
Abstract
For an accurate description of the clinical features of the headache phase in migraine with aura (MA) attacks, we thought it useful to conduct a prospective study of consecutively referred MA patients seeking treatment at the Headache Centre of the University of Parma Institute of Neurology. The case series included 32 patients (22 women and 10 men). At the time of the first visit, each patient was given a questionnaire to be filled in at the next MA attack. Six patients (four women and two men) had attacks of migraine aura without headache. Among the remaining 26 patients (18 women and eight men), the duration of the headache phase was < 24 h in 23 (88.5%); pain location was bilateral in 14 (53.8%) and unilateral in 12, but occurring on the opposite side to aura only in one patient; pain intensity was mild or moderate in 13 (50.0%). The headache phase of MA appeared to have clinical features that differed widely from patient to patient and was consistent with the International Headache Society diagnostic criteria for migraine without aura in 26.9% of patients and for tension-type headache (TTH) in 23.1%.
Introduction
Very few reports have been published so far on the clinical features of the headache phase of migraine with aura (MA) attacks. The 1988 International Headache Society (IHS) classification (1) does not list any diagnostic criteria for the headache phase of MA, thus restricting MA diagnosis at the three-digit level to compliance with the diagnostic criteria set for aura. The only existing reference is to migraine with acute onset aura, to which the IHS classification applies the same criteria for the headache phase that are used for migraine without aura (MO). The need for a better definition of the clinical features of the headache phase of MA prompted us to carry out a prospective investigation of consecutively referred MA patients.
Patients and methods
We conducted a prospective study on 32 MA patients (22 women and 10 men) consecutively referred to the Headache Centre of the University of Parma Institute of Neurology. At the time of the first visit at our centre, patients had all their clinical data collected for a diagnosis of MA down to the three-digit level of the IHS classification. Each patient was given a self-administered questionnaire and was instructed on how to fill it in at the first MA attack following the first visit.
We used a single questionnaire comprising two sections, one for the aura phase and one for the headache phase. The section about aura comprised four subsections for visual disturbances, sensory disturbances, speech disturbances, and motor disturbances and/or other non-neurological symptoms, respectively. Patients were previously trained on the exact meaning of the items used in the questionnaire, where the location of the focal disturbances during the aura phase and the location of pain during the headache phase were defined as either right-handed, left-handed, or bilateral. The questionnaire had to be completed immediately at the end of both the aura and the headache phases in the respective sections. Later, the examiner determined whether aura was ipsilateral or contralateral to the headache side.
Among other things, the specially designed, previously validated questionnaire contained all the items necessary to establish a diagnosis of migraine down to the three-digit level of the IHS classification (1) and of tension-type headache (TTH) down to the two-digit level.
All patients were then seen again after the MA attack. At the follow-up visit, each patient handed in his/her questionnaire and discussed it with the examiner. Finally, we assessed whether the headache phase of the MA attacks in our patients fulfilled the IHS diagnostic criteria for migraine (both migraine without aura at 1.1 and migrainous disorder not fulfilling above criteria at 1.7) and for TTH (both episodic tension-type headache at 2.1 and headache of the tension type not fulfilling the above criteria at 2.3).
Results
Characteristics of our patient sample at the first visit
In our sample of 32 patients, including 22 women and 10 men, mean age at the first visit at our centre was 30.3±11.7 years (range 12–61 years), i.e. 29.7±10.08 years (range 12–52 years) for females and 31.7±15.6 years (range 17–61 years) for males.
Mean age at onset of MA was 22.0±11.6 years (range 6–48 years), i.e. 22.8±11.3 years (range 10–47 years) for females and 20.1±12.9 years (range 6–48 years) for males.
Fourteen patients (seven women and seven men), or 43.8% of the sample, did not suffer from any other forms of primary headache associated with MA. The remaining 18 patients (15 women and three men, or 56.2% of the sample) also had MO (eight female and one male), TTH (three female and two male), both of the above-mentioned headache forms (one female), and acute idiopathic stabbing headache (one female). Two women suffered from daily chronic headache.
By applying the IHS diagnostic criteria down to the three-digit level, we were able to classify each attack according to the various subtypes listed in the IHS classification. Overall, our 32 patients reportedly suffered from all the MA subtypes shown in Table 1.
Migraine with aura (MA) subtypes found retrospectively at the patients' first observation (n=32)

Data of the first prospective MA attack
The interval of time that elapsed from the first visit at referral and the first next MA attack was on average 2.9±2.3 months for each patient (2.8±2.1 months for females and 3.1±2.7 months for males), varying from 15 days up to 9 months.
From the analysis of the clinical features of the first MA attack following the first visit at referral, it appears that six patients (four women and two men) had attacks of migraine aura without headache. Three of these patients (two female and one male) had already reported a history of migraine aura without headache at their first visit, while two other patients (one female and one male) had reported a history of migraine with typical aura; finally, the remaining patient (a male) had reported a history of both migraine with typical aura and of migraine aura without headache (Table 2).
Migraine with aura (MA) subtypes at the first attack following the first visit (n=32)

Migraine with typical aura was the most frequent MA subtype, but migraine with prolonged aura was also common. Nearly one-fifth of the patients reported attacks of migraine aura without headache. Basilar migraine was extremely rare. No statistically significant differences were found between the two sexes for the different MA subtypes.
All 32 patients under study had an aura characterized by visual disturbances. These disturbances were the only focal neurological phenomenon accompanying aura in 15 patients (nine female and six male), were associated with paraesthesias in eight patients (six female and two male), and were associated with speech disturbances without paraesthesias in only one patient (a female).
Seven patients (six female and one male) had an aura with both visual disturbances and paraesthesias accompanied by a transient speech disturbance. Only in one case (a man) were visual disturbances and paraesthesias accompanied by a transient motor disturbance (precisely at the upper limb on the same side as the sensory disturbance). In no case was aura characterized only by sensory disturbances or speech disturbances or a combination of the two.
As regards the type of visual disturbances, 11 patients (nine female and two male), or 34.4% of the sample, had only scintillating scotomas; 12 (seven female and five male), or 37.5%, had a combination of scintillating scotomas and fortification spectra, seven (five female and two male) had only fortification spectra, and two more (one female and one male) had fortification spectra alternating with scintillating scotomas and negative scotomas.
These disturbances involved the whole visual field in 12 cases (eight women and four men), with hemianopsia at onset in one case (a woman, in the right-hand visual field). In the remaining 20 cases (14 women and six men), the visual disturbance appeared and continued as hemianopsia involving only the right-hand visual field in four patients (three female and one male) and the left-hand visual field in nine (five female and four male), and spreading progressively from the right to the left visual field or vice versa in seven patients (six female and one male).
Six patients (two female and one male), or 18.7% of the sample, complained of other neurological and non-neurological symptoms during aura, such as a diffuse sensation of cold, accompanied by shivering, pallor, panic attacks, drowsiness and diarrhoea.
In 40.6% of cases (13 patients, 10 women and three men), aura lasted between 11 and 30 min, i.e. between 5 and 10 min in four patients (two female and two male), between 31 and 60 min in three (two female and one male), and over 60 min in two (both female). In four cases (three women and a man), the duration of aura in the different MA attacks varied between 11 min and 60 min.
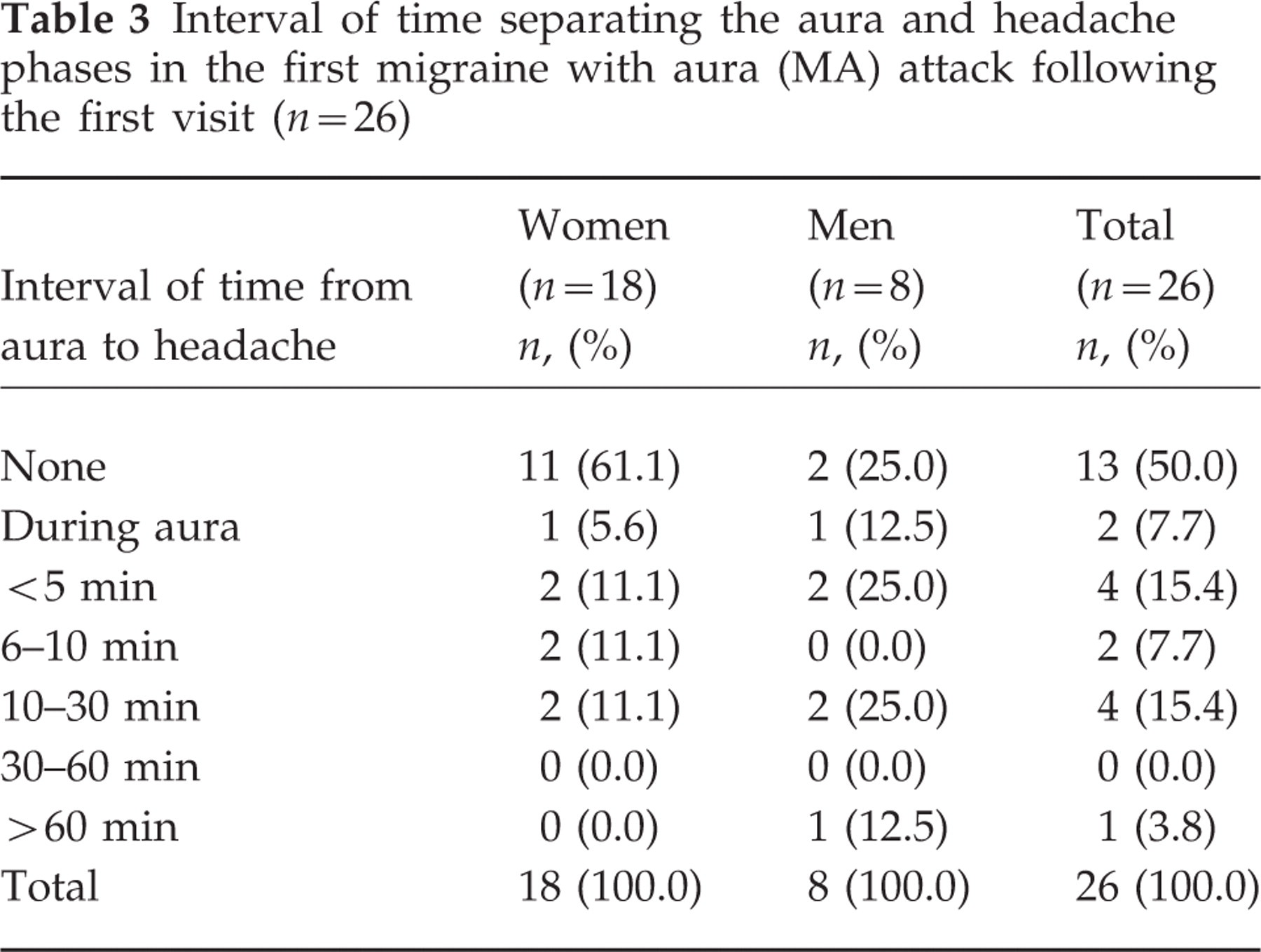
Before proceeding with a detailed analysis of the headache phase in the 26 patients (18 women and eight men) left after we excluded the six cases with migraine aura without headache, we tried to determine whether or not in these patients the aura and headache phases were separated by an interval of time. In half the cases, the aura immediately preceded the headache, while in the remaining 50% the interval of time separating the two phases varied between <5 min to >60 min (Table 3).
Interval of time separating the aura and headache phases in the first migraine with aura (MA) attack following the first visit (n=26)
Analysis of the clinical features of the headache phase showed that the duration of pain was <4 h in 46.2% of patients and varied between 4 h and 24 h in 42.3%. In the remaining three patients (all of them women), the pain might last from a minimum of 24 h to a maximum of >72 h. At onset, pain was unilateral in 13 (50.0%) of 26 cases and remained so throughout the attack in 12 patients; only in one patient (a woman) was the pain located on the opposite side to aura from the beginning until the end of the attack. The pain was severe and pulsating in type in 50.0% of cases, and was worsened by physical activity in 84.6%. The most common associated symptoms were nausea (50.0%) and phonophobia (46.1%), followed by photophobia (38.5%), osmophobia (23.1%), and vomiting (15.4%). In 23.1% of cases, the patients did not report any symptoms associated with pain (Table 4).
Clinical features of the headache phase of the first migraine with aura (MA) attack following the first visit in 26 patients

The headache phase of the MA attack fulfilled the IHS diagnostic criteria for MO in seven patients (26.9%), including six women (33.3%) and one man (12.5%); for migrainous disorder not fulfilling above criteria (coded as 1.7 in the IHS classification) in three patients (11.5%), all of them women; for TTH in six patients (23.1%), all of them women; for tension type disorder not fulfilling above criteria (coded as 2.3 in the IHS classification) in four patients (15.4%), including three women (16.7%) and one man (12.5%); for both the 1.7 group and the 2.3 group of the IHS classification in six patients (23.1%), including four women (22.2%) and two men (25.0%).
Discussion
As the collection of clinical data about MA attacks from a patient's previous medical history is quite complex and often recall biased, it is necessary to resort to a prospective method of investigation in order to provide a reliable definition of the various aspects characterizing an MA attack. However, very few prospective studies have been conducted so far on the clinical features of aura and/or the headache phase of MA—among them, Russell et al. (2), Jensen et al. (3), Balottin et al. (4) in children and Lanzi et al. (5) in young people aged 12–24 years, the last two investigating prospectively the characteristics of aura but not of the headache phase. In addition, no study has ever investigated prospectively the interval of time separating aura from the headache phase. In half of our patients, we found that some time elapsed between the end of aura and the beginning of the headache phase.
The symptoms that were most frequently associated with pain in the MA attacks were nausea and phonophobia. This finding is at variance with the observations by Rasmussen and Olesen (6), who found that photophobia and phonophobia were more common than nausea.
As to the average duration and the intensity of the headache phase, our results show that the headache almost always lasted <24 h—the percentage of patients reporting a duration even <4 h being as high as 50.0%—and that the pain was severe in half of our patients. Our findings are in agreement with the few ones published so far in the literature, including those of Rasmussen and Olesen (6), who found a headache phase lasting from <24 h in 77.2% of their patients, and with those of Russell (2), who reported a shorter duration and a less severe intensity of MA attacks compared with MO attacks.
There appears to be no clear consensus among the various authors in the literature about aura and pain location, the consistency between sides varying from 90.0% of Russell et al. (2) to 55.0% of Bana and Graham (7), down to 33.0% of Jensen et al. (3) and 14.0% of Ranson et al. (8). In our study, only one out of 13 patients had unilateral pain on the opposite side to aura. The total lack of diagnostic criteria for the headache phase of MA in the IHS classification prompted us to attempt a comparison of pain between our prospective study and the features listed in the IHS classification for migraine (both at 1.1 and at 1.7) and for TTH (both at 2.1 and at 2.3).
We found that the headache phase could be coded as migraine (1.1 or 1.7) or as TTH (2.1 or 2.3) in a comparable proportion of patients (about 40%), while in 23.0% of patients the headache phase could be clinically diagnosed as belonging to both groups.
The only two studies in the literature that have attempted to define the headache phase of MA attacks according to the diagnostic criteria set by the IHS for MO and/or TTH are those of Rasmussen and Olesen (6) and of Russell et al. (2). The former authors concluded that the headache that follows aura does fulfil the IHS diagnostic criteria for MO, the only significant clinical differences being a shorter duration and a lesser intensity of pain. The latter author prospectively demonstrated that, in about 50% of MA attacks, the headache phase was characterized by pain that was either too mild or too short-lived to fulfil the IHS diagnostic criteria for MO. Not considering whether aura was present or not, according to these authors such attacks could be classified as migrainous disorders (1.7) or TTH (2.1).
The presence of a headache phase in MA attacks that cannot be diagnosed solely as MO (1.1), as was found in our study on a clinical population, suggests the need for further studies, possibly among the general population, in order to provide clear indications on the headache phase of MA that could be used for a future review of the IHS criteria for MA diagnosis, which so far include no definition whatsoever of the characteristics of the headache phase following aura. The data obtained from our study are the result of a prospective analysis and, as such, should be considered clinically reliable. However, they are merely descriptive data, due to the relatively low number of cases under study. We believe that a study on a larger case series, such as the one that we have currently under way, will provide data that are also statistically reliable.