
Abstract
The purpose of this clinic-based study was the assessment of symptoms of depression, anxiety, and non-specific psychiatric disorders amongst patients with migraine, compared with healthy subjects and with individuals with a non-neurological chronic disease. A cross-sectional study was carried out in which 178 individuals (migraine 51; psoriasis 35; healthy 92) were submitted to three scales: MADRS (depression), STAI-T (anxiety) and SRQ (screening for mental disorders). The subjects with migraine and psoriasis were from the Out-patient Clinics of Headache and of Dermatology, and the healthy volunteers were persons who were accompanying out-patients in the same hospital. Scores were analysed by MANOVA and by association analysis and logistic regression. Scores of all instruments were higher in the migrainous group, but the univariate analysis of association (using cut-offs) showed significance only for suspicion of mental disorders (SRQ). By logistic regression, variables with strongest association to migraine were gender, education, and SRQ in decreasing order.
Introduction
The relationship between migraine and psychopathology has been discussed far more often than it has been systematically studied (1, 2). Until the late 1980s, twentieth-century investigators described the rigid, obsessional, angry personality postulated to characterize migraine sufferers (3–6). More recently, community and population-based studies have demonstrated association between migraine and specific personality characteristics (7–9) and between migraine, depression and panic disorder (10–13).
The idea of migraine association to some specific personality features and psychiatric disorders first grew out of clinical observations of the highly selected patients seen in subspecialty clinics (3–6, 14–19). Nonetheless, controlled studies are essential because migraine is a common condition and coincidental associations are likely. A more subtle problem may arise because of patterns of referral and methods of identifying cases. Some clinic-based studies (e.g. case series, personal opinions, and naturalistic observations of antidepressants’ effects) (20–22) presented important methodological pitfalls that compromised their internal and external validity. The association between migraine and psychiatric disorders has been investigated systematically only recently in clinical and community samples (23–33) and some population-based studies have examined the co-morbidity of migraine, major depression, panic disorder and other psychiatric disorders (12, 13, 34).
Previous interpretations of the more specific association between migraine and depression have preferred the shared mechanisms explanation, based on studies on biological markers (dexamethasone suppression, tyramine sulfoconjugation, 3H-imipramine platelet binding) (35–39), observations regarding tricyclic and monoamine oxidase inhibiting antidepressant efficacy in both disorders, and evidence suggesting that dysfunction in serotoninergic and adrenergic neurotransmitter systems might be involved in both (40–42). Higher allelic variation of the human serotonin transporter gene in migraine and major depression patients has been reported (43, 44). This association, for an obvious candidate gene, has provided a critical starting point for an understanding of the likely polygenic contributions towards susceptibility to migraine and to affective disorder.
Community-based studies from Breslau and collaborators (11, 33, 45, 46) and from Merikangas and collaborators (8, 10) and population-based studies from Stewart and collaborators (12, 13) provided a solid basis to the current concept of co-morbidity of migraine, depression, and anxiety disorders. These studies have, respectively, evidenced: (i) increased relative risk among migraineurs for affective and anxiety disorders, suicide ideation and nicotine, alcohol or illicit drugs dependence; (ii) higher odds ratio (OR) for major depression among migraineurs and higher OR for migraine among major depression subjects; (iii) higher occurrence of previous migraine attacks and more medical consultations due to headache among individuals with panic attacks, and increased OR for depression, bipolar disease, generalized anxiety, panic, simple phobia, and social phobia.
The purpose of the present study was to analyse the variability and the association of symptoms of depression, anxiety and non-specific psychiatric disorders (screening for mental disorders) in migrainous patients from an out-patient headache clinic, controlling for the condition of chronic disorder.
Patients and methods
Study design
A cross-sectional study was developed to test the hypothesis of association of migraine and symptoms of depression/anxiety, and positive identification in a screening test for mental disorders. The study comprised subsamples of subjects grouped by the main factor under evaluation (migraine, psoriasis, and healthy). The study was developed at the University Hospital Neurology Service (tertiary facility), after being approved by the local Research Ethics Committee. All subjects under study signed an informed consent form after the nature of all procedures was fully explained and they were enrolled in the study.
Subjects
The sample comprised subjects belonging to three groups: (i) Migraine: patients from the Headache Out-patient Clinic of the Neurology Service with diagnosis of migraine without aura, migraine with aura or migrainous disorder, according to the International Headache Society (IHS) criteria (47); (ii) Psoriasis: patients with the diagnosis of psoriasis enrolled in the same hospital Dermatology Service out-patient clinic; (iii) Healthy Volunteers: individuals who were escorting patients to any of the same hospital out-patient clinics were recruited, as far as they had no history, symptoms, or signs of migraine or psoriasis according to specific inquiry and inspection.
Instruments
The instruments applied by the research team members were (i) SRQ (Self-report Questionnaire): a screening scale designed to detect cases of mental disorder (48), previously studied in Brazil (49) with cut-off validation (50). Only the first part of the scale, comprising 20 questions on neurotic symptoms, was used in the study. Its score ranges from 0 to 20 and the cut-off is 8 (50–53). We also analysed the instrument by eliminating three questions regarding symptoms that can be part of migraine attacks (‘headaches’, ‘digestive problems’ and ‘stomach unpleasant sensations’) since they could explain differences of SRQ-20 scores between migraine and the other groups. This variant was named SRQ-17 (see Results); (ii) MADRS (Montgomery-Åsberg Depression Rating Scale): a scale designed to rate symptoms of depression (54), previously validated for the Brazilian adult population (55, 56). Its score ranges from 0 to 60 (the higher the score, the higher the depressive symptomatology). The cut-off for the identification of very mild levels of depressive symptoms is 10 (57); (iii) STAI (State-Trait Anxiety Inventory): this scale is probably amongst the most widely used self-report measures of anxiety in clinical and research settings. Spielberger (58) developed the STAI as a self-report scale measuring two separate components: state anxiety, which refers to a transitory emotional state characterized by subjective feelings of tension that may vary in intensity over time, and trait anxiety, which refers to a relatively stable disposition to respond to stress with anxiety and a tendency to perceive a wider range of situations as threatening. The Portuguese language version of STAI's trait form (STAI-T), validated in Brazil by Biaggio and Natalício (59), was used. Its score ranges from 20 to 80 (the higher the score, the worse the symptoms of anxiety). Although some studies utilized 50 (60) or 1 SD above the group mean (61) as the cut-off value for high trait anxiety, we preferred to adopt the more conservative value of 59.
Sample characteristics
One hundred and seventy-eight subjects (51 with migraine, 35 with psoriasis, and 92 healthy volunteers) constituted the sample. Table 1 shows the three groups’ demographic data distribution and Table 2 shows the frequency of migraine types amongst migraine patients. Medications in use by the subjects at the time of study are presented in Table 3.
Demographic variables
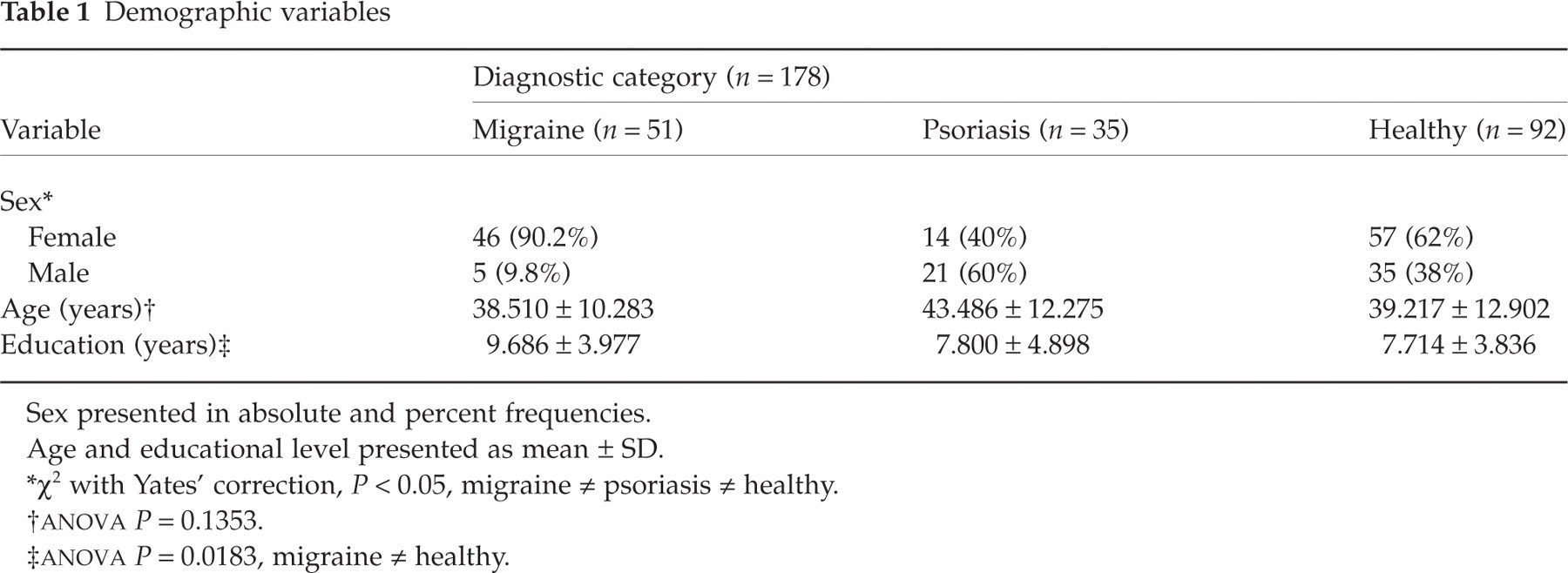
Sex presented in absolute and percent frequencies. Age and educational level presented as mean ± SD.
∗χ2 with Yates’ correction, P < 0.05, migraine ≠ psoriasis ≠ healthy.
†
‡
Frequency of migraine types

Medications in use at the time of the interview

Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS-PC Plus) software (62). The parametric data (age and education) were analysed by one-way
Results
The multivariate analysis by
Mean scores from the scales (

Results presented as mean ± SD. CI 95%, confidence interval 95%; N1, level 1 (group 1 × group 2); N2, level 2 (groups 1, 2 × group 3); STAI-T, State-trait Anxiety Inventory; MADRS, Montgomery-Åsberg Depression Rating Scale; SRQ-20, Self-Report Questionnaire – 20 questions form; SRQ-17, Self-Report Questionnaire – 17 questions form.
∗Coefficients of comparison between each two levels of the factor.
The other potential confounding variables (age and education) were analysed by covariance of
Correlation coefficients (B and Beta) of co-variants age and educational level in relation to the scales (

After application of cut-offs, frequency of subjects classified through this method was obtained (Table 6). Thirty-six percent of migraine patients (n = 18) had a positive result in the screening test for mental disorders, while amongst patients with psoriasis and healthy volunteers the values were 12.1% and 11.1%, respectively.
Distribution of subjects in the three groups according to scales cut-off values

Results from the three SRQ-20 questions described above were submitted to χ2 test (Table 7). As expected, presence of headache (question 1) was significantly different between migraine and psoriasis (χ2 = 29.515, P = 0.000), and between migraine and healthy volunteers (χ2 = 82.621, P = 0.000). Nevertheless, the occurrence of digestive problems (question 7) and stomach unpleasant sensations (question 19) were not different between migraine and psoriasis (χ2 = 0.000, P = 1.000; χ2 = 3.411, P = 0.065, respectively), and between migraine and volunteers (χ2 = 1.337, P = 0.248; χ2 = 2.105, P = 0.147, respectively).
Frequency of Yes/No answers to SRQ questions 1, 7 and 19 in the three groups

Higher rates of headache (question 1) were also observed in the psoriasis group compared with the healthy volunteers group (χ2 = 5.636, P = 0.018), but no differences were detected for questions 7 (χ2 = 1.121, P = 0.290) and 19 (χ2 = 0.461, P = 0.497).
Univariate analysis of association among scales and diagnostic groups
The comparison between migraine and psoriasis groups did not show significant association for the presence of mild to severe depressive symptoms (χ2 = 2.012; P = 0.156), nor for mental disorders by SRQ-17 (χ2 = 3.336; P = 0.068) or anxiety trait (χ2 = 3.096; P = 0.079). Nevertheless, there was a significant association (χ2 = 4.658; P = 0.031) for suspicion of mental disorders by SRQ-20.
Analysis between migraine and healthy volunteers groups did not evidence association for presence of depressive symptoms (χ2 = 2.168; P = 0.141), nor for anxiety trait (χ2 = 2.974; P = 0.085). However, both SRQ-20 and SRQ-17 revealed more positive individuals for suspicion of mental disorders among migraineurs than among healthy volunteers (χ2 = 10.938; P = 0.001 and χ2 = 8.508; P = 0.004, respectively).
The univariate analysis of association between psoriasis patients and healthy volunteers showed no association with depressive symptoms (χ2 = 0.038; P = 0.846), anxiety trait (χ2 = 0.148; P = 0.701) or suspicion of mental disorders (χ2 = 0.000; P = 1.000 in both SRQ-20 and SRQ-17).
Multivariate analysis of association (logistic regression)
The first set of analyses was done considering positivity on psychiatric scales as the dependent variable. The association to the presence of symptoms of depression (MADRS) was tested by logistic regression in order to observe the weight of the variables sex, age, and education, simultaneously to diagnosis. The cut-off 10 separated individuals with almost no symptoms from those with mild to severe symptoms, and this classification was taken as the outcome. The final model included only the variable age (Table 8). The same procedure was used for suspicion of mental disorders (SRQ-20) through the application of 8 as the cut-off value for outcome definition (Table 8). The final model maintained the variables diagnosis and education to explain the outcome. In the analysis for anxiety trait (STAI), the cut-off value was 59 and the final model kept the variables sex and education (Table 8).
Regression coefficients, Wald and significance of independent variables maintained in the final models of the analysis for depressive symptoms (MADRS), mental disorders (SRQ-20) and anxiety trait (STAI-T)

∗Diagnosis (1) = migraine (1); psoriasis (0); healthy (−1).
†Diagnosis (2) = migraine (0); psoriasis (1); healthy (−1).
Migraine was regarded as the dependent variable in the second part of multivariate analysis, and it was analysed as the outcome through a logistic regression model in a three-step (or three-level) analysis by changing the comparison group and, consequently, the potential exposure to the independent variables. In the first step, migrainous patients were compared with healthy volunteers. The weight of the variables age, sex, educational level, depressive symptoms (MADRS), anxiety symptoms (STAI) and general psychiatric symptoms (SRQ-20) were included in the model as independent variables. The final model has maintained sex, education, general psychiatric symptoms (SRQ-20) and anxiety symptoms (Table 9). In the second step, migrainous patients were compared with healthy volunteers and psoriasis patients together. Variables age, sex, education, depressive symptoms (MADRS), anxiety symptoms (STAI) and general psychiatric symptoms (SRQ-20) were included in the model as independent variables. The final model included sex, schooling, general psychiatric symptoms (SRQ-20) and anxiety symptoms (Table 9). In the third step, migrainous patients were compared with psoriasis patients with the same procedure and the final model has kept the variables sex and depressive symptoms (Table 9).
Regression coefficients, Wald and significance of independent variables maintained in the final models of the analysis for Migraine group in relation to Psoriasis and Healthy groups

∗Migraine × healthy.
†Migraine × psoriasis and healthy.
‡Migraine × psoriasis.
Use of medications by migrainous patients
The effect of continuous medication use on the scores was assessed in the migraine group. As seen in Table 3, migraineurs were highly dispersed in the various categories of medications, either in an isolated form or in combinations, precluding an adequate evaluation. So a new division was created with one group including all those who were using some prophylactic anti-migraine drug (n = 26) and another group with the remaining migraineurs (n = 25). No significant difference was observed between the scores of these two subgroups (Table 10).
Mean and standard deviation of the scales scores in migraine subjects in relation to chronic use of systemic medication and

Discussion
The present study aimed to evaluate symptoms of depression, anxiety, and general psychiatric symptoms among migraine patients, compared with a group of patients suffering from another chronic medical illness without neurological or psychiatric impairment, and with a group of healthy volunteers. Statistical differences in the score of scales (depression, anxiety, and general psychiatric symptoms) were observed between migraine sufferers and the other groups. However, no association (i.e. the distribution of persons within categories and between groups) of presence of moderate to severe symptoms of depression and anxiety with migraine was found. On the other hand, a higher frequency of positive patients screened for mental disorders (general psychiatric symptoms) was observed among migraineurs than among psoriasis patients and healthy volunteers. Despite this apparent discrepancy, such results were not contradictory, since extreme values within a group might strongly influence variability, even if such values correspond to few persons in the group. In contrast, the use of cut-off points for the association analysis allocates individuals in distinct categories, eliminating the influence of extreme values. However, the number of subjects identified within one and another category is determinant. Thus, the migraine group showed high average rates of depressive symptoms, while the psoriasis and healthy groups did not. Nonetheless, the number of migraineurs classified above the cut-off was not enough to promote the association.
The instrument for depressive symptoms used in our study (MADRS) is a rating scale that evaluates current depression symptomatology; it is not a major depression diagnostic tool. Major depression diagnosis requires the assessment of additional clinical features besides those measured by the scale (e.g. duration of symptoms). The observed association between SRQ and migraine might express a relation to non-specific psychiatric diagnosis, since SRQ-20 is a screening tool for general psychiatric diagnosis with adequate detection values (48, 50, 51), and may be interpreted as an indirect relation to the frequently associated diagnoses (depression, anxiety and panic disorders) (2, 8, 10–13, 33, 46, 66–68). Exclusion of the three potentially misleading questions from the scale did not affect the findings.
As described above, STAI is a widely employed self-report anxiety symptoms scale, and its trait component refers to a relatively stable pattern of enhanced anxiety response to stressing situations (58, 69). As the depression rating scale used in this study, STAI-T refers to symptoms and may not fulfil diagnostic criteria for anxiety disorders. Similarly, a few migraine patients may have presented very high STAI-T scores allowing the significant difference with the other groups, but these patients were not enough to associate STAI-T positivity with migraine when cut-offs were applied.
The logistic regression analysis showed how many different variables associate simultaneously, and to what degree, to migraine. The three-step comparison of migraineurs to psoriasis patients and healthy volunteers disclosed sex as the variable of higher association, followed by educational level, general psychiatric symptoms, and anxiety trait. In any clinical research setting, higher methodological concerns on the sampling process warrant greater validity of results. The presence of 90% of women in the migraine group in the present study is certainly related to the process of search and selection, but it also expresses the difference in the prevalence of migraine between sexes (70). Male members of the migraine group were very few (n = 5), while in psoriasis and healthy groups men represented 60% and 38% of the sample, respectively. Although all statistical analyses were carried out with control of this confounding, logistic regression findings expressed the sex distribution within subsamples. Similarly, the association between higher education and migraine could have been a consequence of the sampling process. As patients were allocated from a university hospital out-patient clinic (tertiary health care level), it may be expected that subjects would have their origin from a higher than average socio-economic stratum. Consequently, educational attainment may also be higher than that of the general population, and perhaps this characteristic was not neutralized by the selection of individuals of the same origin for the comparison groups. Breslau and co-workers (33) observed a relation of low educational level with migraine in a community sample of migraineurs. However, only a small subgroup of 37 subjects (total sample n= 1007) showed an educational level lower than college, of which only eight presented migraine (from 177 migraineurs identified in the total sample). The number of individuals in this subgroup seems to be very small to sustain the alleged strength of the observed association. This matter should be addressed in the future as a study's main objective, with a population with greater variability of educational level. In the present study, the migraine set showed an average schooling higher than that of the other groups, and a very small subgroup of lower education among migraineurs was identified which may have influenced some results. The findings of the general psychiatric symptoms scale (SRQ) were similar to both the logistic regression and the univariate analysis of association. Anxiety trait (STAI-T) was not associated with migraine by univariate analysis, but was kept in the final model through logistic regression, and this may be one of the aspects related to the low education subgroup within the migraine patients group cited above.
Sex and depressive scores (MADRS) showed significant association for the outcome migraine/psoriasis, but sex presented a higher coefficient. In such a condition, depressive symptoms appeared related to migraine, and suspicion of mental disorders was no longer significant.
In non-populational studies like the present one, the small number of subjects in subgroups and the fact that they are less representative may cause a type II statistical error (β-type error), when discrete existing associations are not detected (71, 72). In spite of these considerations, Merikangas (71) argues that patients from out-patient clinics are more thoroughly evaluated than those who are enrolled in populational studies. Furthermore, the present study displayed methodological characteristics that differentiate it from the previous clinic-based ones, such as the use of healthy volunteers (unexposed group) and of patients with a chronic disease – psoriasis – without neurological or psychiatric damage that affects young people (intermediate exposition group), in addition to the application of the IHS criteria (47) for migraine diagnosis (exposed group).
The inclusion of the psoriasis group was an attempt to refute the argument that, in case of a significant association of the addressed symptoms with migraine, this association would have occurred simply because of the presence of a chronic disorder. The fact that psoriasis has been traditionally classified among the ‘psychosomatic disorders’ would increase the probability of its association with psychiatric symptoms. Therefore, such a procedure has increased the reliability of the positive results (association between migraine and psychiatric symptoms).
Our migraine sample consisted of 27% of people with migrainous disorder (IHS 1.7). This subsample did not meet IHS criteria for migraine with or without aura because duration of migraine attacks was not 4–72 h. According to a review on the diagnostic value of historical features in primary headaches (73), the most specific features for migraine are nausea, phonophobia, photophobia and exacerbation by physical activity (positive likelihood ratios of 19.2, 5.2, 5.8 and 3.7, respectively). If we accept that duration is a less specific migraine characteristic and that it was responsible for the migrainous disorder diagnosis in this subgroup, we can assume that these subjects present true migraine syndrome and might consequently have little or no impact on the findings. On the other hand, clinic samples may present more severe and less defined cases. This can be seen in some published series where, for example, 21.73% of the patients met criteria for migrainous disorder (IHS 1.7) (74); 37.7% of the patients suffered from chronic daily headache (75) and 35.9% had received a diagnosis of migrainous disorder (IHS 1.7) or headache of the tension-type not fulfilling the above criteria (IHS 2.3) (76).
It is important to stress that these groups could not be assumed as representative of either migraine, psoriasis or healthy individuals of the state or country populations. Nevertheless, our study did not aim to evaluate clinical characteristics that are pertinent to populations (e.g. prevalence), which would require a completely different design. Our purpose was the assessment of features that have been described as occurring at higher frequency among migraineurs than in other groups. This is an important point, since high-frequency characteristics of a population tend to present more reliable findings in non-populational samples than low-frequency ones. The ‘Berkson bias’ (77) must be considered, however, because patients from the tertiary health care level, such as the present ones, can have more severe symptoms than individuals with the same disease in the population. Nonetheless, for the evaluation of variability and frequency of psychiatric symptoms between the subsamples, being representative of the population is not imperative.
In conclusion, there was a significant association of general psychiatric symptoms (SRQ, a screening for mental disorders) with migraine through either univariate or multivariate statistical procedures. No association was observed with depressive symptoms. Nevertheless, females and higher educational attainment were more strongly associated with migraine than general psychiatric symptoms (SRQ). On the other hand, association of higher anxiety traits (STAI-T) was observed for the healthy participants that might be attributed to educational level differences between groups.