
Abstract
To carry out a systematic review of the literature examining the effectiveness of spinal manipulation for the treatment of headache disorders, computerized literature searches were carried out in Medline, Embase, Amed and CISCOM. Studies were included only if they were randomized trials of (any type of) spinal manipulation for (any type of) headache in human patients in which spinal manipulation was compared either to no treatment, usual medical care, a ‘sham’ intervention, or to some other active treatment. Two investigators independently extracted data on study design, sample size and characteristics, type of intervention, type of control/comparison, direction and nature of the outcome(s). Methodological quality of the trials was also assessed using the Jadad scale. Eight trials were identified that met our inclusion criteria. Three examined tension-type headaches, three migraine, one ‘cervicogenic’ headache, and one ‘spondylogenic’ chronic headache. In two studies, patients receiving spinal manipulation showed comparable improvements in migraine and tension headaches compared to drug treatment. In the 4 studies employing some ‘sham’ interventions (e.g. laser light therapy), results were less conclusive with 2 studies showing a benefit for manipulation and 2 studies failing to find such an effect. Considerable methodological limitations were observed in most trials, the principal one being inadequate control for nonspecific (placebo) effects. Despite claims that spinal manipulation is an effective treatment for headache, the data available to date do not support such definitive conclusions. It is unclear to what extent the observed treatment effects can be explained by manipulation or by nonspecific factors (e.g. of personal attention, patient expectation). Whether manipulation produces any long-term changes in these conditions is also uncertain. Future studies should address these two crucial questions and overcome the methodological limitations of previous trials.
Introduction
Headache disorders are one of the most common problems seen in medical practice. Population based studies suggest one-year prevalence rates for episodic tension-type headaches of 38.3% and for chronic tension headache of 2.2% (1). In Western countries, one-year prevalence rates for migraine range from 10 to 12% (2). Headache sufferers are also frequent users of complementary-alternative medicine (CAM) with relaxation therapies and chiropractic care being the most common CAM therapies employed (3). Chiropractors themselves report high rates of treatment for headache disorders. A study conducted by the National Board of Chiropractic Examiners found that most chiropractors see patients for headaches in their clinical practice on a daily basis (4).
While there is considerable evidence—based on meta-analyses and systematic reviews of randomized controlled trials (5–7)—that various mind-body/behavioural strategies (e.g. relaxation and biofeedback) can be effective treatments for headache disorders, the evidence for chiropractic spinal manipulation is less clear. Although nonsystematic reviews (8) have suggested that headache disorders respond well to spinal manipulation, there have been no systematic reviews to support these claims. We therefore carried out such a review, specifically focusing on randomized controlled trials of spinal manipulation (chiropractic or otherwise) for the treatment of any type of headache disorder (e.g. migraine, tension, cervicogenic).
Method
A comprehensive literature search was carried out to identify randomized controlled trials of spinal manipulation in the treatment of any type of headache. The MEDLINE, Embase, PSYCHLIT, CAMPAIN, Science Citation Index, Amed, CISCOM, and Cochrane Library databases (including the Cochrane Registry of randomized trials) were searched from their inception to March 2001. We also hand-searched our own files and the reference sections of identified trials and review articles for additional studies. Criteria for inclusion were as follows:
Random assignment of human subjects;
Comparison of spinal manipulation to either a no treatment control, ‘sham’ intervention, usual medical care, and/or some active treatment;
Publication in a peer-reviewed journal (i.e. excluding abstracts, conference proceedings, dissertations).
Dual or overlapping publications were excluded. If such studies were found, the trial with the larger sample size was used. No restrictions as to the language of publication were applied. Data were extracted and validated independently by both authors according to predefined criteria (Table 1). The methodological quality of the trials was assessed using criteria outlined by Jadad et al. (9).
Study outcomes

Results
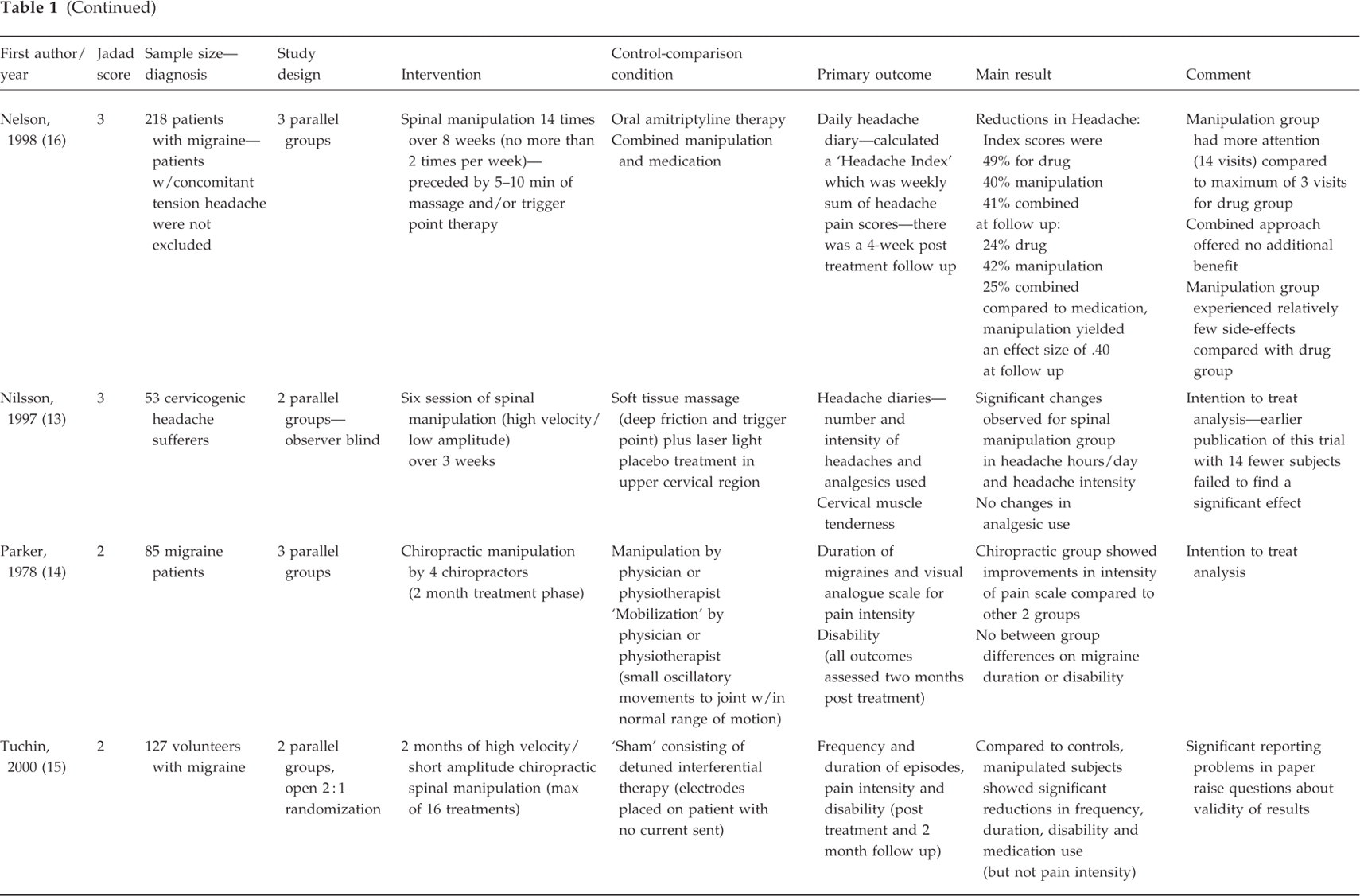
We identified 9 randomized controlled trials that examined the efficacy of spinal manipulation for any headache disorder (10–17). Three studies explored the effectiveness of spinal manipulation in the treatment of tension headaches (10–12); three examined the effectiveness of manipulation for migraine (14–16); two papers examined spinal manipulation for cervicogenic headache (13, 18). These two were overlapping publications (i.e. involved data from the same trial), therefore we used the latter publication that included data from 14 additional subjects. One trial was found for ‘headaches of spinal origin.’ (17) Study characteristics are summarized in Table 1.
Owing to the small number of trials, study heterogeneity (particularly in terms of differences in the nature of the control/comparison conditions), and the lack of data to calculate effect sizes in a number of trials, we did not carry out a formal meta-analysis.
Mean sample size across trials was 91 (overall n=760). Seven trials tested the effectiveness of chiropractic spinal manipulation while one study (12) examined osteopathic manipulation. In most instances, spinal manipulation involved what the authors described as ‘low-amplitude, high velocity thrusts’ in which the vertebrae were carried ‘beyond the normal physiologic range of movement without exceeding the boundaries of anatomic integrity.’ (15). In some studies, practitioners were instructed to focus their manipulation efforts on the cervical region of the spine but were free to manipulate any area of the spine they determined by palpation to be clinically relevant; in other studies manipulation occurred only along the cervical region of the spine. With the one exception of a trial in which the entire treatment appears to have lasted only 10 min (12), interventions averaged approximately 6 weeks in length with an average of 10 treatment sessions.
We assessed methodological quality using the scale developed by Jadad et al. (9) The mean score across the 8 trials was 2.3 (out of a maximum of 5) suggesting fairly low quality overall. All studies employed random assignment of subjects (an inclusion criteria), 3 of 7 trials described the method of randomization, while 6 of 7 discussed dropouts and withdrawals. In two trials, an adequate method of allocation concealment was used. In two trials a power analysis was performed. And in three trials, the assessors were described as being blind to the treatment condition.
The nature of the control/comparison groups also varied considerably across trials. Two studies compared spinal manipulation to drug therapy (amitriptyline); three trials attempted to employ a ‘placebo’ or sham condition (e.g. the use of low power laser treatment to the cervical spine); and, in two trials the control consisted of palpation or ‘mobilization’ (small oscillatory movements) without actual manipulation of the spine. Despite such efforts to control for nonspecific (placebo) effects, no trials were scored on the Jadad scale as ‘double-blinded.’ We note, however, that because it is difficult to blind subjects to group assignment in studies of manipulative therapies, such trials will frequently receive lower scores on quality rating inventories such as the Jadad scale.
Among the studies that examined migraine headache, Nelson et al. (16) found comparable improvements in a composite headache index between spinal manipulation (49%), amitriptyline (40%) and the two treatments combined (41%). (It should be noted, however, that the manipulation group had 14 visits compared to 3 visits for the medication group). At four week follow up, there was a non significant trend toward the manipulation group being more likely to have maintained treatment gains compared to the other two groups (effect size of 0.40; P=0.05) compared to drug therapy alone.
Parker et al. (14) found significant improvements in ‘intensity of pain’, but no significant differences in duration of migraines or disability between chiropractic spinal manipulation, physical therapy manipulation or a mobilization ‘placebo’ (all 3 groups showed improvements).
In the most recent study, Tuchin et al. (15) reported that migraine patients receiving spinal manipulation experienced significant reductions in headache frequency and duration, disability, and medication use (but not pain intensity) compared to a ‘placebo’ laser therapy condition. These effects were maintained at two-month follow up. There were, however, considerable methodological and statistical problems with this study that call into question the validity of these findings (see Discussion).
Among trials examining tension headaches, Boline et al. (10) found comparable improvements between spinal manipulation and drug therapy (amitriptyline) at the end of the treatment phase. However, at four-week postintervention follow-up, the manipulation group experienced significantly greater improvement on all outcome measures. Patients in the spinal manipulation group were seen 12 times over six weeks compared with twice overall for the medication group.
More recently, Bove and Nilsson (11) found significant improvements postintervention and at follow up (in headache frequency and analgesic use) in both the manipulation and placebo laser therapy group, but no intergroup differences were noted. In an earlier, smaller trial (n=22), subjects receiving osteopathic spinal manipulation showed significant post treatment reductions in headache pain compared with a control group receiving only ‘palpatory’ examination with no manipulation (12). The treatment in this trial, however, consisted of only one 10-minute session of manipulation, thus it is difficult to gauge the significance of these findings.
In a small three-armed trial, Bitterli et al. (17) found no significant between-group differences between ‘manual therapy’ (according to Maigne (19)) performed by physicians and either ‘sham’ therapy performed by nonphysicians or waiting list (no treatment) control among patients with ‘headache of spinal origin’. Finally, in the one trial examining chiropractic manipulation for the treatment of cervicogenic headaches, Nilsson et al. (13) found significant reductions in headache hours and intensity compared to a ‘placebo’ light control group. As noted, an earlier publication (containing 14 fewer subjects) (18) failed to find a significant treatment effect for manipulation. However, the authors subsequently published the paper in 1997 which included these additional patients and which did find a significant treatment effect.
Discussion
The relatively small number of randomized trials identified (n=8) coupled with a high degree of heterogeneity and small sample sizes in a number of studies, makes it difficult to draw definitive conclusions. Although we included only randomized trials, on average the methodological quality was fairly low, which suggests that there may have been significant bias in a number of the studies. Moreover, the results of our review might have been influenced by the phenomenon of positive publication bias.
Looking across all headache categories, we found that spinal manipulation yielded treatment effects over and above the respective control groups in 4 of 8 studies. In the two studies that compared manipulation to drug therapy, no intergroup differences were observed in one study while the other trial found chiropractic to be superior to drug therapy at follow-up. In the studies that compared manipulation to a ‘sham’ or placebo intervention (e.g. laser light therapy), results were again equivocal with 3 of 6 studies showing significant between group differences.
The most recent of the three migraine trials reported that chiropractic spinal manipulation was superior to a sham condition (detuned interferential therapy) in terms of headache frequency, duration, disability, and medication use (but not pain intensity) (15). However, there were significant methodological and reporting problems in this study that raise questions as to the validity of the findings. For example, closer analysis suggests that the authors did not carry out the appropriate statistical analyses (e.g. they report doing paired t-tests as well as a ‘Oneway
In the earlier trial by Parker (14) that compared manipulation to a ‘mobilization’ placebo, the manipulation group experienced significant improvements on one of three measured outcomes (pain intensity). Finally, in the third and largest of the migraine trials (n=218), Nelson et al. (16) found no differences between migraine and amitriptyline therapy although both groups did demonstrate clinical improvement following treatment. It is therefore not clear whether or not the observed effects of spinal manipulation can be attributed to specific or nonspecific (i.e. placebo) effects.
In the two trials examining chiropractic manipulation for tension headaches, one trial reported that chiropractic manipulation was no better than a ‘sham’ condition, whereas the other trial found manipulation to be superior to amitriptyline therapy at follow up (but not postintervention). Again, the design in this latter study cannot rule out nonspecific effects.
The one study that examined the effectiveness of manipulation for cervicogenic headache did find a significant treatment effect of chiropractic spinal manipulation compared to placebo light therapy suggesting this therapy may be effective for this particular type of headache disorder. Although this diagnostic category remains controversial (20, 21), cervicogenic headaches are, by current definitions, believed to be of neck (or cervical) origin and therefore theoretically more amenable to chiropractic (cervical) manipulation than other headache types (22). It remains, however, for future research to demonstrate this more definitively.
This raises the question as to the optimal design for future trials of spinal manipulation for headache. Such a study should, in our view, have a closely defined research question. This includes an adequate definition of the experimental and control conditions, the setting, and the outcome measure. Studies should be randomized to minimize selection bias and its sample sizes should be based on power calculations. Depending on the exact research questions, it could be ‘sham’ controlled and patient-blinded. In any case, it should be evaluator-blind. The test statistics should be predefined and relate to intergroup comparisons rather than to prepost differences. In view of the oftentimes emotional discussions in this area, such a study would benefit from an independent outside monitor. It is clear that a study of this nature is best designed with the input of chiropractors, research methodologists and statisticians. The above data shows that, at present, a study of this caliber (even though feasible) does not yet exist.
In conclusion, it is unclear from the findings of this systematic review whether or not spinal manipulation is an effective treatment for headache disorders. Methodological limitations coupled with the small number and considerable heterogeneity of the randomized trials we were able to identify make it difficult to rule out nonspecific (placebo) factors as an explanation for the clinical improvements that were consistently observed across trials, irrespective of headache category. We therefore believe that additional, better-designed trials are required before such treatments can be considered effective for headache disorders.
Footnotes
Acknowledgements
This work was completed while the first author was at the Complementary Medicine Program at the University of Maryland School of Medicine and was supported by a grant from the National Center for Complementary and Alternative Medicine, National Institutes of Health (5 PS0AT00084).