-oculogram, and submental electromyogram were recorded with surface electrodes. Airflow was assessed with nasal-oral thermistors, respiratory movements with thoracic and abdominal inductive plethysmography, and blood oxygen saturation with a pulse oximeter index finger probe. AI was defined as the total number of apnoeic episodes per hour of sleep with> 80% airflow decrease for at least 10 s. Each apnoea was scored as either obstructive, mixed or central according to the respiratory movement pattern. No patient had a central apnoea disorder. The minimal diagnostic criteria for OSAS were defined as an AI ≥ 5/h (1, 12). We also evaluated prevalence of headache and body pain according to the oxygen desaturation index (ODI) defined as the average number of desaturations> 4% per hour of the sleeping period.
Participants in the Nord-Tr⊘ndelag Health Survey (HUNT) conducted between 1995 and 1997 were used as controls. Details of the study have been reported elsewhere (13). Briefly, all the 92 566 inhabitants aged ≥ 20 years were invited, of whom 46 144 (50%) completed all the relevant questions about headache and musculoskeletal complaints. A subgroup of 41 340 persons (18 646 men, age range 20–70 years; and 22 694 women, age range 23–79 years) was selected in order to match the age distribution of the patients admitted for polysomnography (Table 1). Individuals who answered ‘yes’ to the question ‘Have you suffered from headache during the last 12 months?’ had to fill in questions about, for example, headache frequency, duration, and pain characteristics. Details of the headache questionnaire have been described previously (13). Participants who answered ‘yes’ to the question ‘Have you during the last month suffered from pain/discomfort in muscles and/or joints?’ were asked to specify the localization.
Characteristics of patients admitted for polysomnography compared with the general population

Statistical analysis
Difference between proportions was analysed by χ2 tests. Differences between means were tested with the unpaired t-test. P-values < 0.05 were considered statistically significant. We estimated prevalence odds ratios (OR) for the association between headache and OSAS. In multivariate analyses, using unconditional logistic regression, we evaluated potential confounding by age (5 years categories), gender, BMI, and self-reported information about: occupational status (paid work or not), smoking (never vs. current or previously), hypertension (yes/no), heart disease (yes/no), and epilepsy (yes/no). The precision of the OR was assessed with 95% confidence intervals (CI).
Ethics
The HUNT study was approved by the Regional Committee for Ethics in Medical Research, and by the Norwegian Data Inspectorate.
Results
Men and women admitted for polysomnography were more obese, and had a higher prevalence of hypertension, heart disease (men only), and epilepsy. They were also more likely to smoke compared with an age-trimmed HUNT population (Table 1). As a consequence, we adjusted for potential confounding with these variables in the multivariate analysis. Out of the 324 patients admitted for polysomnography, a total of 128 (40%) (108 men and 20 women) had an AI ≥ 5/h indicating OSAS.
Headache
Prevalence of headache was higher in the group of 324 patients admitted for polysomnography than in the general population, i.e. 57% vs. 30% (P < 0.00001) in men and 76% vs. 47% in women (P < 0.00001). In the multivariate analyses, the association between polysomnography-admitted patients and headache was mainly restricted to individuals with headache ≥14 days per month (Table 2). Chronic headache was seven times more likely among patients both with and without confirmed OSAS (Table 2).
Prevalence odds ratio (OR)∗ of headache according to apnoea index level

No, Number of subjects.
∗Adjusted for age, gender, occupational status, hypertension, smoking, heart disease, body mass index, and epilepsy.
†CI, Confidence interval.
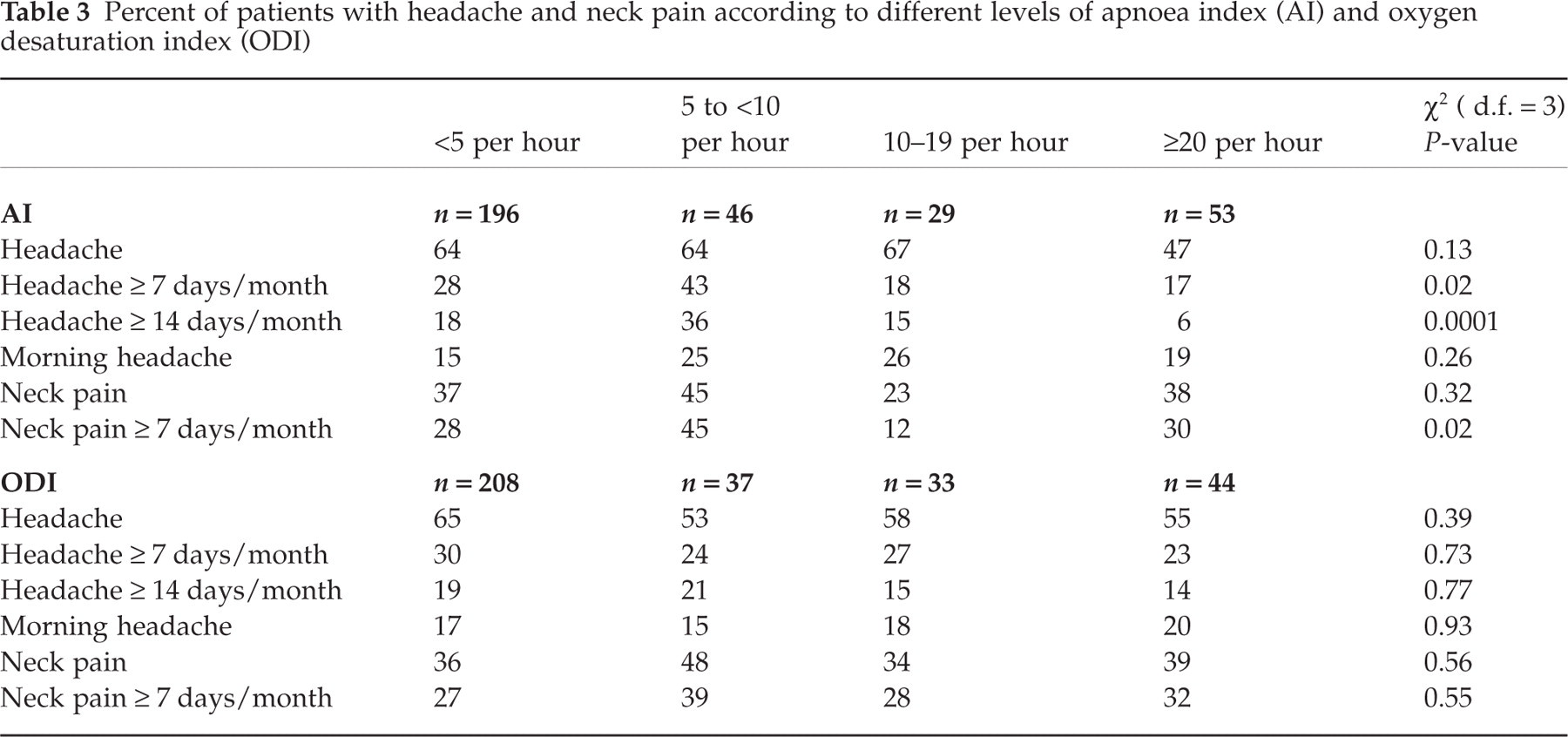
Prevalence of frequent and chronic headache (≥7 and ≥14 headache days/month, respectively) was significantly higher among individuals with AI between 5 and 10 compared with the groups with higher AI (P = 0.02 and P = 0.0001). We found no consistent linear dose relationship between headache and severity of apnoea and oxygen desaturation (Table 3).
Percent of patients with headache and neck pain according to different levels of apnoea index (AI) and oxygen desaturation index (ODI)
There was no significant difference in prevalence of morning headache between individuals with AI ≥ 5/h compared with those with AI < 5/h (Table 4). Duration of headache, pain intensity, and localization of headache at onset did not differ between the two groups (Table 4).
Headache characteristics in the group of headache sufferers with apnoea index (AI) ≥ 5/h compared with apnoea index < 5/h

Body pain
There was no difference in prevalence of body pain in general among patients admitted for polysomnography compared with the general population (67% vs. 65%, P = 0.67). Neck pain was, however, more likely, i.e. 37% vs. 32% (P = 0.03). In multivariate analyses, neck and shoulder pain ≥ 7 days/month was more common (OR = 2.0, 95% CI 1.5–2.7 and 1.5, 95% CI 1.1–2.0) in the group of polysomnography-admitted patients compared with the general population (OR = 1.0). No linear dose–response relationship between neck pain and severity of apnoea and oxygen desaturation was found (Table 3).
Discussion
The main finding was a strong association between chronic headache and patients with and without polysomnography-confirmed OSAS. Furthermore, there was no dose relationship between headache and severity of apnoea and oxygen desaturation.
In the present study, we used a large unselected population of adults living in the same area as controls, a strategy also chosen by others (8). The questionnaires were comparable, but the initial headache question was less rigorous for the polysomnography-admitted patients than for the general population in the HUNT study. Thus, there was no restriction in time for the question ‘Do you suffer from headache?’, in contrast to the HUNT question, ‘Have you suffered from headache during the last 12 months?’. Different phrasing of this first headache question may have given a slight overestimation of the difference in headache prevalence between the two groups.
Headache was a frequent symptom among patients admitted for polysomnography. In agreement, Ulfberg et al. (8) reported that headache at least once a week was more likely among heavy snorers and OSAS patients compared with the control group, and Jennum et al. (9) found an association between headache and self-reported snoring. However, these authors did not analyse whether this association varied with headache frequency. To the best of our knowledge, this is the first study showing that, irrespective of whether OSAS was present or not, the association was restricted to those with chronic headache.
The diagnostic criteria for OSAS differ between studies, and in many recent studies the OSAS diagnosis has been based on the apnoea plus hypopnoea index (e.g. (5, 6, 10, 11, 14)). In the present study we used the AI, since the validity seemed to be better for apnoeas than for hypopnoeas in our method (qualitatively judged, e.g. by the lack of agreement between automatic scoring and attempted visual scoring of hypopnoeas). Like Guilleminault et al. (12), we diagnosed OSAS in individuals with AI of ≥ 5. The clinical significance of an AI barely greater than 5, particularly in the elderly, has been debated (15). However, we repeated all analyses when OSAS was diagnosed in individuals with AI of ≥10, but this did not change our main results.
Our patients were evaluated by ambulatory polysomnography, probably minimizing the ‘first night effect’ seen in some sleep laboratory recordings. Most contemporary sleep studies seem to use single-night recordings, although a second investigation might increase the diagnostic sensitivity (16).
‘Sleep apnoea headache’ is a separate headache type in the Headache Classification Committee of the International Headache Society, 1988 (IHS) (17), but no diagnostic criteria are stated. Morning headache, described as frontal or diffuse over the scalp (11), is often listed as a common symptom in OSAS (18, 19), and many reports demonstrate improvement in morning headache after treatment of OSAS (20, 21). In the present study, the total group of individuals with confirmed OSAS was only slightly more likely to report headache onset at night and morning headache compared with the polysomnography-admitted patients without OSAS. We could not confirm what Loh et al. (14) reported: that patients with more severe OSAS were more likely to have morning headaches compared with patients with mild OSAS.
Controversial results exist regarding morning headache. On the one hand, morning headache was equally or less frequent among patients with ‘sleep-disordered breathing’ compared with snoring and non-snoring subjects (10), and among patients with other causes of sleep-disordered breathing or sleep disorders than in patients with sleep apnoea (11, 20). On the other hand, in other studies morning headache was more likely in snorers compared with non-snorers (9), and in heavy snorers and patients with OSAS compared with the general population (8).
The reason for the high headache prevalence among patients admitted for polysomnography is unclear. Possibly, this may partly be an effect of a referral bias, if patients with headache and neck pain are more likely to be referred for investigation with polysomnography than are patients without such symptoms. The fact that body pain as a whole was not more frequent among the polysomnography-admitted patients than in the general population may argue against this explanation.
A possible biological explanation for the high headache prevalence may be, as suggested by others (8, 11), the ventilatory effort seen in patients with sleep-disordered breathing. The vast majority of the patients admitted for polysomnography self-reported snoring, and snoring is associated with an increase in upper airway resistance, and as a consequence increased inspiratory effort (19). Neck pain was frequent among patients admitted for polysomnography, and others have noted excessive neck movements in sleep apnoea patients (22). These findings may suggest that altered muscle activity in the upper body region may be involved as a cause of headache.
Some authors have suggested hypoxia and subsequent cerebral vasodilatation as a cause of headache, but our data do not support this hypothesis. In accordance with Aldrich et al. (11), we found no linear dose–response relationship between headache or neck pain and severity of apnoea and oxygen desaturation. In fact, the prevalence of chronic headache seemed to be low among patients with the most severe apnoea. This may reflect that respiratory effort could be stronger in many patients with slight OSAS compared with those with severe apnoea.
The compensatory increased activity of upper-airway muscles preventing airway collapse is linked to negative intrathoracic pressure, which may reduce the intracranial venous pressure as well as the cerebrospinal fluid (CSF) volume. Low CSF pressure is a well-known headache trigger (23), and speculatively, this factor may be of importance for the high prevalence of headache among the group of patients referred for suspected OSAS.
There is a strong relationship between headache, especially chronic headache, and anxiety and depressive disorders (24, 25). Confounding with these conditions may, at least in part, explain the high headache prevalence among patients admitted for polysomnography, since anxiety and depression are common underlying contributors to sleep disturbance in patients who are seen at sleep centres (11). Other proposed mechanisms by which headache might occur are, for example, frequent arousals and sleep stage disruption which may produce a headache, either by increasing daytime fatigue and sleepiness or because of an as yet unknown neurochemical mechanism (20).
In conclusion, chronic headache was more likely in patients with or without polysomnography-confirmed OSAS compared with the general population. There was, however, no linear dose–response relationship between headache and severity of apnoea and oxygen desaturation. Thus, hypoxia per se is less likely to explain the high headache prevalence among patients admitted for polysomnography.