
Abstract
Background
The Headache Disability Inventory assesses the dimensions of headache disability, but it is not available in Brazilian Portuguese yet. We aimed to translate the Headache Disability Inventory into Brazilian Portuguese and analyze its measurement properties.
Methods
Consecutive patients with headaches diagnosed by expert neurologists as per the International Classification of Headache Disorders were included. For the cross-cultural adaptation, 30 individuals answered the translated Headache Disability Inventory version. The internal consistency was evaluated, and the structural validity was assessed through exploratory factor analysis. For the construct validity assessment, 132 individuals answered the Headache Disability Inventory-Brazil, 12-item Short Form Survey (SF-12), and Headache Impact Test (HIT-6). After 1–3 weeks, 67 individuals again answered the Headache Disability Inventory-Brazil for the reliability assessment. The Pearson's correlation test, the intraclass correlation coefficient and the standard error of measurement were analyzed.
Results
The pre-stage version of the questionnaire was considered as the final version. The Headache Disability Inventory-Brazil had an internal consistency of 0.84 and consisted of a functional, emotional and social participation domain (factor loads > 0.3). The internal consistency ranged from 0.81 to 0.93 for each of the three domains. For the construct validity, the Headache Disability Inventory-Brazil presented moderate correlation with the SF-12 (r = −0.70, p < 0.05) and with the HIT-6 (r = 0.67, p ≤ 0.05). Its test-retest reliability was considered to be excellent (intraclass correlation coefficient = 0.95) and the standard error of measurement was 2.26 points.
Conclusion
The Headache Disability Inventory-Brazil was successfully translated and culturally adapted to the Brazilian population. It can be used for the impact assessment of primary and secondary headaches with validity and reliability equivalent to its original version.
Introduction
Headaches are a common and prevalent neurological condition. In Brazil, the 1-year prevalence of headaches can reach 70.6% and among all these, 15.8% are migraine, 29.5% tension-type headache, and 6.1% chronic daily headache (1). Headaches are considered the second cause of the number of years lived with disability in the world, with a significant impact on patients’ daily life and productivity (2). Migraine stands alone as the world’s most important cause of disability (3) and the first cause of disability in individuals under 50 years old (4). Several scales have been developed as an attempt to quantify headache disability and overcome patients’ self-reported difficulties (5–8), allowing comparisons among individuals and a tailored therapeutic approach (2). The use of specific instruments for impact evaluation allows the assessment of the individual as a whole and takes different life domains into consideration (9).
The Headache Disability Inventory (HDI) questionnaire created by Jacobson et al. in 1994 (5) is one of the instruments used to assess headache disability. The HDI assesses different dimensions related to headache disability and interference with daily life during the last month (5,10). It is widely used and recommended for impact assessment in both research and clinical practice (9,11,12). The HDI questionnaire contains 25 questions subdivided into functional and emotional scales. Its total score, ranging from 0–100 points, ranks the individual from absence to the maximum level of disability (5).
However, this questionnaire has not yet been translated and culturally adapted into Brazilian Portuguese and its measurement properties have not been tested. Therefore, this study aimed to translate and perform the cross-cultural adaptation of the HDI into Brazilian Portuguese. Furthermore, we aimed to test its reliability, internal consistency, construct and structural validity in patients with primary and secondary headaches.
Material and methods
Sample
Consecutive patients were recruited and screened from a tertiary headache outpatient clinic in Ribeirão Preto, Brazil. Patients with primary and secondary headaches diagnosed by headache neurologists according to the International Classification of Headache Disorders, 3rd edition (ICHD-III) (13) were included if they were between 18 and 65 years old and had a headache at least 1 day in the previous month. Subjects with concomitant headaches or inconclusive headache diagnoses were excluded. Moreover, for the cross-cultural adaptation and reliability assessments, non-literate individuals were excluded. As recommended by the guideline for the process of cross-cultural adaptation of self-report measures, 30 patients were considered for the cross-cultural adaptation (14). A further 132 patients were included for structural and construct validity assessment, considered respectively very good and adequate according to the consensus-based standards for the selection of health measurement instruments (COSMIN). Sixty-seven patients were included for the reliability assessment, also considered adequate according to the COSMIN guidelines (Figure 1) (15).

Flowchart of patients included and excluded in the stages of cross-cultural adaptation, validity and reliability.
The study was approved by the Research Ethics Committee at Hospital das Clínicas de Ribeirão Preto, University of São Paulo (process number 3622/2017) and all participants clarified possible questions and signed a consent form before the data collection.
Translation and cross-cultural adaptation
After acquiring consent from the author of the original version, the HDI translation process questionnaire started. This process followed the recommendations made by guidelines for translations and cross-cultural adaptations of self-report measures (14,16). Our study followed these six stages, according to Beaton et al.: i) English to Portuguese translation, done by two professionals who were fluent in English and whose native language was Portuguese (T1 and T2); ii) synthesis of T1 and T2 to establish a common version of the questionnaire (T-12); iii) back-translation to English, performed by two fluent Portuguese translators whose native language was English (BT1 and BT2); iv) review of all reports by an expert committee, to reach a consensus and produce a pre-final version (14). The expert committee consisted of post-graduation students, clinicians, doctors, professors in the field, and all the translators involved in the previous stages. At this stage, cross-cultural adaptations were performed with the original version author’s help. After reaching the pre-final version, the pre-testing stage (v) was started. The pre-final version was administrated in 30 subjects with primary and secondary headaches. If more than 10% of patients had doubts regarding the same question, it would have to be reformulated, and the questionnaire would have to be applied again to 30 new subjects (17).
Measurement properties assessment
After the successful translation and cross-cultural adaptation of the HDI-Brazil, the evaluation of its measurement properties started (see Supplemental material) (15). All the patients answered a structured questionnaire with information about demographics and headaches, including the onset of pain, frequency, and intensity (NRS 0–10). The HDI-Brazil, the Headache Impact Test (HIT-6 GlaxoSmithKline) (7) and 12-item Short Form Survey (SF-12) (18) questionnaires were administered after the patient’s routine appointment at the headache outpatient clinic. The patients were instructed to answer the questionnaires in a self-applicable form regarding only the headache, under the supervision of the main researcher. Illiterate individuals answered all the questionnaires through interview 5,3% (n = 7).
In accordance with the COSMIN statement, the test-retest reliability assessment of the HDI was performed through in-person appointments with a time interval from 1–3 weeks between the first and second applications (15). For the construct validity evaluation, the headache frequency, intensity, the SF-12, and the HIT-6 questionnaires were used as a reference (7,18).
The SF-12 is considered a short version of the SF-36 questionnaire. It reproduces the same measurement properties as the SF-36 with some advantages, including reduced application time (18). This questionnaire contains 12 questions to evaluate different dimensions related to the quality of life, considering the individual’s perception of their health aspects in the last 4 weeks (18). The SF-12 score ranges from 37 to 123 points, and greater scores indicate a greater quality of life (19).
The HIT-6 was created to assess the impact of headache through a short set of six questions related to disability at work, school or social activities, pain intensity, fatigue, frustration and difficulty in concentrating during the last 4 weeks (7). Each question is answered using five possible categories ranging from “never” to “always”. The total score ranges from 36 to 78 points. The higher the score, the greater the impact of headache on patients’ daily life (7).
Statistical analysis
The internal consistency of the HDI-Brazil total score was assessed after the translation and cross-cultural adaptation to Brazilian Portuguese using Cronbach’s α coefficient. The results were considered adequate as they were between 0.70 and 0.95. Low values indicate a lack of correlation between the items and high values indicate redundancy in the questionnaire composition (20).
To access the structural validity, exploratory factor analysis was performed to verify whether the Brazilian version of the questionnaire has the same two factors as the original version. In order to define the factors, a Principal Component Analysis with Varimax Rotation was performed (21). The amount of model variance of the retained factors was demonstrated through eigenvalues greater than 1 and percentage of explained variance greater than 50% (22). The magnitude of the factor loadings for each question was also analyzed according to the item’s contribution to the model. Thus, items with a factor loading less than 0.3 after Varimax Rotation could be excluded (21).
The analysis of the Kaiser-Meyer-Olkin (KMO) test – known as the sample adequacy index – was also considered to identify whether the factor analysis model was adequate for the data (23). KMO values between 0.5 and 1.0 were considered (24). The internal consistency analysis was repeated after the structural analysis of the questionnaire.
Construct validity was analyzed through a two-tailed Pearson’s correlation among the HDI-Brazil, the SF-12 and HIT-6 questionnaires. The correlation between the HDI-Brazil questionnaire score and the frequency as well as intensity of the headache was also performed. Correlation values below 0.3 indicate weak correlation, between 0.31 and 0.7 are considered as moderate correlation, and values above 0.71 indicate a strong correlation (20).
The Intraclass Correlation Coefficient (ICC) analysis was performed for test-retest reliability of the HDI-Brazil, based on the total scores of the first and second questionnaire. ICC is classified as poor (<0.45), satisfactory (0.50 < ICC < 0.75) or excellent (>0.75) (25). Furthermore, the standard error of measurement (SEM) was calculated. All statistical analyses were performed in the SPSS 21 software and an alpha level at 5% was considered.
Results
Translation and cross-cultural adaptation
During the cross-cultural adaptation of the HDI questionnaire, English words and expressions were changed to improve the clarity of the Brazilian version. The expression “paying penalties” or “pagando penalidades” in the Brazilian raw translation was adapted to “suffering consequences” or “sofrendo consequências” in Portuguese. The item “I don’t like social events” needed the help of the questionnaire’s author to clarify if the original meaning was “I don’t like social events” or “I don't enjoy social events.” After clarification, the latter option was more suitable for the question, and the expression in Portuguese was adapted to “eu não aproveito eventos sociais”. Both male and female word forms were included in the HDI Brazilian version. The word “severe” was translated to Portuguese as “forte”. The term “any spouse (significant other)” has been defined as “spouse (partner)” or “cônjuge (parceiro (a))” in Portuguese. The last change was regarding the expression “focus my attention away” which was translated to “taking my focus away” or “tirar o foco” in Portuguese. Thus, it was possible to adapt the questionnaire to the Brazilian population.
The last stage of the HDI translation and the cross-cultural adaptation was carried out between April and May 2018. The HDI-Brazil was administered to 30 patients (age 34.9, SD 11.5 years old) and of the total sample, 90% (n = 27) were women. Patients with the following diagnosis were included: Migraine with aura (26.6%, n = 8) and without aura (50%, n = 15), chronic migraine (6.6%, n = 2), familial hemiplegic migraine (3.3%, n = 1), post-craniotomy headache (3.3%, n = 1), chronic tension-type headache (3.3%, n = 1), trigeminal autonomic headaches, including cluster headache (3.3%, n = 1), and unilateral neuralgiform headache with conjunctival hyperemia and tearing (SUNCT) (3.3%, n = 1). The education level of the individuals ranged from incomplete elementary education to complete university education: 10% (n = 3) attended elementary school, 23% (n = 7) attended high school, 67% (n = 20) attended the university.
Up to 20% of patients had doubts regarding the meaning of the words “disability”, “impact”, “restrict”, “spouse”, and outlook on the world in questions 1, 3, 4, 8 and 10, respectively. The doubts were cleared in just five of the 25 questions, and no more than three individuals (10%) had doubts in the same question. Therefore, the version applied at the pre-test stage was considered as the final version of the questionnaire (Supplemental material).
The analysis of the internal consistency of the HDI-Brazil total score resulted in a Cronbach’s α coefficient of 0.84; the Cronbach's α coefficient was 0.86 and 0.88 for the functional and emotional subscales, respectively.
Structural validity
The assessment of the questionnaire’s measurement properties was performed between June 2018 and August 2019. Of the 530 potential patients, 132 patients with primary and secondary headaches were included for the validity assessment. Considering the total sample, 71.2% (n = 94) patients were women with a mean age of 39.6 (12.7) years. Patients with the following diagnosis were included: Migraine (39.4%, n = 52), tension-type headache (12.9%, n = 17), trigeminal autonomic cephalalgia (12.9%, n = 17), and secondary headaches (34.9%, n = 46). The education level of the total sample ranged from illiterate to technician level of education: 0.7% (n = 1) was illiterate, 22% (n = 29) attended incomplete basic education, 27% (n = 36) completed basic education, and 46% (n = 60) attended university education. The HDI-Brazil mean score of all patients was 54.0 (SD: 27.7), for the HIT-6 the mean score was 63.7 (SD: 7.6), and for the SF-12, 79.1 (SD: 17.6). The sample characteristics according to the headache diagnosis are represented in Table 1.
Sample characteristics of the validity of the HDI-Brazil questionnaire (mean and standard deviation).

M: migraine; TAC: trigeminal autonomic cephalalgia; TTH: tension-type headache; SH: secondary headaches; NVS: visual numeric scale.
The exploratory factor analysis revealed that the construct of the HDI-Brazil is described by three domains. A third factor (domain) related to social participation showed the best factor solution to support the concepts underlying the HDI questions. Hence, besides the emotional and functional factors described by the original version, the social participation domain was also observed (Table 2).
Factor loadings of HDI-Brazil questions represented by emotional, functional and social participation factors.

Note: Magnitude of factor loadings analyzed by Varimax Rotation method with KMO normalization. Bold values refers to greatest factor loading of each question.
Q: question.
The emotional domain encompasses questions related to feeling angry, losing control, not socializing, having problems with the spouse, family and friends, feeling of going crazy, discrediting the worldview, feeling desperate, stress in the relationships, disrupting life goals, not thinking clearly, feeling tense, angry, confused and frustrated due the headache. The functional domain encompasses questions related to disability, limitation of daily activities, reading difficulties and not being able to focus on anything else but the headache. The new domain related to social participation, encompasses the questions related to the impact of the headache, restriction of leisure activities, fear of leaving home, feeling harmed, avoiding other people, not enjoying social events and not traveling due to the headaches.
The questions were grouped into three factors through the Varimax Rotation with Kaiser normalization. The percentage of cumulative explained variance was 58.98%, with a KMO index of 0.92. All factor loadings values were above 0.3, which was considered as an acceptable contribution of all items to the questionnaire construct (17). The factor loadings of each question and the model statistics can be verified in Table 1.
As the HDI-Brazil questionnaire presented three domains, Cronbach’s α coefficient was calculated to assess the internal consistency of each domain. The emotional domain showed internal consistency of 0.93, the social participation domain showed 0.87, and the functional domain showed 0.81.
Construct validity
The HDI-Brazil total score presented a strong negative correlation with the SF-12 questionnaire (r = −0.70, 95% CI: −0.79 to −0.59, p < 0.05, Figure 2) and a moderate positive correlation with the HIT-6 questionnaire (r = 0.67, 95% CI: 0.56 to 0.75, p < 0.05), Figure 3). The three domains of HDI-Brazil were correlated with the two subscales of the SF-12 questionnaire. The social participation and emotional factors had a negative moderate correlation with the SF-12 mental domain (r = −0.50, 95% CI: −0.64 to −0.35, p < 0.05). The functional factor also had a negative moderate correlation with SF-12 physical domain (r = −0.58, 95% CI: −0.69 to −0.44, p < 0.05). The correlation between the HDI-Brazil total score and the frequency of headache was positive but weak (r = 0.07, 95% CI: 0.05 to 0.42, p < 0.05). The correlation between the HDI-Brazil total score and the headache intensity was positive and moderate (r = 0.45, 95% CI: 0.28 to 0.60, p < 0.05). This result demonstrated that the HDI-Brazil score increases with both frequency and intensity of headache.

Correlation between HDI-Brazil and SF-12 total score.

Correlation between HDI-Brazil and HIT-6 total score,
Reliability
Of the 132 potential patients who underwent the questionnaire’s validity assessment, 67 patients came back for the second appointment. Up to 74.6% (n = 50) were women and the following headache diagnosis were included: Migraine (35.8%, n = 24), tension-type headache (12%, n = 8), trigeminal autonomic cephalalgia (10.5%, n = 7), and secondary headaches (41.8%, n = 28). The education of the total sample ranged from elementary school to university education, and 10% (n = 7) attended incomplete basic education, 16% (n = 11) attended complete basic education, and 74% (n = 49) university education. The sample characteristics are presented in Table 3.
Sample characteristics of the reliability assessment and the score on the first and second application of the HDI-Brazil questionnaire (mean and standard deviation).
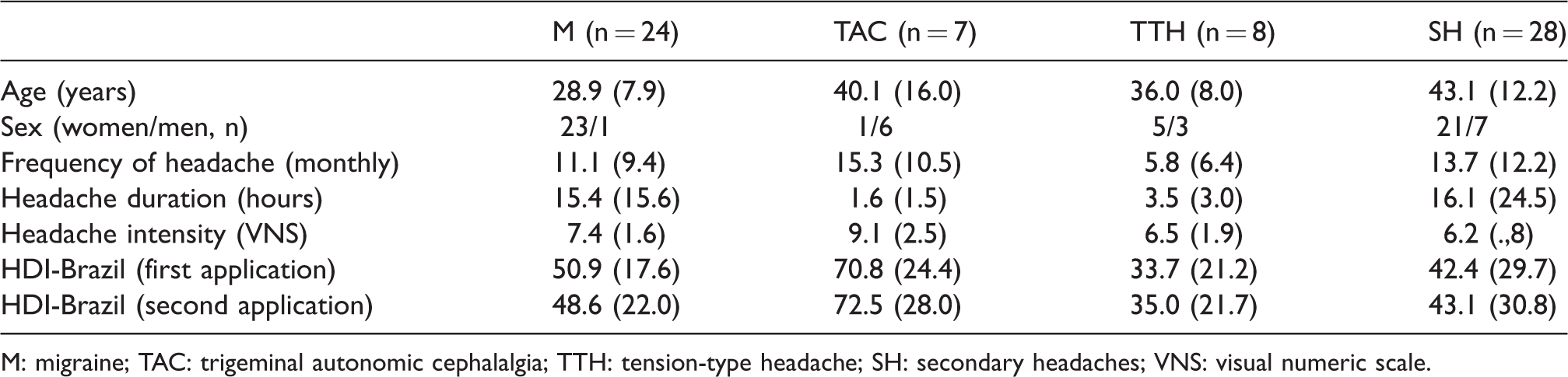
M: migraine; TAC: trigeminal autonomic cephalalgia; TTH: tension-type headache; SH: secondary headaches; VNS: visual numeric scale.
The average score of the HDI-Brazil questionnaire was 54.0 (SD: 27.7) in the first application and 47.5 (SD: 28.6) in the second application. In the re-evaluation, 39% of the sample had a score higher than 60 points. The reliability for HDI-Brazil was considered excellent (ICC = 0.95, p < 0.05) and it presented an SEM of 2.26 points.
Discussion
The Brazilian version of the HDI questionnaire was successfully translated and adapted to Brazilian Portuguese. Furthermore, its measurement proprieties were considered equivalent to the questionnaire’s original version, with acceptable validity and reliability. Therefore, the questionnaire is considered adequate to measure the disability related to the headaches and it can be used to assess Brazilian headache patients.
Chronic conditions such as headaches can be very disabling and affect several areas of an individual’s daily life. Thus, the use of tools to quantify the impact of a disease is relevant to assess patients individually and as a whole, since the same condition can impact different individuals in various forms or domains (26).
Besides the Brazilian Portuguese and the original version in English (5), the HDI questionnaire was also translated into Spanish (27) and German (28). The subscales of the original (5) and the three Brazilian versions exhibit excellent internal consistency, demonstrating the HDI-Brazil maintained similar meaning to the original version. Exploratory factor analysis of the HDI-Brazil was accomplished to verify the number of factors of the questionnaire. Different from the original version (5), the Brazilian version verified an extra domain of social participation. Unlike the Brazilian version of the questionnaire, the Spanish (27) version also presented just the functional and emotional factors (5). The majority of HDI-Brazil questions are related to the emotional domain of the questionnaire. Still, all questions factor loads had an acceptable contribution to the questionnaire construct. Future studies aiming to confirm the three domains and taking them into account in the sub-scores calculation are needed.
In the assessment of construct validity, our results demonstrated moderate to strong correlations among the HDI-Brazil with the SF-12 (29) and HIT-6 questionnaires (7). The correlations between the SF-12 and HDI-Brazil subscales were negative, corroborating to the fact that the quality of life is lower in individuals with greater disability, related to both functional and emotional aspects (29). The moderate correlation between HDI-Brazil and HIT-6 may have been influenced by the slight differences between the questionnaires. Even though both measure headache impact, the HIT-6 addresses only the disability construct, while the HDI-Brazil includes different emotional and functional domains. Meanwhile, the positive correlation with the HIT-6 shows that both questionnaires are useful to evaluate headache impact with comparable results. Our results also demonstrated that the HDI scores are correlated moderately with headache intensity, but not with headache frequency during the last month. It could be hypothesized that the inclusion of several types of headache may explain this weak correlation, since evidently more disabling headaches are related to greater disability, independently of their frequency. Furthermore, Magnusson & Becker also demonstrated that headache frequency is not clearly related to disability or psychological factors (30).
The test-retest reliability for both the English (10) and the Portuguese version of the HDI questionnaire were similar and considered excellent. The HDI-Brazil had ICC = 0.95, p < 0.05 and the original version of the HDI had ICC = 0.83, p < 0.05, without significant differences between the first and the second application. Moreover, the SEM was considered low (2.26 out of 100 points).
The HDI English version (5) was conducted through an interview, while the Brazilian version was through a self-applied form. Despite this difference, both versions exhibited similar validity and test-retest reliability. It shows that the questionnaire can be either administered by the clinician or a researcher or can be answered by the patient. It allows flexibility according to the clinical or research routine, maintaining similar measurement properties of the assessment tool.
Another difference between the English and the Brazilian versions was regarding the sample assessed. Even though both included men and women in the samples, the original only considered patients with migraine and tension-type headache diagnoses (5). For the Brazilian version, we opted to include patients with both primary and secondary headache diagnosis. The inclusion of individuals with diverse headache types is important for the impact assessment of less prevalent headaches, which also require attention and medical care as much as any other headache types. The Brazilian version of HDI is considered valid and reliable also in the assessment of both primary and secondary headaches.
As reported in the review by Haywood et al. (11), the HDI questionnaire is relevant as it addresses the headache-related disability construct comprehensively, considering several domains. With this questionnaire being widely used (11), the Brazilian Portuguese version would allow comparisons to the disability to be verified in different populations. Furthermore, it can be included in the clinical routine as well as in research projects, allowing proper patient evaluation and an individualized approach.
There are several limitations with this study. First, the sample was collected in a tertiary care center, which consists of a large proportion of patients with more severe headaches, such as migraine and secondary headaches. This factor is reflected in our sample, which consisted of a small number of prevalent but least impacting headaches, such as TTH. The second limitation was the small number of males in the sample. Therefore, measurement properties assessment according to sex was not possible. Furthermore, the small number of subjects in each headache subgroup also did not allow the analysis of each headache type. We also consider the non-application of the MIDAS questionnaire (6) in individuals with migraine as a limitation. The use of MIDAS would allow construct validity assessment in comparison with the HDI in the migraine sample. However, the aim of the study was to use tools that could be applied to all types of headaches and not only migraines. As a last point, we emphasize that it was not possible to assess other relevant measurement properties, such as the responsiveness of the questionnaires to a treatment. Future studies should aim to assess this, as it is very relevant for clinical practice.
Despite the limitations, according to the COSMIN recommendations (15), the sample size included in this study was considered adequate to very good for both validity and reliability analysis, ensuring the generalizability of the results for both measurement properties. Furthermore, the validity and reliability properties have been tested on several types of headache diagnoses, including trigeminal autonomic cephalalgia and secondary headaches. Some had not had their level of disability measured so far, due to the lack of an adequate tool. Moreover, the data collection was performed in a center for headaches and craniofacial pain and therefore all diagnoses were obtained by neurologists specialized in headaches. This study, at least, provided a questionnaire for the national impact assessment of any type of headache in a clinical or research setting.
Conclusion
The HDI-Brazil questionnaire was successfully translated and culturally adapted to the Brazilian population and the Brazilian version presented validity and reliability equivalent to the original versions to assess the impact of primary and secondary headaches.
Clinical implications
The HDI-Brazil has been translated and culturally adapted to Portuguese speakers. Its validity and reliability are considered similar to the original HDI version. The HDI-Brazil can be widely used to assess the disability of both primary and secondary headaches.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102420949860 - Supplemental material for Brazilian Portuguese version of the Headache Disability Inventory: Cross-cultural adaptation, validity, and reliability
Supplemental material, sj-pdf-1-cep-10.1177_0333102420949860 for Brazilian Portuguese version of the Headache Disability Inventory: Cross-cultural adaptation, validity, and reliability by Juliana Pradela, Débora Bevilaqua-Grossi, Thais Cristina Chaves, Fabiola Dach and Gabriela Ferreira Carvalho in Cephalalgia
Footnotes
Acknowledgements
The authors would like to thank the clinical team of the Craniofacial Pain Outpatient Clinic from Ribeirão Preto Clinics Hospital.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data sharing statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior Brasil (CAPES) – Finance Code 001.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.