
Abstract
The objective was to examine the association between high blood pressure (BP) and chronic daily headache using 24-h ambulatory blood pressure monitorization (24-h ABPM). This was a cross sectional study in an out-patient clinic. Women were selected among patients referred for first evaluation, 62 with chronic daily headache and 57 without chronic daily headache. The main outcome measures were mean office systolic and diastolic blood pressure (BP), mean systolic and diastolic daytime and night-time BP and BP load, and mean systolic and diastolic nocturnal fall. Office systolic BP was 138.2 mmHg for women with chronic daily headache and 141.7 mmHg for women without headache (P = 0.36). Office diastolic BP was 88.9 mmHg for women with headache and 92.7 mmHg for women without headache (P = 0.17). Mean daytime and mean night-time systolic BP was, respectively, 122.2 mmHg and 108.8 mmHg for women with headache and 122.9 mmHg and 109.5 for women without headache (P = 0.82 and P = 0.80, respectively). Mean daytime and mean night-time diastolic BP was, respectively, 78.6 mmHg and 65.4 mmHg for women with headache and 79.9 mmHg and 67.1 mmHg for the women without headache (P = 0.80 and P = 0.45, respectively). There was no difference between the two groups regarding systolic and diastolic BP load and nocturnal systolic and diastolic fall. No significant difference in BP values was observed in women with chronic daily headache compared with women without headache using 24-h ABPM.
Keywords
Introduction
Conflicting results have emerged from investigations into the relationship between headache and arterial blood pressure. Bulpitt et al. observed the presence of headache in 31% of patients with untreated, severe hypertension compared with 15% in treated hypertensive patients and normotensive controls (1). Cooper et al. investigated 11 710 hypertensive patients and reported that headache was a common symptom related to arterial blood pressure (2). A population-based study observed that in women with migraine, diastolic blood pressure was significantly higher than in women without migraine (3). More recently, in a population-based study, headache was associated with hypertension for both treated and non-treated patients (4). In contrast, in a population-based study, Walters found no differences for either systolic or diastolic blood pressure when individuals with headache were compared with individuals who had not had a headache in the previous year (5). Using data from the 1960–62 United States Health Examination Survey of Adults, Weiss observed no differences in the occurrence of headache between normotensive and hypertensive groups (6). In all these studies, blood pressure was measured in an office setting using standardized technique.
The 24-h ABPM has become a clinically useful procedure for evaluating hypertensive patients, and has resulted in significant improvement in understanding the behaviour of blood pressure in the world outside of clinicians' offices. By giving a more accurate picture of daily fluctuations in blood pressure, 24-h ABPM allowed for easier diagnosis of white-coat hypertension and for this reason it is an excellent tool for examining the association between blood pressure and chronic daily headache.
To investigate whether or not a true association exists between high blood pressure and headache, we performed a 24-h blood pressure monitorization in women with chronic daily headache and women without headache.
Methods
Study population
We studied 119 women between ages 15 and 69 years selected from patients referred for first evaluations in a general outpatient clinic of a tertiary hospital. Among patients of this clinic, 10% suffer from headaches and 50% have hypertension observed in a first evaluation. We included only women in our study because prevalence of most types of headache is higher in women than men (7, 8).
In this study, the women with headache were consecutive patients who visited the clinic between May 1995 and February 1996 with chronic daily headache as the main complaint. The women without headache were the first consecutive patients of approximately the same age referred to the clinic for other complaints (except headache- or migraine-associated symptoms) and who were seen immediately after patients with chronic daily headache. Patients with cardiac, pulmonary, hepatic and renal conditions were excluded from the study, as were those with severe disability, those who lived in another city, and those who had taken drugs for hypertension, anxiety, depression, or migraine prophylaxis in the prior 3 months. Basically, the only medicines used by women participating in the study were hormonal contraceptives and/or analgesics. Five women in the group without headache did not agree to participate in the study, leaving 62 women who met criteria for chronic daily headache and 57 women who never or rarely report a headache episode. All participants signed an informed consent approved by the Institutional Ethics Committee.
Definition of chronic daily headache
Subjects were initially interviewed by a physician using a multiple choice formatted questionnaire for headache modified from Raieli et al. (9) that was translated to Portuguese and validated for Portuguese-speaking people in a previous study (10). This questionnaire included information about age, presence of recurrent headaches during the previous 12 months, and characteristics of headache such as frequency, duration, location, type of pain, severity, and accompanying symptoms according to International Headache Society criteria (11). For all patients, body mass index (BMI) was calculated by dividing the weight (light clothes) in kilograms by the square of height in meters.
Chronic daily headache was defined according to Silberstein et al. as women with more than 15 days of headache per month for more than 6 months in the previous year and who have more than 4 h of headache during a day (12). According to the subtypes of chronic daily headache proposed by Silberstein et al., 111 (93.3%) cases were transformed migraine, 6 (5.0%) were chronic tension-type headache and 2 (1.7%) were new daily persistent headache.
Blood pressure measurement and 24-h ambulatory blood pressure monitoring
We measured blood pressure in the office according to guidelines established by the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI). High blood pressure was defined as systolic blood pressure of 140 mmHg or higher and/or diastolic blood pressure of 90 mmHg or higher confirmed on at least two subsequent visits during one to several weeks (13).
All subjects agreed to 24-h ambulatory blood pressure measurement using an oscillometric device (SpaceLabs model 90207) that has been validated according to the British Hypertension Society Protocol (14). We followed the guidelines of the Second International Consensus Meeting on 24-h ambulatory blood pressure measurement (15). Cuffs were fitted to arm diameter to avoid overestimation of measured blood pressure. The participants were asked to fill out a diary recording daily tasks, meal time, sleeping and waking hours, and the presence and duration of headache.
Twenty-four-hour ABPM parameters elected for analysis were mean values of systolic and diastolic daytime and night-time blood pressure, mean systolic and diastolic daytime blood pressure load (percentage of measures higher than 140 mmHg for systolic blood pressure and higher than 90 mmHg for diastolic blood pressure) and mean systolic and diastolic night-time blood pressure load (percentage of measures higher than 120 mmHg for systolic blood pressure and higher than 80 mmHg for diastolic blood pressure). Mean systolic and diastolic nocturnal falls were calculated using the real hours of sleeping as follows: mean diurnal (systolic or diastolic) blood pressure minus mean nocturnal (systolic or diastolic) blood pressure divided by mean diurnal (systolic or diastolic) blood pressure. White-coat hypertension was defined as presence of higher office blood pressure values at the interview with normal parameters at 24-h ambulatory blood pressure measurement (16, 17).
Statistical analysis
We presented means and frequencies for baseline characteristics. Comparisons
among groups were performed using
Results
Table 1 shows baseline characteristics of the two groups. Women with chronic daily headache were slightly younger and reported more frequent analgesic use compared with women without headache. In the clinic, hypertension was detected in 46.8% of women with headache and 57.9% of women without headache (P = 0.23).
Characteristics of women with and without chronic daily headache (CDH)
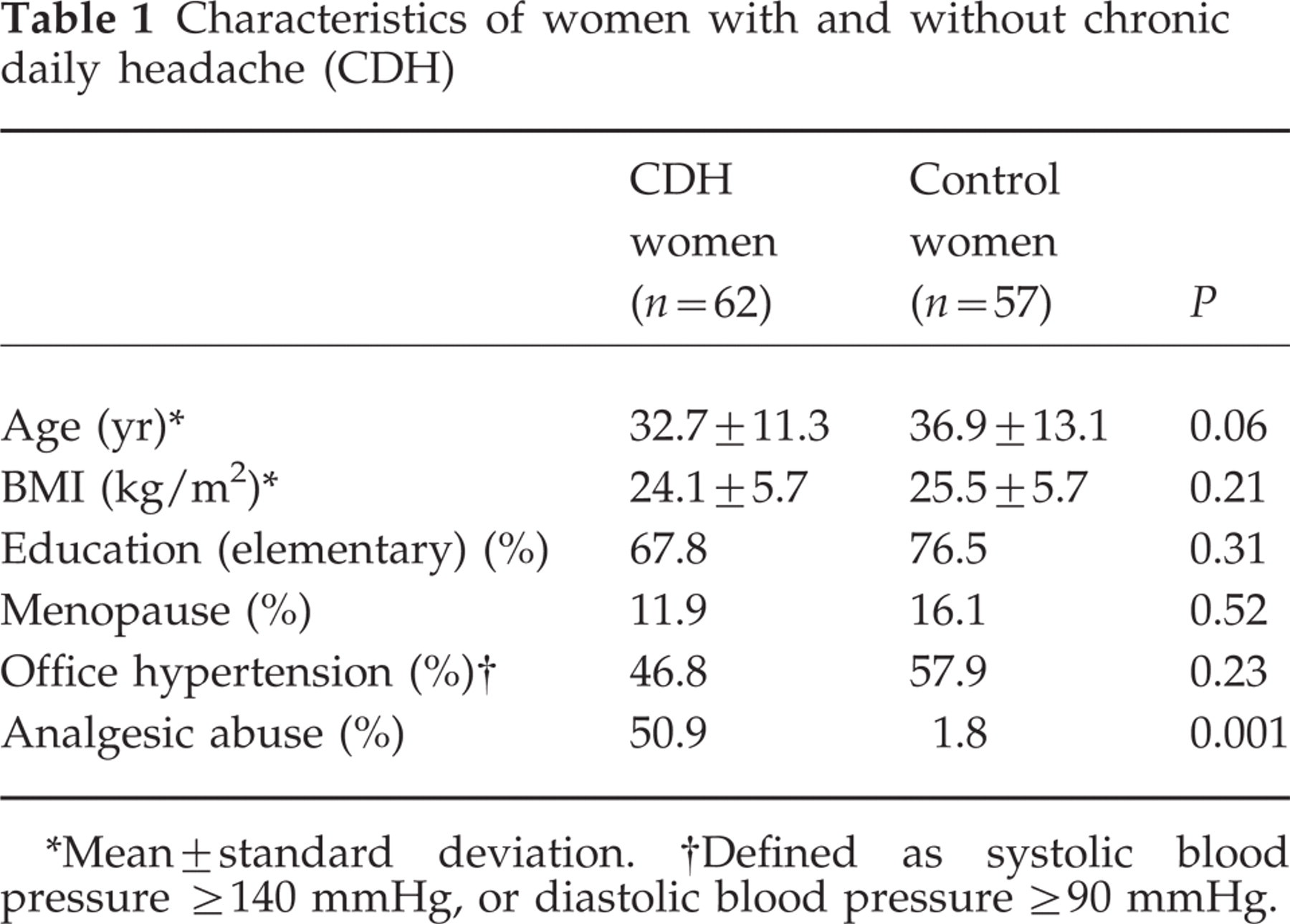
∗Mean±standard deviation.
†Defined as systolic blood pressure ≥140 mmHg, or diastolic blood pressure ≥90 mmHg.
During 24-h ambulatory blood pressure monitoring, headache was reported by 73% of subjects with chronic daily headache and 22.6% of subjects without chronic daily headache (P < 0.001).
Table 2 shows the comparison of the mean values of systolic and diastolic blood pressure at the clinic (office systolic and diastolic blood pressure), mean values of systolic and diastolic daytime and night-time blood pressure, mean values of systolic and diastolic daytime and night-time blood pressure load and mean values of systolic and diastolic nocturnal fall between women with chronic daily headache and controls using analysis of variance. Although mean values of systolic blood pressure and especially of diastolic blood pressure measured at the clinic were lower for women with chronic daily headache, the data are not statistically significant (P-values of 0.36 and 0.17, respectively). We did not observe any difference in the mean values of daytime and night-time systolic and diastolic blood pressure, systolic and diastolic blood pressure loads, and systolic and diastolic nocturnal & fall.
Blood pressure values obtained in a 24-h ambulatory blood pressure monitorization and office blood pressure in women with and without chronic daily headache

SBP = systolic blood pressure; DBP = diastolic blood pressure.
∗Adjusted for age and analgesic use.
†Office systolic blood pressure defined as ≥140 mmHg and office diastolic blood pressure defined as ≥90 mmHg.
No differences in blood pressure values were observed between women with chronic daily headache reporting pain during the 24-h ABPM and those with chronic daily headache not reporting headache pain during the 24-h ABPM.
A significant number of subjects classified in the clinic as hypertensive had normal blood pressure values during 24-h ABPM, white-coat hypertension was observed in 21.3% of subjects with chronic daily headache and 22.8% of controls (P = 0.85).
Comments
Our study does not show any difference in a variety of blood pressure values between women suffering from chronic daily headache and women without headache, and thus does not verify the higher values of diastolic blood pressure found among women with migraine as reported by Rasmussen et al. (3). In fact in our study, office diastolic blood pressure was lower in women with chronic daily headache, although this result did not reach statistical significance. One key difference between our study and that of Rasmussen et al. is that we used 24-h ABPM rather than a single blood pressure measurement. Recently, the GEM Study, a population-based study, did not demonstrate increased systolic or diastolic blood pressure values in migraineurs compared with controls (20, 21).
There are several possible explanations for the null results of our study. First, it is possible that the sample size was not large enough to demonstrate any difference between the two groups. Secondly, it is possible that some of the differences in arterial blood pressure determined in other studies could be a consequence of misclassification of patients with hypertension based on the inclusion of a high proportion of participants with white-coat hypertension. Our study avoided such misclasssification by using the more precise measurements of blood pressure made possible by the 24-h ABPM during a normal day at home and work. Thirdly, the cut-off points generally used for the definition of high blood pressure, although based on cardiovascular disease mortality, are arbitrary. We viewed blood pressure as a continuous variable, and the 24-h ABPM permits a better evaluation of these measures.
In this study, we used very specific criteria to diagnose chronic daily headache, and included only women presenting with more than 15 days of headache pain each month for more than 6 months, following the definition of chronic daily and near-daily headaches proposed by Silberstein et al. (12). Daily duration of headaches was greater than 4 h. Because women with chronic daily headache had more than one type of headache according to IHS criteria (either migraine headache or tension-type headache) we could not associate blood pressure measures with specific types of headache, but 93.3% of cases were transformed migraine according to Silberstein's criteria (12). However, women with chronic daily headache had pain daily or near-daily, which allowed us a high likelihood of measuring ambulatory blood pressure during a number of headache events.
The limitations of our study were related to the population of patients presenting at a tertiary care hospital. In this population there is an elevated percentage of hypertension and white-coat hypertension compared with the general population. To control for this, however, we used a 24-h ambulatory blood pressure monitoring technique that helps differentiate between white-coat hypertension and true high blood pressure (15, 16). Among the participants with and without chronic headache, the prevalence of true high blood pressure and white-coat hypertension was the same.
This study has practical applications. Among physicians and lay people there is a common belief that high blood pressure and headache are causally connected. If it is true, as prior studies suggested, then a key step in preventing or controlling headache would be controlling hypertension. If there is not a causal association, as our study suggests, then control of hypertension is still important (for cardiovascular risks) but other avenues must be explored for the prevention and control of headache.
In conclusion, in the present study we did not observe any significant difference in systolic and diastolic office blood pressure and in 24-h ambulatory blood pressure monitorization in women with chronic daily headache compared with women without headache.
Footnotes
Acknowledgement
Drs Bensen~or, Lotufo and Martins are recipients of an established investigator award from Conselho Nacional de Pesquisa (CNPq), Brasília, Brazil. The authors thank Patrick Skerrett for his assistance.