
Abstract
Enhanced endothelium nitric oxide (NO) and superoxide anion release may cause migraine through related cerebral blood flow changes. Thirty subjects suffering from migraine with and without aura and 20 healthy controls were investigated. Urine samples collected for 24 h during and after the migraine attack, and during the headache-free period, were assayed for urinary NO stable metabolites (NOx) and thiobarbituric acid reactive substances (TBARS). During the headache-free period urinary NOx and TBARS levels were higher in migraine sufferers than in controls (NOx 0.77 ± 0.14 vs. 0.28 ± 0.15 mmol/mmol creatinine, P < 0.05; TBARS 0.40 ± 0.19 vs. 0.26 ± 0.13 μmol/mol creatinine, P < 0.05). Also, NOx excretion was higher during the headache-free period than during or after the migraine attack (P < 0.05). Urinary TBARS were increased during the attack with respect to the headache-free period (P < 0.05). No differences were observed in the same parameters between sufferers of migraine with and without aura. Urinary NOx and TBARS might be promising as markers of their systemic levels to evaluate the increased vulnerability to oxidative stress in migraine sufferers.
Introduction
Sterile neurogenic inflammation due to trigeminal ganglion release of neuropeptides (1, 2) and plasma protein extravasation in the dura mater, although involved in the pathogenesis of migraine, are only partially responsible for head pain (3–6). Also, vasodilation of cerebral vessels and sensitization of perivascular sensory nerves may represent nitric oxide (NO)-mediated phenomena (6–8).
NO may function as a signalling molecule in controlling neuronal activity (9) and as a major nonadrenergic, noncholinergic neurotransmitter (10). This short-lived free radical is responsible for cerebral blood vessel relaxation activating guanylate-cyclase and increasing cyclic guanosine monophosphate in smooth muscle (11). NO is crucial in controlling signal-to-noise sensory inputs during migraine attack and, interacting with oxygen free radicals, may cause the headache through variations of cerebral blood flow (5, 12, 13).
Recently an association between decreased cerebral blood flow and NO bioavailability with increased levels of superoxide and peroxynitrite during glyceryl trinitrate infusion, usually precipitating the onset of migraine, has been proposed (14). Regional changes of cerebral blood flow may enhance release and formation of an excess of oxygen free radicals overcoming the operative defences, thus causing increased plasma accumulation of lipid peroxidation by-products (15, 16), explaining the enhanced vulnerability to oxidative stress of migraine sufferers (17).
In this study we investigated in vivo variations of NO metabolites and oxidative markers in urine, to provide a non-invasive assessment of these parameters during the migraine attack and the headache-free period.
Methods
Thirty subjects, 22 women and eight men (mean age ± SD: 35 ± 15 years) suffering from migraine with (n = 12) and without (n = 18) aura were assessed during the migraine attack, immediately after, and during the headache-free period. Mean duration of migraine attack was 16 ± 12 h. Migraine with or without aura was diagnosed according to the criteria of the Headache Classification Committee of the International Headache Society (18). All subjects were non-smokers, free of any cardiovascular, neurological, psychiatric, and coagulation disease and none of them was under any preventive headache treatment before the testing session. In women urine collection was not performed during the menstrual cycle. Twenty healthy subjects, 10 women and 10 men (mean age ± SD: 35 ± 10 years) represented the control group. All participants to the study were carefully instructed to avoid any nitrite/nitrate-enriched diet for at least 4 days before assessment (19). The nature of the study was explained to all participants, who gave their informed consent.
Urinary samples were collected every 6 h throughout a 24-h period: the first urine collection was performed during the index attack, the second was performed during the day following the attack, and the third, at random, during the headache-free period. The headache-free period was defined as the portion of time, lasting>72 h, separating two different migraine attacks.
Urinary samples were ultrafiltered and centrifuged at 14 000 r.p.m. for 15 min to remove substances larger than 10 kD and to separate precipitates (Ultrafree MC microcentrifuge device; Millipore Corp., Bedford, MA, USA). Samples were enriched with 0.02% butylhydroxytoluene (BHT) to inhibit spontaneous oxidation and were stored at −80°C before analyses.
Determination of urinary NO stable nitrite/nitrate metabolites (NOx)
NO is a free radical rapidly decomposed to nitrite and nitrate (NOx). NOx were measured by reducing nitrate to nitrite by the action of nitrate reductase from Aspergillus niger (20) and measuring nitrite by a sensitive fluorimetric assay based on the reaction of nitrite with 2,3-diaminonaphthalene to form the fluorescent product 1-(H)-naphthotriazole (21). Intensity of the fluorescent signal of the samples was measured and compared with known concentrations of sodium nitrite (excitation wavelength 375 nm, emission wavelength 415 nm). The fluorimetric assay was able to detect amounts in the order of 30 n
NOx corrected by creatinine excretion were expressed as mmol/mmol creatinine. Urinary creatinine was evaluated using a commercial assay kit (Sigma-Aldrich Fine Chemicals, St Louis, MO, USA) based on the reaction of creatinine with picric acid under alkaline conditions.
Determination of urinary thiobarbituric acid reactive substance
Lipid peroxidation was measured in urine using the thiobarbituric acid (TBA) assay which detected thiobarbituric acid reactive substance (TBARS) generated by peroxidative process, including lipid peroxides and malondialdehyde. Urinary TBA products were formed at pH 2.5 by heating 1 ml urine with TBA reagent at 100°C, for 30 min (22). Determination of TBARS was carried out fluorimetrically (excitation wavelength 510 nm, emission wavelength 553 nm); the quantitative evaluation was made using a standard curve obtained from a stock solution of 10 m
Statistical analysis
Values of urinary NOx and TBARS of migraine sufferers and controls were expressed as means ± SD. Student's unpaired t-test was used to determine the statistical significance of NOx and TBARS differences between migraine sufferers and controls and between patients suffering from migraine with and without aura. Repeated measures
Results
In sufferers from migraine with and without aura, urinary NOx levels, assessed during the headache-free period, were higher than in controls (0.77 ± 0.14 vs. 0.28 ± 0.15 mmol/mmol creatinine; P < 0.05), as well as TBARS, with respect to the same controls (0.40 ± 0.19 vs. 0.26 ± 0.13 µmol/mol creatinine; P < 0.05).
As shown in Fig. 1, NOx urinary levels fell significantly during the migraine attack compared with levels measured during the headache-free period; after the attack urinary NOx levels slightly increased in all migraine sufferers even if levels were significantly lower than those measured during the headache-free period (P < 0.05;
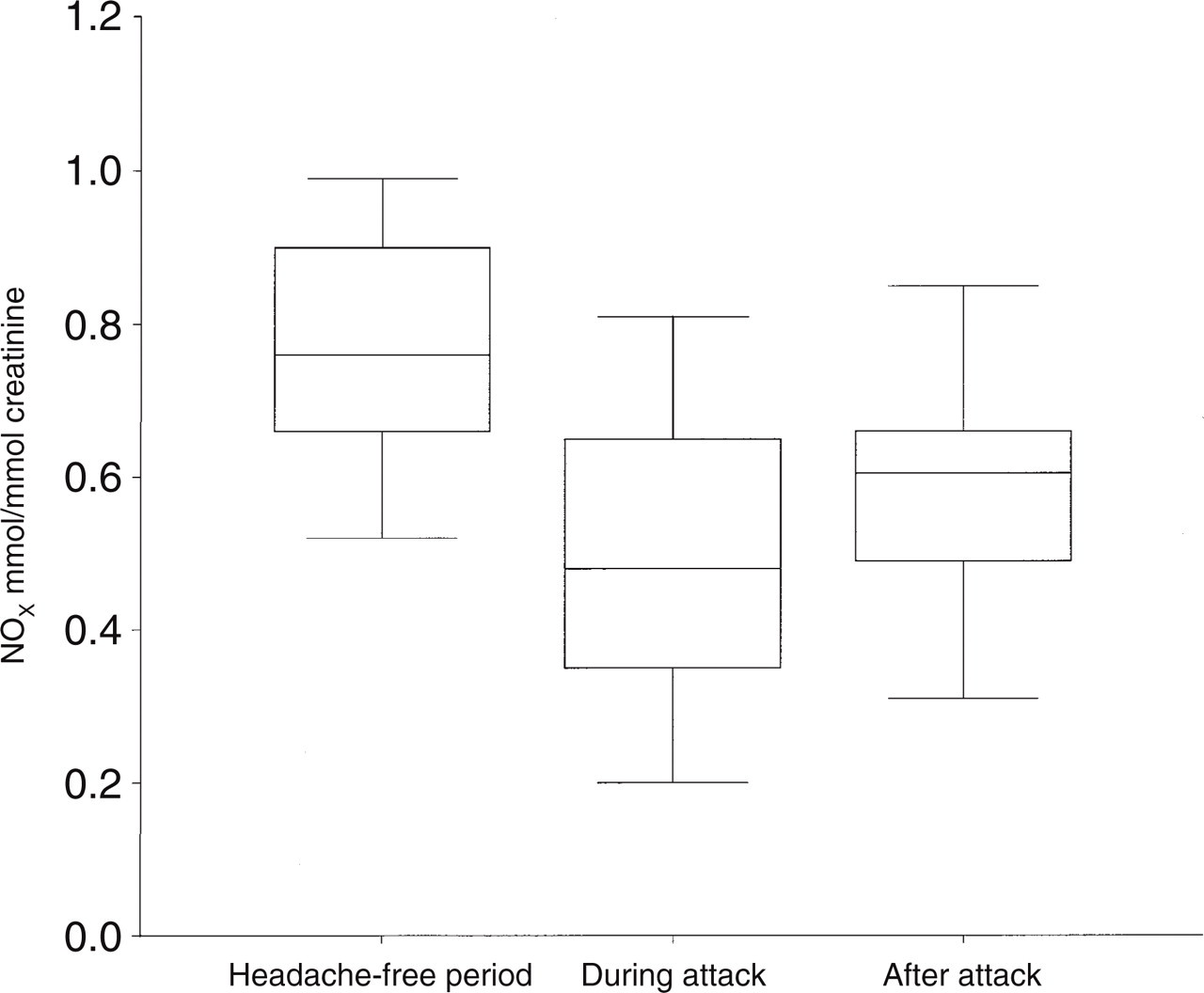
NO stable metabolite (NOx) urinary levels measured during the headache-free period, and during and after the migraine attack.
No differences were found in NOx values between subjects suffering from migraine with and without aura measured during and after the attack, and during the headache-free period (Student's unpaired t-test).
As shown in Fig. 2, TBARS values during the attack were higher than those measured after the attack and during the headache-free period (P < 0.05;

Thiobarbituric acid reactive substance (TBARS) urinary levels measured during the headache-free period, and during and after the migraine attack.
No differences were observed between subjects suffering from migraine with and without aura in TBARS levels measured during the headache-free period, and during and after the attack (Student's unpaired t-test).
Discussion
Haemodynamic changes during the migraine attack may depend on alterations in the activity of vascular NO, synthesized by endothelial cell membrane deformation when vascular shear stress increases (12, 23). A sudden migraine-related increase in pulsatile cerebral blood flow may increase shear stress (24) with formation of endogenous vascular NO.
The role of NO in migraine is not definitely established. So far, conflicting results are reported. Recent data exclude any significant alteration of blood NO after the attack, in migraine patients compared with controls (25). Other data showed an activation of the L-arginine–NO pathway which accompanied the release of vasoactive peptides from the trigeminal endings, thus favouring the maintenance of the migraine attack (26).
In our study, urinary NOx and TBARS levels were higher in migraine sufferers during the headache-free period than in healthy subjects. The observed higher values of urinary NOx support biochemical changes in the L-arginine–NO pathway ictally and interictally, in migraine sufferers (26, 27). During the headache-free period, urinary NOx levels were higher than during and after the attack, suggesting that plasma NO bioavailability might be reduced during the attack. In fact, plasma NO may be inactivated by superoxide anions: an increase in the vascular production of superoxide anions leads to decreased levels of NO via a fast radical/radical reaction occurring more rapidly than the reaction of superoxide anions with superoxide dismutase, a specific enzyme able to dismutase superoxide anions (28). Besides, in the presence of reactive oxygen radicals, NO may act as an antioxidant, avoiding alkyl peroxide-mediated cytotoxicity (29).
Migraine sufferers were vulnerable to the toxic effects of TBARS and NO; besides, NO reacting with superoxide anions may induce the formation of peroxynitrite, thus contributing to vascular relaxation. Thus, the interaction between NO and TBARS, indices of lipid peroxidation, may contribute to alter endothelium regulation of vasomotion (30) and may determine the migraine-related cerebral blood flow changes (5). Simultaneous release of NO and of superoxide anions determine an oxidative status (31), depending on individual susceptibility to oxidative reactions and on its capability to eliminate lipid peroxidation by-products via breath and urine (22).
Free radicals are usually removed or scavenged by endogenous antioxidants. However, when free radicals overwhelm the operative protective mechanisms, the oxidative reactions induced by their high reactivity lead to the formation of peroxidative by-products metabolized and cleared into urine (31). As a consequence, urinary concentrations of NO stable metabolites and of peroxidative by-products such as TBARS are good indexes of their plasma levels and sensitive indicators of plasma NO and TBARS bioavailability (22, 32).
As suggested by our findings, urinary levels of NO and TBARS might help to detect changes in oxidative stress in migraine sufferers. As a corollary, reducing the overproduction of oxygen free radicals, by enhancing endogenous protective antioxidant mechanisms, might help to disclose new treatments for migraine.