
Abstract
The objective of the present study was to use systematic nation-wide case-finding methods to establish the prevalence and sex ratio of hemiplegic migraine (HM) in the entire Danish population of 5.2 million inhabitants. Affected patients were identified from three different recruitment sources: the National Patient Register, case records from private practising neurologists and advertisements. Based on the observed number of affected patients from each case-finding method, it was attempted to estimate the total number of affected patients by means of the statistical method known as capture- recapture. Two hundred and ninety-one affected patients were identified; 147 were familial HM from 44 different families, 105 were sporadic HM and 39 were unclassifiable HM. The HM sex ratio (M: F) was 1: 3. Based on the identified number of affected patients the prevalence of HM at the end of 1999 was estimated to be 0.01% in Denmark, where the familial and sporadic form were equally frequent.
Introduction
Hemiplegic migraine (HM) exists in a familial and a sporadic form. The familial form, called familial hemiplegic migraine (FHM), is due to its dominant mode of inheritance, according to the operational diagnostic criteria of the International Headache Society (HIS classification), recognized as a distinct subtype of migraine with aura (MA) (1). FHM is characterized by migraine attacks associated with some degree of motor weakness/hemiparesis during the aura phase and where at least one first-degree relative (parent, sibling or child) has identical attacks (Table 1). The sporadic form, called sporadic hemiplegic migraine (SHM), is characterized by identical attacks but other family members are unaffected. SHM is classified as MA, as MA, according to the HIS classification, can include hemiparesis. The literature describes about 100 FHM families (2–46) and about 100 SHM cases (6, 10, 43, 45–55) world-wide. All are clinic-based materials. Due to the rarity of HM, traditional sampling methods are impractical when assessing the prevalence. The aim of the present study was to use several systematic, nation-wide case-finding methods to establish the prevalence and sex ratio of sporadic and familial HM.
The operational diagnostic criteria of migraine with aura (MA) and familial hemiplegic migraine (FHM) according to the International Headache Society's classification (1)

Materials and methods
Overview of the search strategy
Patients were initially recruited systematically from three different recruitment sources and screened by using a telephone interview. The screen of recruited patients identified 195 patients affected with HM. In order to stratify these into FHM or SHM cases, we subsequently screened their relatives. All first-degree relatives were screened and second-degree, third-degree or more distant relatives were screened by two different strategies depending on whether an affected first-degree relative had been identified or not. Affected patients with at least one affected first-degree relative were diagnosed as having FHM, whereas affected patients without any affected relatives were diagnosed as having SHM.
The three sources of ascertainment
Our search strategy included patients from the entire Danish population of 5.2 million inhabitants. Three sources of ascertainment were used to identify HM cases: a computer search of the unique and very complete National Patient Register of all hospitalized patients, screening of case records from headache clinics and practising neurologists, and advertisements for patients with HM. These three sources were chosen to systematically recruit HM patients treated at hospitals, HM patients treated by private practitioners or general practitioners (GPs) and HM patients (treated or non-treated anywhere), who were members of the major patient organization for headache patients in Denmark.
From the National Patient Register, we extracted records of all patients admitted to hospital or seen as outpatients at a department of neurology or paediatrics in a Danish hospital from 1994 to 1997 and discharged with a diagnosis of migraine with aura or migraine with complication (ICD 10 diagnosis DG431 or DG433).
More than 27 000 case records were screened, in the period 1997–99, for patients with migraine with motor or more widespread sensory symptoms. The time frame covered by these records was from the date of screening to at least 10 years prior to the screening time. About 6000 of these case records were from two different headache clinics and a SPECT-scanning clinic, whereas about 21 000 case records were from practising neurologists from all over the country. The neurologists had been selected due to a special interest in headache disorders and represented 17% of the total number of practising neurologists in Denmark.
All chairmen of Danish departments of neurology (n=21) and paediatrics (n=21), and all Danish private practising neurologists (n=54) and private practising paediatricians (n=41) received a posted letter with information about the project, and were asked to report patients with migraine with motor symptoms.
A review article about FHM and an advertisement for patients with HM were placed in Ugeskrift for Lœger, the major Danish medical journal, in June 1998 (56). An advertisement was also placed in the journal of the major Danish organization of headache patients, which has approximately 1000 members.
Invitation
All recruited patients received a posted letter with information about the project, before they were contacted by telephone. The letter emphasized the importance of participation and stated that the objectives were to study the prevalence and the inheritance of migraine associated with some degree of motor weakness/hemiparesis. The letter included a return slip and a prepaid envelope. The chairmen of the departments of neurology and paediatrics provided us with written consent to contact patients treated in their department. Patients recruited from case records of the private specialists had to reply confirmatively to the specialist before we were allowed to contact them by telephone. The other patients were contacted by telephone, unless they stated within 5 days that they did not want to participate. Patients who could not be reached by telephone received a second letter asking for their telephone number. Those not responding had a third reminding letter. The project was approved by The Danish Ethical Committees.
Definition of familial, sporadic and unclassifiable hemiplegic migraine
FHM was defined according to the criteria of the IHS, i.e. as patients with migraine with an aura that includes some degree of motor weakness/hemiparesis where at least one first-degree relative also has attacks of migraine with an aura that includes some degree of motor weakness/hemiparesis (1).
SHM was defined as patients with migraine with an aura that includes some degree of motor weakness/hemiparesis without other affected relatives (first-degree relatives were non-affected, verified by telephone interview, and other relatives were unaffected, by history).
‘Possibly affected FHM relatives’ were defined as patients who had had one FHM attack, and thereby did not fulfil the criteria for FHM or patients who by history had or had had FHM, but where the diagnosis could not be verified with certainty.
‘Unclassifiable HM’ was defined as patients affected with HM where the family history with regard to migraine status was not obtainable.
Definition of prevalence
The prevalence was defined by the total number of affected patients by the end of 1999 divided by the total number of Danish inhabitants at that time. HM is thought of as a chronic disease, thus once a patient has had a minimum of two HM attacks, the patient is affected.
Definition of primary and secondary cases and probands
Primary cases were defined as affected HM patients identified from any of the three recruitment sources. Secondary cases were defined as affected HM patients identified by screening relatives of FHM probands. In each family the proband was defined as the first identified primary case in the family.
Participation pattern
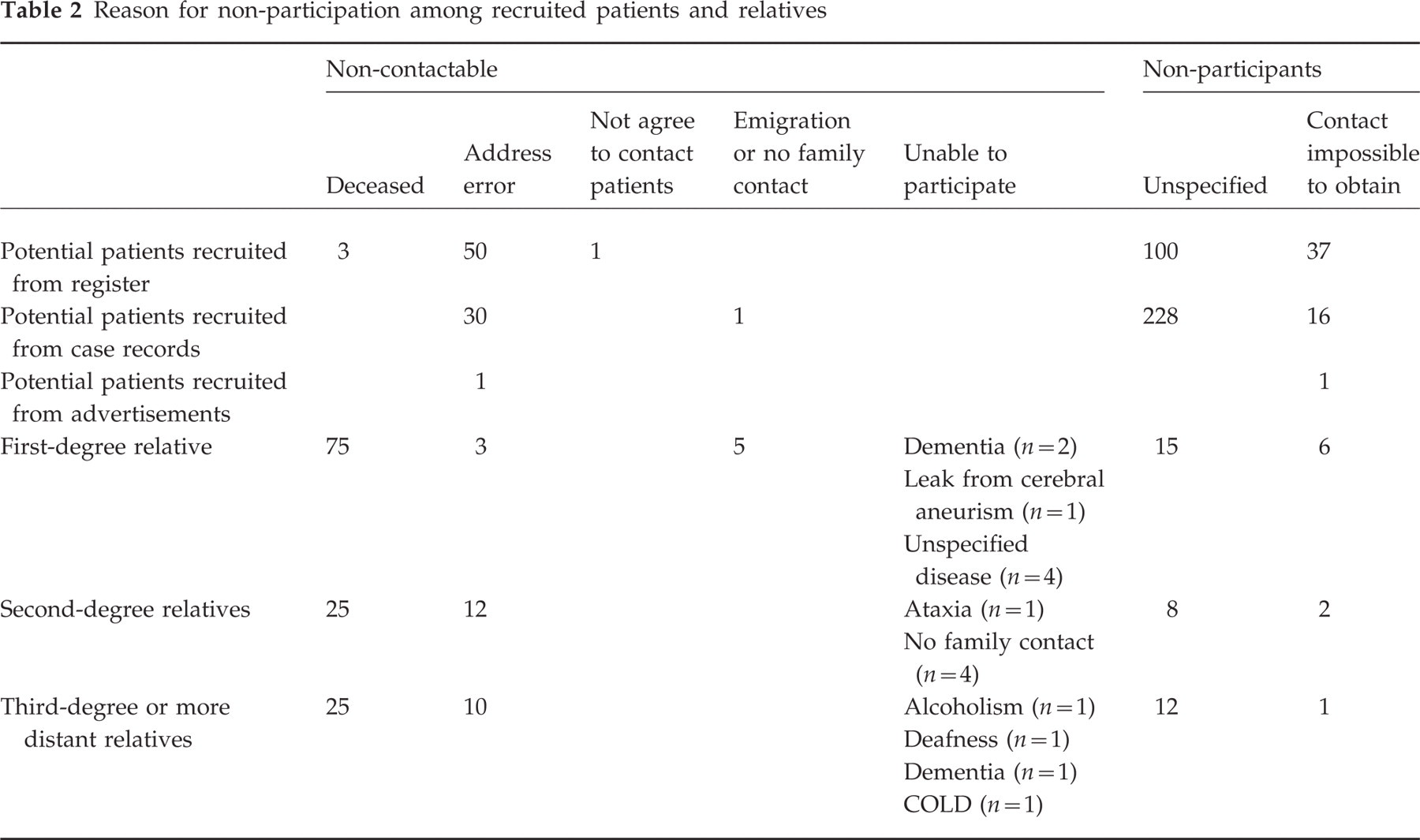
The ascertainment of recruited patients and their pattern of response and participation are shown in Fig. 1. A total of 1828 (500 M : 1328 F) patients from the three recruitment sources were contacted. Those interviewed by telephone were labelled participants (n=1446) and those not interviewed were labelled non-participants (n=382). The ascertainment of relatives and their pattern of response and participation are shown in Fig. 2. A total of 1486 (722 M : 764 F) relatives were available. All first-degree relatives above 15 years of age were contacted for a telephone interview. Relatives of 15 years or below 15 years of age were only contacted for a telephone interview if suspected of having or previously having had headache or aura symptoms. If an affected first-degree relative was identified, the proband was classified as FHM. Among second- and third-degree or more distant FHM relatives, as many relatives as could be traced in the families were contacted for a telephone interview, except children/young people living with their parents not suspected of having or having had headache or aura symptoms and a few grown-up relatives not suspected of having or having had headache or aura symptoms. If no affected first-degree relative was identified, the proband was classified as SHM. Among second- and third-degree or more distant SHM relatives only individuals that were suspected of having or having had headache or aura symptoms were contacted for an interview. The reasons for not participating are shown in Table 2.
Reason for non-participation among recruited patients and relatives

Ascertainment of patients with hemiplegic migraine and their response and participation pattern. The arrows show how many familial hemiplegic migraine (FHM) and sporadic hemiplegic migraine (SHM) patients were recruited from each source and the extent of the overlap between the sources.

Ascertainment of relatives and their response and participation pattern. Of the 723 first-degree relatives, 240 were relatives of FHM probands and 483 were relatives of SHM probands. Among 313 second-degree relatives, 264 were relatives of FHM probands and 49 were relatives of SHM probands. Of the latter all 49 relatives were contacted and all participated. Among 450 third-degree or more distant relatives, 448 were relatives of FHM probands and two were relatives of SHM probands. Of the latter both were contacted and participated.
The overall participation rate among recruited patients was 79% (1446/1828). The participation rate of patients recruited from the hospitalization register, case records and advertisements were 87%, 65% and 99%, respectively.
The overall participation rate among relatives was 95% (859/903). The participation rates of first-degree relatives, second-degree relatives and third-degree or more distant relatives were 96%, 94% and 93%, respectively. A total of 49 second-degree SHM relatives were contacted and all participated, and two third-degree or more distant SHM relatives were contacted and both participated, the rest of the second- and third-degree or more distant relatives were FHM relatives.
Telephone interview, physical and neurological examination and neuroimaging results
Recruited patients from the National Patient Register, and recruited patients from the case records with widespread sensory symptoms, were screened for migraine with motor symptoms in a screening telephone interview by three medical students, all well trained in headache diagnostics (MKE, SFR and IA). All patients who, in the screening interview, were suspected of having motor symptoms, together with recruited patients from advertisements and recruited patients from the case records with motor symptoms, were contacted in a more extensive and validated telephone interview by a neurological resident with experience in headache diagnostics (LiLT). In order to differentiate whether the patient actually had a hemiparesis or not, 11 questions were asked concerning the patient's ability to defeat gravity with the affected limb during HM attacks, as shown in Table 3. Those classified as affected had to answer yes to at least two of the questions from questions 2–11. Overall 90% answered positively to at least five questions from questions 1–10.
Motor aura screening questions∗
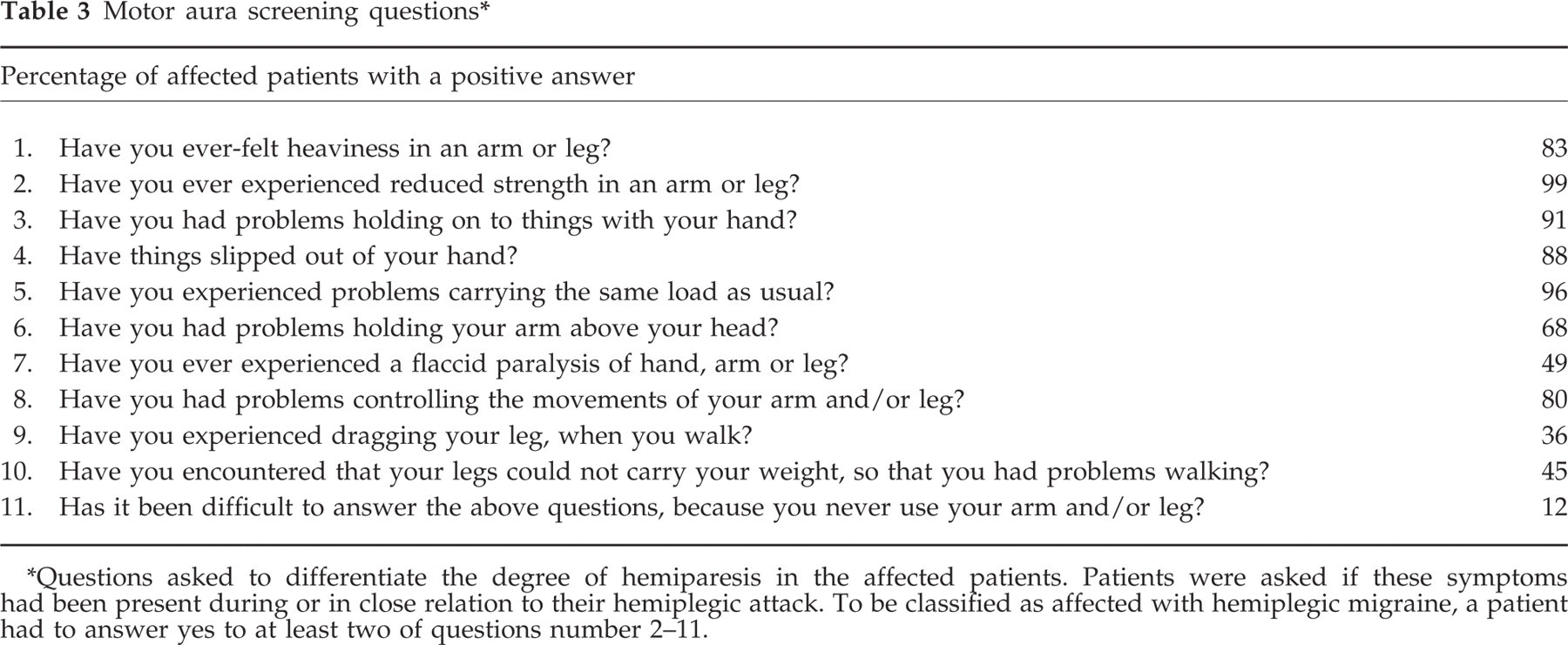
∗Questions asked to differentiate the degree of hemiparesis in the affected patients. Patients were asked if these symptoms had been present during or in close relation to their hemiplegic attack. To be classified as affected with hemiplegic migraine, a patient had to answer yes to at least two of questions number 2–11.
The probands were asked about affected first- or second-degree relatives by the neurological resident. If there, according to the proband, was no family history of hemiplegic attacks, first-degree relatives had an extensive telephone interview by the medical students. Families with a positive history of hemiplegic attacks, according to the proband, were telephone-interviewed by the neurological resident. If the proband had been wrong about the family history and the medical students identified an affected relative, all family members were re-interviewed by the neurological resident.
The telephone interviews took place from February 1999 to August 2000. All familial and sporadic HM patients also had a face-to-face interview and a physical and neurological examination performed by a neurological resident (LiLT examined all FHM patients and EO examined all SHM patients). The examinations took place at the hospital or in the patient's home, depending on the patient's preference.
Descriptions of CT- and/or MRI-/MR-angio scans of the cerebrum were collected on affected patients who reported previously having had a CT- and/or MRI-/MR-angio scan. All affected patients were included also if a previous scan was unobtainable, and if a patient had had both types of scans only the MRI/MR-angio scan was counted.
The capture-recapture method and statistical analysis
In an attempt to estimate the total number of affected patients, the identified number of HM patients was corrected for ascertainment by the epidemiological method known as capture-recapture. This method derives its name from censuses of wildlife populations. The technique allows the number of cases in a defined population to be estimated by using two or more sources of cases, i.e. records from hospitals or general practice, etc. Each source alone may undercount the actual number of cases, as would a simple aggregate of the sources that excluded duplicate cases. Capture-recapture techniques use information provided by duplicate cases to allow the number of people not identified at any of the sources to be calculated (57). An estimate of the total number of cases is thus the sum of the calculated unobserved cases and the observed cases. In its simplest form the capture-recapture technique makes some underlying assumptions. First, the sources are assumed to be independent. Secondly, all individuals have the same probability of being captured. The use of multiple sources and log-linear modelling applied to this technique has been recommended when the first of these assumptions are violated (57–60). By incorporating source dependence, an empirical estimate of the deviation from independence can be given by using log-linear modelling.
The data used in log-linear analysis of incomplete lists are the tabulations of the number of cases found in each possible combination of ascertainment sources. If there are three sources, A, B and C, then there are seven non-overlapping possible modes of ascertainment: A only, B only, C only, AB not C, AC not B, BC not A and ABC. In this approach the data are regarded as an incomplete 2 t contingency table (t is the number of lists) for which the cell corresponding to those individuals uncounted by all lists is missing. To derive an estimate using the log-linear approach, it is assumed that there is no ‘three–way’ interaction of sources, and more generally, if there are three sources available that there are at most 3 − 1=2 source interactions. This assumption implies an extrapolation formula for the number uncounted. With three sources, there are eight possible models (using all the data) excluding the three-way interaction. Various log-linear models are fitted to the observed cells and a proper model is selected using deviance statistics. The chosen model is then projected onto the unobserved cell. The log-linear modelling was done in the program SAS PROC CATMOD.
Although the formal definition of sporadic patients is pragmatic (no affected first-degree relative has been observed), some patients classified as sporadic could be false SHM patients, in the sense that only by coincidence did they not get any affected relatives identified (e.g. the family was too small). We therefore furthermore estimated the number of ‘false’ sporadic cases by looking at the distribution of affected relatives per FHM proband. If the distribution of affected relatives per FHM proband is Poisson distributed with a mean value λ, λ can be estimated even though the theoretical number of families with 0 secondary cases is unknown. The Poisson distribution assumes that it is equally likely to identify secondary cases of FHM patients in all FHM families, and that all FHM families are approximately of the same size. If the family sizes vary (so they cannot be fitted within the Poisson distribution), a similar but more uncertain calculation may be performed using the negative binomial distribution.
Results
A total of 195 affected HM patients were identified from the three recruitment sources. When screening the relatives another 96 HM patients were identified. Of the 195 ‘primary cases’, seven patients were relatives of FHM probands. After screening the relatives, we were able to state that of a total of 291 affected patients, 147 patients from 44 different families had FHM, 105 had SHM and 39 had unclassifiable HM.
In FHM, the 44 (9 M, 35 F) probands had 103 affected and 22 possibly affected relatives among 952 relatives (450 M, 502 F) (240 first-degree relatives, 264 second-degree relatives and 448 third-degree or more distant relatives). The status ‘possibly affected’ FHM relative was due to: only one FHM attack (n=6), a history of FHM but the patients were dead (n=10), impossible to understand due to ataxic speech (n=1), had dementia (n=1), or declined to participate for unspecified reasons (n=2). Furthermore, two children were unable to properly describe their attacks.
In SHM, the 105 (20 M, 85 F) probands had 534 relatives (272 M, 262 F) available (483 first-degree relatives, 49 second-degree relatives and two third-degree or more distant relatives).
In unclassifiable HM, the 39 (6 M, 33 F) affected had an unknown family history of HM. The hemiplegic migraine was unclassifiable due to: a relative with possible hemiplegic attacks was deceased (n=18), the family declined to participate according to the proband (n=10), the proband had no contact with the family (n=7), a person with possible hemiplegic attacks declined to participate for unspecified reasons (n=3), or the proband was adopted (n=1). The unclassifiable probands were included in the group of affected patients.
Sex ratios
Overall the sex ratio (M : F) for HM was 1 : 3.3 (68 M, 223 F). The sex ratio for FHM was 1 : 2.5 (42 M, 105 F) and there was no statistically significant difference in sex ratio between affected FHM probands and affected FHM relatives (P=0.17, chi-square test). The sex ratio for non-familial HM was 1 : 4.3 (20 M, 85 F). The sex ratio for non-classifiable HM was 1 : 5.5 (6 M, 33 F).
Consultation rates
Forty-nine per cent (72/147) of the FHM patients (75% (38/51) of primary FHM cases and 35% (34/96) of secondary FHM cases), 66% (69/105) of the SHM and 72% (28/39) of the unclassifiable HM patients reported that they had had a CT- and/or MR scan or had been admitted to the hospital at least once due to hemiplegic attacks.
Observed prevalence
Based on the identified number of HM patients, the observed prevalence of FHM was 147 cases +20 unclassifiable cases (with a positive family history of attacks with unilateral motor weakness/hemiparesis)=167/5.2 million inhabitants, which equals 0.003%, and the observed prevalence of SHM was 105 cases +19 unclassifiable cases (with a negative family history of attacks with unilateral motor weakness/hemiparesis)=124/5.2 million inhabitants, which equals 0.002%.
Estimated prevalence
The capture-recapture calculations are based on the 195 patients who were identified from any of the three primary sources. The identified number of HM patients and their distribution on the three ascertainment sources is shown in Table 4. In this table the data are regarded as an incomplete 23 contingency table for which the cells corresponding to those individuals uncounted by all lists are missing. Thus five patients were identified from both the National Patient Register and case records, but not from advertisements, and eight patients were identified from both the National Patient Register and advertisements, but not from case records.
The distribution of the 195 identified hemiplegic migraine patients, on the three recruitment sources (data regarded as a 23 contingency table, for which the cell corresponding to those individuals uncounted by all lists is missing)

Our estimated prevalence from several different log-linear models is shown in Table 5. In these estimates an interplay between two sources A and B is illustrated as A∗B. If we assume that the three ascertainment sources identified patients independently and with same probability (chose the model ‘all independent’), the number of missing patients was estimated to be 398 and the total number of affected patients was estimated to be n= 593 with
Prevalence estimates from the different log-linear models. Lists A, B and C are from the National Patient Register, case records and advertisement, respectively. In these estimates an association between two sources A and B is illustrated as A∗B. To test the fit of the models, the difference between −2 log(likelihood) from one line to the next is compared with a chi-square distribution with one degree of freedom, – values larger than 3.84 correspond to significance at the 5% level. On a level of 5% significance, the models all independent and A∗C fitted poorer than the other models, which fitted similarly

To test the fit of the models, the difference between −2log(likelihood) from one line to the next is compared with a chi-square-distribution with one degree of freedom and values larger than 3.84 correspond to significance at the 5% level. On a level of 5% significance, the models ‘all independent’ and ‘A∗C’ fitted poorer than the other models (had a higher −2log L). The other models fitted similarly because (− 2log L ‘model all independent’)−(− 2log L ‘for each of the other models)>3.84, and (− 2log L)−(− 2log L)<3.84, when comparing the −2log L for the other models.
It is seen that the estimate of the total number of cases that the three case-finding methods ‘should have identified’ varies considerably according to which model is fitted. Although the large standard errors made the models compatible, the models ‘all independent’ and ‘A∗C’ fitted poorer on a 5% significance level than the other models, which fitted similarly well. The most conservative model (model: A∗B, A∗C) estimates that a total number of 390 (
Estimating the number of ‘false’ sporadic cases
The distribution of secondary cases of affected patients in the FHM families is shown in Table 6. Maximum likelihood (program ad hoc in S-plus) estimated λ=2.035, Var. (λ)≈0.058, from which the expected total number of FHM families was estimated to be n=50.6 with an estimated
Distribution of secondary cases per FHM family and fitted Poisson distribution and negative binomial distribution

The estimate of 30 false sporadic cases (29% of total number of identified SHM cases) is better fitting, but more imprecise than the estimate of seven false sporadic cases (7% of total number of identified SHM cases).
Results of physical and neurological examination in FHM
Four FHM-affected subjects were not examined due to refusal of participation for unspecified reasons (n=3) and emigration (n=1). A total of 145 patients were examined (143 FHM patients and two FHM relatives with cerebellar ataxia without co-occurrence of FHM). Of the 143 FHM patients, 121 had a normal physical and neurological examination. Twelve patients (10 FHM patients and two without FHM) had cerebellar ataxia, without other neurological symptoms. Eleven of these were from the same family. In this family eight had ataxic speech, 11 had a wide-based ataxic gait, three had nystagmus, 10 had disturbed finger–nose and knee–heel test and one patient had head tremor. The ataxia in this family was slowly progressive from 8 to 10 years of age and associated with progressive cerebellar atrophy, present on MR-scans in three patients and CT-scans in one patient (a total of five of these patients had been scanned). One FHM patient from another FHM family had cerebellar ataxia characterized by wide-based gait and disturbed finger–nose and knee–heel test, no ataxic speech, no nystagmus and no tremor, with an age at onset of 52 years.
Three patients with HM since childhood had permanent neurological symptoms caused by a previous stroke; one of these was attributed to an aortic stenosis. Seven patients (two from one family) had minor neurological deficits, i.e. sensory disturbances or reduced co-ordination of a limb caused by a hemiplegic attack. One patient had a sensory ataxia verified by nerve conduction examination and normal MRI. One patient had a left supranuclear facial palsy and reduced strength in her right upper limb caused by a previous surgery for a cerebral aneurysm. These patients (except the two patients with cerebellar ataxia without co-occurrence of FHM) were all included as affected with FHM.
Results of neuroimaging in FHM
Thirty-six scans, 23 MRI/MR-angio and 13 CT scans were collected from patients with FHM. Of the 23 MRI-/MR-angio scans, 17 were normal, two showed findings not compatible with the symptomatology (case 6018 and 6020) and four showed cerebellar atrophy without any other changes. The latter all had cerebellar ataxia.
Case 6018: a small lacunar infarction of the cerebellum, no supratentorially pathology. The physical and neurological examination was normal.
Case 6020: a small lacunar infarction near the anterior horn of the right lateral ventricle. The neurological examination showed disturbed finger–nose and knee–heel test and an extensive plantar reflex. Symptoms had occurred in association with a FHM attack, but had not resolved.
Of the 13 CT scans, 11 were normal.
Case 6010: postoperative changes after previous surgery of an aneurysm on the intracerebral anterior communicating artery, no signs of previous stroke.
Case 6044.11: a small lacunary infarction in the centre of the right hemisphere. The physical and neurological examination showed symptoms caused by a previous stroke. Symptoms had occurred in association with FHM attack, but had not resolved. All patients including case 6010, 6018, 6020 and 6044.11 were included as affected FHM patients.
Results of physical and neurological examination in SHM
Five SHM patients were not examined due to refusal of participation for unspecified reasons (n=5). One hundred SHM patients had a physical and neurological examination; of these 92 were normal. One individual had reduced sensation to touch in a small area on her upper left arm, but normal pain, vibration and temperature sensation and motor function, and normal straight arm test and tendon reflexes. Two individuals had typical cerebellar symptoms without other neurological symptoms. In these patients the neurological examination revealed wide-based ataxic gait (n=1), nystagmus (n=1), disturbed finger–nose and knee–heel test (n=1) but no dysarthria (n=0) or tremor (n=0). One had a normal CT scan and neuroimaging was not available in the other person affected. Three individuals with HM since childhood had had a minor stroke in their fifties. These patients had had SHM since childhood, which previous to the stroke never caused any permanent neurological symptoms. One individual had a left-sided peripheral facial nerve paresis and no other physical or neurological findings and one individual had symptoms caused by a previous carpaltunnel syndrome but no other physical or neurological findings. These patients were all included as affected with SHM.
Results of neuroimaging in SHM
Thirty-nine scans, 23 MRI-/MR-angio and 16 CT scans were collected from patients with SHM. Of the 23 MRI-/MR-angio scans, 22 were normal (four patients had irrelevant changes, cases 5003, 5072, 5083 and 5099) and one had changes not compatible with the symptomatology (case 5095). Of the 16 CT scans, 15 were normal (one patient had irrelevant changes, case 5012) and one patient had changes not compatible with the symptomatology (case 5502).
Case 5003: a small enlargement of the left temporal horn of the cerebral ventricle, without any changes of the parenchyma. The physical and neurological examination was normal.
Case 5012: a small internal frontal hyperostosis. The physical and neurological examination was normal.
Case 5072: a slight asymmetry of the cerebral ventricles. The physical and neurological examination was normal.
Case 5083: a couple of subcortical small WM lesions in the right frontal hemisphere. The clinical and neurological examination showed symptoms caused by a previous stroke with positive Romberg (falling right), clumsy alternating movements of her right arm, normal strength of right and left extremities, normal sensibility and reflexes overall. These symptoms were associated with a FHM attack and had not resolved.
Case 5095: a small hyperintense area in the posterior part of the left lateral ventricle. The physical and neurological examination was normal.
Case 5099: a small solitary hyperintense lesion in the left centrum semivowel. The physical and neurological examination was normal.
Case 5502: very light changes parieto-occipital on the right side of the hemisphere, described as consistent with possible infarcts. The physical and neurological examination was normal. All patients, including cases 5003, 5012, 5072, 5083, 5095, 5099 and 5502, were included as affected SHM patients.
Discussion
Methodological considerations
As with other types of migraine, the diagnosis of the hemiplegic migraine (HM) relies exclusively on the information given by the patients. The most precise information from a study population is ascertained by prospective recordings. However, such recordings are difficult to do since only a minority of sufferers fills out the diaries. Furthermore, HM sufferers often have rare attacks that make prospective recordings impossible. Therefore, prospective data of HM cannot be representative. Representative data can, however, be ascertained retrospectively from the general population although the threshold of recall probably varies with the severity and recency of the condition (61, 62). HM is a severe subtype of migraine with aura, which makes it more likely to be remembered than migraine with less severe aura. Recall bias is therefore probably less than in the more common types of migraine. We therefore believe that retrospective recordings are the only possible way to obtain a representative group of HM patients.
The year 1994 was chosen as the first year of inclusion from the National Patient Register because migraine without aura and migraine with aura this year for the first time were given different disease codes. Screening all migraine would have been impossible and we therefore concentrated on migraine with aura. The year 1997 was chosen as the last year of inclusion from the National Patient Register because it was the last year with complete data at the time of study onset. However, due to the fact that we started to advertise intensively for patients in 1998, we assume that the majority of patients who have been hospitalized in 1998 and 1999 were identified. All three recruitment sources supplemented each other as each source identified a number of cases not observed by the other methods.
The operational diagnostic criteria of the IHS were used, as this classification is universally accepted and has shown a high validity for diagnosing clinic patients with migraine, tension-type headache or both (63) and high reproducibility for the different subtypes of migraine (64, 65). The data were collected in a semistructured telephone interview previously validated in epidemiological surveys (66–68). In order to make sure that only patients with true weakness and not patients with sensory changes, which often confuse the issue, were included, questions regarding motor aura symptoms were added and strict criteria for the motor aura (Table 3), as well as for the basilar migraine symptoms, were used.
All semistructured telephone interviews on affected individuals were done by one neurological resident (LiLT) specially trained in headache diagnosis. One interviewer is desirable, as the involvement of more interviewers invariably increases diagnostic variability (64). Together with one other neurological resident (EØ) she also did all clinical and neurological examinations. Of the collected CT/MR scans from affected patients the majority were normal, had irrelevant changes or changes not compatible with the symptomatology, therefore these patients were all included in the study. Four (CT or MR) scans of affected HM patients showed cerebellar atrophy consistent with findings in several previous studies of patients with co-occurrence of HM and cerebellar ataxia (29, 42, 44, 69), and very few patients had changes on a CT or MR scan compatible with a previous stroke. These patients all had had HM since childhood, previous to the stroke never with permanent neurological symptoms, and in adulthood had had a HM attack where varying degrees of neurological symptoms had not resolved after an attack. These patients were all included in the study because their attacks were thought of as secondary to HM.
Three medical students who worked continuously on the project during the study period and were supervized by one of the authors (LiLT) did a first screening of some of the recruited patients. They all had a special interest in neurology and were extensively trained in interview techniques and headache diagnostics. Firstly, they participated in recruiting patients from case records of private specialists and headache clinics. Secondly, they did some of the screening interviews for motor aura and, thirdly, they did the more extensive interview of relatives of SHM probands. About 500 patients excluded in the screening interview for this study (because of no motor aura symptoms) have later in another study been interviewed more extensively by a physician and none had HM (70, 71). This demonstrates the validity of our selection procedure among recruited patients.
Denmark has a rather stable population and only citizens born in Denmark were included. This, together with the existence of the central personal register, where every citizen is registered with a specific number, combined with highly developed medical registers of our public hospitals, makes Denmark a well-suited country for epidemiological surveys. The majority of the medical specialists are employed at the hospitals, which are all owned and run by the government. Hospital admission and access to private specialist's services require referral by a GP. It is free to consult a GP and free to be referred to a specialist, which makes it easy for the patients who wish to consult a physician.
The majority of patients recruited from case records came from headache clinics and only seven probands were identified from case records of practising neurologists. The seven patients found in private practices were recruited from selected neurologists with a special interest in headache. Possibly a few more HM cases could have been identified by searching case records of all practising neurologists (n=54); however, the much larger contribution from hospital records suggested that this huge task would not be feasible.
Patients who exclusively consulted their general practitioner and who were not referred to a neurologist or a paediatrician were reached by an advertisement in the major Danish medical journal Ugeskrift for Lœger and the journal of the major Danish organization of headache patients.
Even though our search was not complete and may be skewed towards larger FHM families, we believe that our material is the largest and most representative material of HM ever collected.
Sex ratio
Overall the male : female sex ratio for FHM was 1 : 2.5 and the sex ratio of SHM was 1 : 4.5. The sex ratio among affected relatives was more equal in FHM families with more than four affected individuals. These families had a male : female sex ratio among affected relatives of about 1 : 2, which is still a female preponderance compared with the sex ratio reported in selected FHM families (23, 30, 37, 43, 72). The over-representation of women in our FHM families and in SHM cases could be due to ascertainment bias but it more likely reflects a difference in genetic background.
Statistical considerations
None of our case-finding methods identified all HM cases; therefore we explored the applicability of the so-called capture-recapture method as a means of combining the evidence from several methods to obtain a more realistic estimate of the total number of HM patients among Danish inhabitants. This method has previously been applied to results obtained by cross-checking of registers combined with active case search strategies, to determine the prevalence of other rare diseases (73–79).
When assuming independence between the three sources, we estimated the number of missing patients to be 398±97. However, there are many reasons to believe that our three sources are not independent and that the selection probability varies between patients: all three sources recruited patients from hospitals or private specialists, the geographical intensity is (mostly for source B=case records) varying and the three sources were not quite contemporary. Because of this we fitted several different log-linear models and found rather widely varying estimates of the total number of HM patients. Although the large standard errors made them all compatible, the models ‘all independent’ and ‘A∗C’ fitted poorer on a 5% significance level than the other models, which fitted similarly (Table 5). Even though our estimates of the prevalence of HM differ, these calculations emphasize that the true number of clinical HM patients in Denmark at the end of 1999 must be considerably higher than the identified number of patients. Very likely the true number of HM patients would be at least twice as high (i.e. model A∗B, A∗C, Table 5).
As specified in the methods section, important assumptions behind the capture-recapture method are the independence between sources and the ‘equal catchability’ assumption that for each given source, patients have the same probability of being included. Both assumptions are most likely violated at least to some extent in our application. To compensate for the first assumption, we fitted all possible log-linear models for our incomplete 23 table, following Bishop et al. (58). The result was hardly satisfactory, giving widely varying results for models that seemed to fit equally well. The most obvious explanation seems to be deviation from the second assumption of equal catchability. We have not attempted to implement the various suggestions in the literature (80–82) describing heterogeneity in patient ‘catchability’, primarily because of lack of suitable covariates. Our general conclusion from this case study about the applicability of the capture-recapture method is necessarily rather sceptical. However, as it is important to know the prevalence of this disease and the capture-recapture method is the only method available to estimate the prevalence of this rare disease, we believe it makes sense to use the method.
Prevalence
The total number of affected HM patients is estimated to be at least twice the observed number of patients (n=195), which equals 390 affected HM patients among 5.2 million inhabitants. However, when estimating the prevalence of HM we have to consider the 96 secondary cases identified from screening relatives. Some of these patients had previously sought medical assistance. Those that sought medical assistance during our study period should have been among the recruited patients, but were missed (one assumption) and those that did not seek medical assistance or did seek medical assistance outside the study period should not have been among the recruited patients (second assumption). As we do not know how many of the secondary cases belonged to either of the two groups, the most precise estimate of HM would be an interval between a conservative estimate (a total of 390 HM cases) and a less conservative estimate (a total of 390 + 96=486 HM cases) among 5.2 million inhabitants. Based on these data, the prevalence of HM is estimated to be between 0.0075 and 0.0093%, which rounded up is 0.01% at the end of 1999.
Thus, the prevalence of HM was not as low as previously thought, but much lower than the prevalence of migraine with typical aura symptoms (66, 83, 84).
Footnotes
Acknowledgements
We thank the many sufferers of hemiplegic migraine and their many non-affected relatives who agreed to participate. We also thank our many colleagues for their excellent collaboration and Hanne Kηckelhahn for computing assistance. The work was supported by grants from the Cool Sorption Foundation of 1988, the Foundation for Research in Neurology, the Danish Headache Society, The A.P. M⊘ller Foundation for the advancement of medical science, the Novo Nordisk Foundation, the IMK-Almene Foundation, the GlaxoWellcome Research prize and Ms Else Torp Foundation.