
Abstract
Background: The objective was to investigate the prevalence and clinical characteristics of sleep apnoea headache.
Methods: A postal questionnaire was received by 40,000 Norwegians from the general population. A total of 376 and 157 persons with high and low risk of sleep apnoea according to the Berlin Questionnaire had a polysomnography, and a clinical interview and examination by physicians.
Results: Sleep apnoea headache was diagnosed in 11.8% of the participants with obstructive sleep apnoea (OSA), while morning headache with similar symptomatology was diagnosed in 4.6% of the participants without OSA (p = 0.002). After adjusting for potential confounders the odds ratio for OSA remained significantly increased among participants with morning headache with an adjusted odds ratio of 2.92 (1.31–6.51). When using a cut-off of moderate (apnoea hypopnea index, AHI ≥ 15) and severe (AHI ≥ 30) OSA, the prevalence of sleep apnoea headache was 11.6% and 13.3%, respectively. Average oxygen desaturation and lowest oxygen saturation was not significantly different in participants with OSA with and without morning headache.
Conclusion: Morning headaches were significantly more frequent among participants with OSA than those without OSA. Sleep apnoea headache is less common in the general population than has previously been reported in clinic populations. The relation of hypoxia and morning headache is questioned.
Introduction
Obstructive sleep apnoea (OSA) is a disorder with partial or complete obstruction of the upper airways during sleep that constitutes hypopnea and apnoea and will typically result in repeated airflow cessation, oxygen desaturation and sleep disruption. The disruption of sleep may then result in excessive daytime sleepiness, unrefreshing sleep, daytime fatigue or reduced cognitive function (1). There is increasing evidence that OSA is associated with cardiovascular disease (2). OSA syndrome is defined as an apnoea hypopnea index (AHI) of at least five apnoeas or hypopneas per hour of sleep, in conjunction with symptoms such as daytime somnolence. This is a common disorder among middle-aged adults with an estimated prevalence of 4% among men and 2% among women (3,4). When the definition of OSA is defined solely by an AHI ≥ 5, the estimated prevalence among middle-aged adults is approximately 20% in the general population (3,5,6).
The International Classification of Headache Disorders (ICHD II) classifies sleep apnoea headache as a secondary headache, i.e. a recurrent morning headache with polysomnography (PSG) verified AHI ≥ 5 and cease of headache within 72 hours after effective treatment of sleep apnoea (7). The prevalence of morning headache has been reported in variable levels from 15 to 60% in patients with OSA (8–11). However, several other studies have found morning headache to merely be a non-specific symptom with no clear relationship with OSA (12–14). Thus, there is still controversy regarding the association of morning headache and OSA.
The aim of the present study was to investigate the prevalence and clinical characteristics of morning headache among persons with and without PSG-verified OSA in a population-based sample.
Methods
Sampling and representativeness
This is a cross-sectional population-based study. An age- and gender-stratified random sample of 40,000 persons aged 20 to 80 years old were drawn by the National Population Register. Each of the ages 30, 35, 40, 45, 50, 55 and 60 years included 2000 persons of each gender, while the remaining ages included 1000 persons of each gender. The participants were residing in Akershus, Hedmark or Oppland County in Norway. The three counties have both rural and urban areas, and Akershus County is situated in close proximity to Oslo. Data from Statistics Norway have shown that the sampling area was representative for the total Norwegian population regarding age, gender, marital status and level of education. The employment rate was equal, but employment in trade, hotel/restaurant and transport were over-represented, while industry, oil and gas and financial services were under-represented in the sampling area as compared to the total Norwegian population. As shown in Figure 1, the sample size was reduced to 38,871 because of error in the address list (n = 1024), multi-handicap (n = 4), dementia (n = 23), insufficient Norwegian language skills (n = 3) and deceased (n = 75). All participants received a standard letter by mail containing information about the project and a short questionnaire, including the Berlin Questionnaire. The Berlin Questionnaire was used to classify respondents to be of either high or low risk of OSA (15). If the questionnaire evoked no response, a second mailing was sent. The replies could either be on paper or electronic. The overall response rate was 54.5% (21,177/38,871), and it was significantly higher among women than men (n = 11,120 vs. n = 10,057; p < 0.001). Questionnaires received later than 4 months after the first mail or not containing a telephone number necessary for re-contact (n = 770) and questionnaires delayed in the screening procedure (n = 672) were regarded as not eligible for inclusion in further investigations. Respondents aged 30 to 65 years were then invited by mail to a clinical evaluation and contacted by telephone. If they could not be reached within three attempts, no further attempts were made (n = 202). Exclusion criteria applied to all participants contacted by telephone and were: use of continuous positive airway pressure (n = 10), pregnancy (n = 9), lack of Norwegian language skills (n = 5) and severe physical impairment (n = 4). An age- and gender-stratified sample of 378 persons with high risk and 157 persons with low risk of sleep apnoea aged 30–65 years were then included for further investigations. The remaining 13,510 persons were not invited for a physical and neurological examination or PSG. In case of technical failure in the PSG recordings, the participants were asked to return for a second recording. Because two people refrained from such a second PSG recording, the final study sample in the present study comprised of 533 (376 high risk and 157 low risk) people. A total of 585 people decided not to participate, yielding a participation rate of the interview and examination of 47.7%. Participants and non-participants were not significantly different regarding self-reported headache, depression, excessive daytime sleepiness, gender or age. However, self-reported simple snoring was over-represented in the low-risk group in the study sample, as compared to all respondents of the questionnaire with low risk.
Flow chart of the study population according to type of participation. M and F denotes males and females.
Clinical evaluation
The participants were all admitted to Akershus University Hospital (Stensby Hospital), Norway and underwent an extensive clinical interview including a semi-structured headache interview and a physical and a neurological examination by three physicians. The semi-structured headache interview focused on migraine, tension-type headache and sleep apnoea headache, but included all types of headache. The physicians were blinded regarding the participant’s replies on the questionnaire, i.e. high vs. low risk of OSA by the Berlin Questionnaire. The diagnosis of sleep apnoea headache was based on the International Classification of Headache Disorders (ICHD II), but did not include criterion D, i.e. headache ceases within 72 hours, and does not recur after effective treatment of sleep apnoea (7). We used the diagnosis of sleep apnoea headache if the AHI was ≥5, while we used the diagnosis of morning headache if the AHI was <5. For further details see the methodological section in the discussion. The Hospital Anxiety and Depression Scale (HADS) was used to screen for depression (16). The replies were dichotomised and depression was defined by a score of 8 or above on the subscale of depression (HADS-D) (17). Excessive daytime sleepiness was assessed by the Epworth Sleepiness Scale (18). The results were dichotomised into scores of ≤10 and >10, the latter being considered to represent clinically significant excessive daytime sleepiness (19). All participants then underwent in-hospital PSG performed on standard, multichannel Embla™ PSG devices (ResMed Corp., Poway, CA, USA). The recordings included a two-channel electroencephalograph (C4/A1, C3/A2 according to the 10–20 international electrode placement system), a two-channel electro-oculogram, a one-channel submental electromyogram, leg EMG (tibialis), SaO2, breathing movements (Respitrace; Ambulatory Monitoring, Ardsley, NY), air flow (Protech, Woodinvill, WA) and body position. All electrophysiological signals were pre-amplified, stored and subsequently scored (30-second epochs using Somnologica 3.2 software package, Flaga-Medcare, Buffalo, NY) according to the Rechtschaffen and Kales scoring manual by two US board certified PSG technicians who were blinded to the result of the Berlin Questionnaire (20). Arousals were documented and classified (21). Obstructive apnoeas were scored when a 90% decrease of flow occurred for more than 10 seconds. Hypopneas were defined as a 30% decrease in flow for more than 10 seconds with subsequent oxygen desaturation of at least 4%. The AHI was calculated as the average of total number of apnoeas and hypopneas per hour of sleep. In this study the participants with AHI ≥ 5 were classified with OSA.
Statistical analyses
The statistical analyses were performed using SPSS Base System for Windows 16.0. Chi-square tests and logistic regression modelling with 5% level of significance were used. Fisher’s exact test was used when appropriate. Student’s t-test and Mann-Whitney U-test were used to compare normally and non-normally distributed continuous variables. In our multivariable logistic regression model morning headache was used as the dependent variable, while OSA, depression, gender, body mass index and age were independent variables.
Ethical issues
The project was approved by the Regional Committees for Medical Research Ethics and the Norwegian Social Science Data Services.
Results
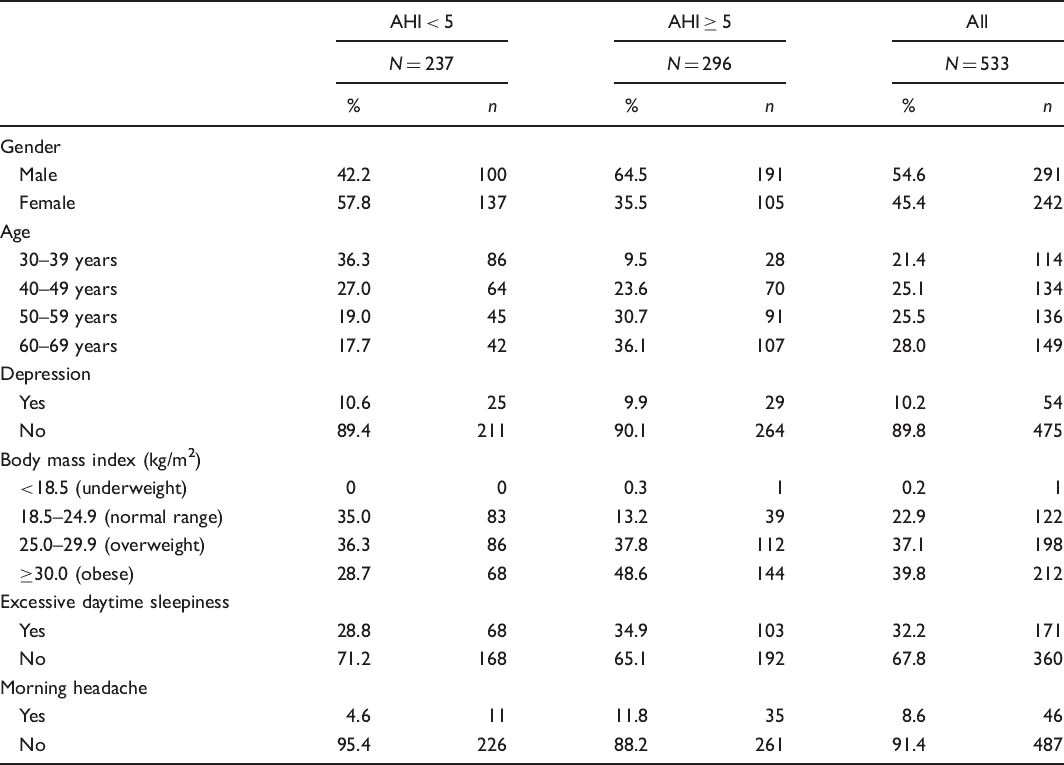
Distributions of selected characteristics of the sample (N = 533)
Clinical characteristics of sleep apnoea headache and morning headache

No significant differences between the two groups in any of the characteristics.
When comparing participants with sleep apnoea headache with participants with OSA without morning headache, we did not find any significant differences in total sleep time and average oxygen saturation. Regarding the variables indicating hypoxia, participants with sleep apnoea headache did not have significantly more minutes below 90% oxygen saturation (23.1 min vs. 22.4 min, p = 0.517), higher level of average oxygen desaturation (5.9% vs. 5.8%, p = 0.749) or lower average of the lowest oxygen saturation (80.9% vs. 81.8%, p = 0.571) as compared with OSA participants without morning headache.
Crude and adjusted odds ratios (cOR and aOR) with 95% confidence intervals (CI) for morning headache by obstructive sleep apnoea, depression, gender, body mass index and age

Data was missing in four people, so the analysis above was based on 529 people.
Discussion
Results
The main finding in this population-based cross-sectional study was the demonstration of a significant relationship between morning headache and OSA. This is concurrent with the findings from a recent clinic-based study from Turkey (22). However, we could not confirm their findings that the prevalence of morning headache increases with increasing severity of OSA. We found that the prevalence of morning headache was similar in mild (AHI ≥ 5), moderate (AHI ≥ 15) and severe (AHI ≥ 30) OSA, in accordance with two previous case-control studies from the USA and Norway (12,23). Few studies have evaluated this relationship in the general population. In a large survey of the general populations of the UK, Germany, Italy, Portugal and Spain, the prevalence of chronic morning headache was 7.6%, while 15.2% reported both morning headaches and breathing-related sleep disorder (24). We found that 11.8% of the participants with PSG-confirmed OSA had morning headache. The methodological differences between these studies were that our participants went through a headache interview and examination by physicians and evaluated sleep-disordered breathing by PSG, while the other study was based solely on a structured telephone interview by a lay interviewer (24). A Swedish questionnaire-based study found a positive correlation between heavy snoring, OSA and morning headache (18% vs. 5% from the general population) (8). There were, however, no significant differences in headache among the two groups of heavy snoring and OSA. This may indicate that there is no linear dose–response relationship between morning headache and severity of OSA (8,12,23).
The clinical characteristics of sleep apnoea headache and morning headache were both predominantly of bilateral, pressing/tightening of mild or moderate intensity with few accompanying symptoms, which is in accordance with ICHD II (7). However, the majority of our participants reported that the morning headache lasted longer than the 30 minutes listed as typical in ICHD II. These findings are concurrent with previous studies that also found similar clinical characteristics of morning headaches in OSA patients and in controls, as well as the headaches needing more than 30 minutes to resolve (11,22).
The present study was not designed to investigate the pathogenic basis of sleep apnoea headache, but nevertheless it did give some insights into the possible mechanisms. In ICHD II hypoxia has been suggested as an important mechanism by which OSA causes morning headache (7). This has been supported by studies finding a dose–response relationship between morning headache and severity of OSA (10,11,22). We did not find such a relationship nor did we find a correlation between sleep apnoea headache and the severity of nocturnal oxygen desaturation, when comparing with participants with OSA but without morning headache. This is concurrent with previous studies casting doubt on the hypothesis of oxygen desaturation as a cause of morning headache in those with OSA (12,23,25–28). Hypoxia may not be a sufficient factor in this complex mechanism and may need an elevated intracranial pressure as well (29). Or it might be that nocturnal oxygen desaturation is only important in susceptible persons, in the same way as migraine with aura can be precipitated by sunlight only in people susceptible to migraine with aura and high-altitude headaches do not occur in all people at the same height. What we can say is that the mechanism of sleep apnoea headache/morning headache is intriguing, but still unsolved.
Methodological considerations
The screening tool included the Berlin Questionnaire, in order to classify participants as at high or low risk of OSA (15). The sensitivity and specificity are 0.77 and 0.89 in the respiratory disturbance index ≤5, and 0.86 and 0.77 if it is >5.
We used the explicit diagnostic criteria of ICHD II, but criteria A and B were expanded, i.e. in criterion A we also allowed for headache duration ≥30 min and in criterion B we included all, irrespective of respiratory disturbance index ≥5, as those with index <5 were classified with morning headache. This was necessary in order to shed more light on sleep apnoea headache. Criterion D was excluded, because this is a weak and possibly not valid criterion. In the revised version of ICHD II such criteria are likely to be omitted, because it is impossible to form a diagnosis unless the type of headache is resolved, and then it is not clinically relevant any more.
The strengths of this study are the inclusion of a large sample of people age 30 to 65 years old from the general population who received the questionnaire, the use of interview and examination by physicians regarding the diagnosis of headache and the use of PSG to diagnose OSA. The questionnaire response rate was relatively low. However, similar replies to the first and second questionnaires issued, as well as electronic responses, suggest that responders and non-responders are no different. A previous Danish epidemiological survey found no significant difference in the frequency of migraine among responders and non-responders (30). In addition the response rate is comparable to that of other sleep-related epidemiological studies (31,32).
The relatively low participation rate is a potential limitation of the study. However, participants and non-participants were not significantly different regarding headache, depression, excessive daytime sleepiness, gender or age. Regarding the difference between the participants and the study population, we discovered that self-reported simple snoring was over-represented in the low-risk group in the study sample, as compared to all respondents of the questionnaire with low risk. As there may exist a relationship between snoring and headache, this may have contributed to a slight overestimation of morning headache in participants without OSA in the current study (8,33). The exclusion of people already using continuous positive airway pressure (n = 10) may be a limitation, but on the other hand we would not expect these individuals to have sleep apnoea headache, as this headache by definition resolves after treatment of OSA. The diagnostic criteria for sleep apnoea headache are controversial and still lack validation. In the current study we did not verify criterion D of ICHD II, which implies rapid resolution of the headache after effective treatment of sleep apnoea (7). This criterion of the secondary headaches has made it impossible to provide a definitive diagnosis until the underlying cause has been resolved and is subsequently of no help in guiding treatment in clinical practice. Because of this shortcoming of the diagnostic criteria of secondary headaches, it is proposed that this criterion be removed in a revised edition of ICHD, entitled ICHD IIR (34).
Conclusion
Morning headaches were significantly more frequent among participants with OSA as compared to those without. This relationship remained significant even after adjusting for potential confounders. However, sleep apnoea headache appeared to be not as common in a population-based sample of OSA as had previously been reported in clinician-driven studies. Furthermore the importance of hypoxia is questioned.
Footnotes
Authors’ contribution
KJK and MBR designed the project. HAK collected data and drafted the manuscript. All authors contributed to the manuscript with critical revisions and suggestions. All authors approved the manuscript.
Acknowledgements
The Institute of Clinical Medicine, Campus Akershus University Hospital kindly provided technical support. Thanks to Akershus University Hospital for providing research facilities.
Funding
This study was supported by a grant from South-East Norway Regional Health Authority, grant number 2004219.
Declaration of conflicting interests
None declared.