
Abstract
Nitrite concentrations in plasma were investigated in a population of migraine and cluster headache patients and a group of healthy non-headache controls. A hundred migraine patients and 69 cluster headache patients in the interictal period, and 112 controls, were studied. Significantly higher nitrite concentrations were found in migraine patients, with and without aura, and cluster headache patients, in remission and cluster phase, than in controls. These findings suggest that a basal dysfunction in the L-arginine-NO pathway may be involved in the peripheral mechanisms predisposing subjects with neurovascular headaches to individual attacks.
Introduction
It has been proposed that nitric oxide (NO) may be the causative molecule of vascular headaches (1, 2). This theory is inspired by the observation that NO donors can provoke headaches similar to spontaneous headaches in migraine and cluster headache patients (3, 4). NO is an ubiquitous messenger molecule synthesized from L-arginine by the NO-synthases that occur in many tissues and cells, including endothelia, brain, peripheral nerves, macrophages, platelets and microglia. NO is an unorthodox neurotransmitter as it diffuses freely through cell membranes; it activates soluble guanylate cyclase to convert GTP to cGMP, and is deactivated within seconds to nitrates and nitrites (5, 6). The L-arginine-NO metabolic pathway plays an important role in many biological processes, some of which could be implicated in the pathophysiology of migraine and ‘vascular headaches’ (1, 2, 5, 6). In particular, endogenous NO may be involved in perivascular neurogenic inflammation (7), thought to be a key process in the mechanisms underlying the pain attacks in both migraine and cluster headache (8–12). The aim of the study was to explore the L-arginine-NO pathway in migraine and cluster headache (CH) by determining nitrite concentrations, the stable components of NO metabolism, in patients' plasma. Blood was sampled from patients during pain-free periods and nitrite levels in plasma were compared with those in a group of healthy controls.
Methods
Patients were recruited consecutively from out-patients presenting at the Regional Headache Center of the C Besta National Neurological Institute. Those eligible had migraine or CH diagnosed according to the criteria of the International Headache Society (13), duration of illness greater than 2 years, and age between 18 and 65 years. None had taken prophylactic medication for migraine or CH for at least the 2 months prior to entering the study. Control subjects had no history of recurrent headache and were aged between 18 and 65 years. The presence of metabolic, renal and gastrointestinal diseases and of treatment with nitro-derivatives was excluded in all patients and controls by history taking and routine blood tests.
We recruited 100 migraine patients (60 migraine without aura and 40 migraine with aura), 69 CH patients (32 in cluster phase, 37 in remission during the study) and 112 healthy controls. The principal characteristics of the participants are summarized in Table 1. All gave their informed consent to take part in the study.
Main characteristics of the studied groups
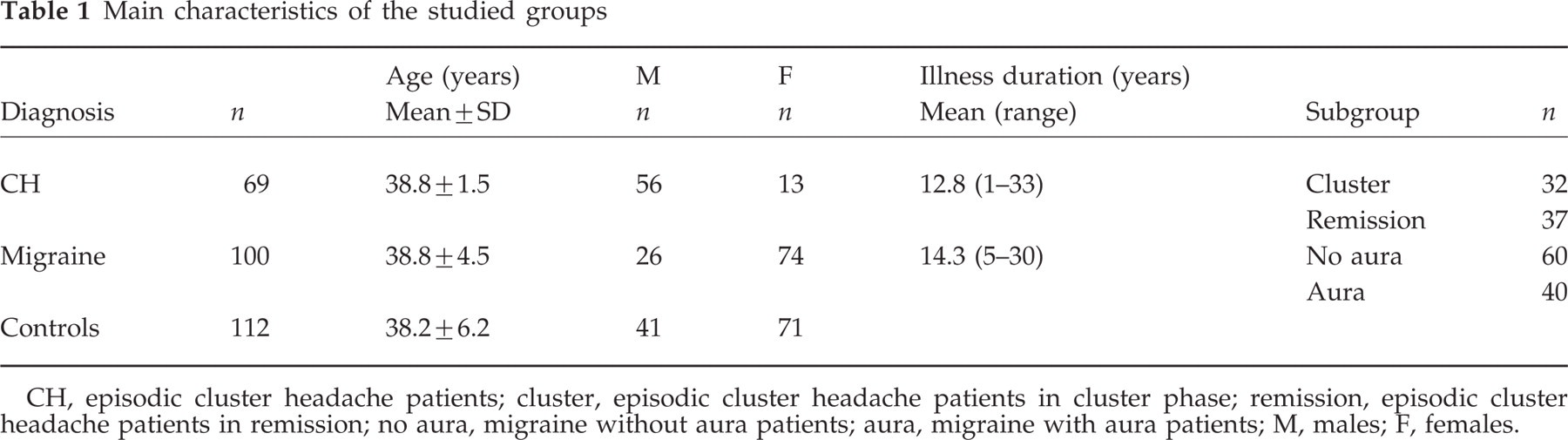
CH, episodic cluster headache patients; cluster, episodic cluster headache patients in cluster phase; remission, episodic cluster headache patients in remission; no aura, migraine without aura patients; aura, migraine with aura patients; M, males; F, females.
Blood samples were drawn from the cubital vein after overnight fast. Each studied subject received a list of potential dietary sources of nitrates/nitrites (e.g. red meat or cured meat) and was instructed to refrain from such foods for at least 48 h before blood sampling. None of the patients were suffering from headache when the sample was taken: for the migraine patients at least 72 h had elapsed since the last migraine, and for the CH patients in cluster phase at least 3 h had elapsed since the last cluster headache. As an estimate of plasma NO we measured plasma nitrites (14). Nitrates (which are other products of the breakdown of NO) were converted into nitrites by treatment of serum with nitrate reductase (Boehringer Mannheim Italia SpA, Milan, Italy). After enzymatic reduction, samples were mixed with equal amounts of Griess reagent (sulphanilamide 1%, naphtylethylenamide 0.1% in phosphoric acid 0.25%). Samples were incubated at room temperature for 10 min, then were centrifuged and the plasma was stored at −80°C pending analysis. Absorbance was measured at 540 nm using a microplate reader.
To assess the significance of differences in plasma nitrite concentration we employed the Mann–Whitney rank sum test. Pearson's test was used to assess correlations between duration of illness and age and nitrite levels. Student's t-test was used to assess nitrite level differences between the sexes.
Results
Nitrite levels in plasma were significantly higher in both migraine and CH patients than controls. When the four subgroups (migraine with and without aura; CH in remission and cluster period) were compared individually with controls, in all cases nitrite levels were significantly higher than in controls. There were no significant differences in nitrite levels between any of the four patient subgroups (Fig. 1).

CH, patients with episodic cluster headache (n = 69); cluster, episodic cluster headache patients in cluster period (n = 32); remission, episodic cluster headache patients in remission (n = 37); migraine, patients with migraine (n = 100); no aura, migraine without aura patients (n = 60); aura, migraine with aura patients (n = 40). P-values calculated by Mann–Whitney rank sum test.
No correlation was found between age and nitrite level (Pearson's test, r = 0.20), nor between duration of illness and plasma nitrite (Pearson's test, r = 0.22 for migraine, r = 0.03 for CH). Furthermore there was no significant difference between men and women in terms of nitrite levels (Student's t-test P = 0.89). The proportion of males and females was similar in controls and migraine patients (chi-square P = 0.13); however, there were significantly more males than females in the CH group than controls (chi-square P < 0.001).
Discussion
Our study has shown that plasma levels of nitrites were significantly higher in migraine and CH patients outside of pain episodes than in a group of healthy controls who did not suffer from recurrent headache and who did not differ from the migraine or CH patients in terms of age (Student's t-test, P = 0.8 in both cases).
The fact that the proportion of males in the CH group was significantly greater than in the controls could represent a bias of our study; however, it is unlikely to have had any effect as nitrite levels in plasma did not differ between the sexes within each patient group and within the control group.
We used plasma nitrite accumulation as an estimate of circulating NO. In fact, endogenous metabolism of NO is known to give rise to nitrites and nitrates (6). As illustrated in ‘Methods’, plasma nitrates were also converted into nitrites and possible dietary and pharmacological nitrite/nitrate sources were excluded. Thus, our findings constitute evidence that the L-arginine-NO pathway is hyperfunctional in migraine and CH patients when they are not undergoing a headache.
Other literature data support this finding. In 1994 D'Andrea et al. (15) proposed that NO synthesis was abnormal in migraine with aura patients, in order to explain the hyper-responsiveness of platelets to collagen stimulation. Gallai et al. (16) demonstrated increased basal and collagen-stimulated production of NO and cGMP in platelet cytosol of migraine with aura patients (n = 35) and to a lesser extent in migraine without aura patients (n = 45), indicating that the platelet L-arginine-NO pathway was hyperactive both during attacks and outside of attacks. Sarchielli et al. (17) also found that the L-arginine-NO pathway was hyperactive in the platelets of 40 female migraineurs (without aura) during attacks and also outside of attacks. Martelletti et al. (18) found increased nitrites in serum and peripheral blood mononuclear cell supernatants during NO donor-induced migraine attacks and also outside of attacks. Nitrite levels in CH patients are less well documented in the literature and the only relevant study is that of Martelletti et al. (19), who found high levels in serum and peripheral blood mononuclear cell supernatants in 12 CH patients during spontaneous and NO-donor-induced cluster headaches, but not outside attacks (19).
As noted in the introduction, several studies suggest a relation between NO and the phenomenon of neurogenic inflammation, which appears to be key step in the development of neurovascular headaches (8, 12). Neurogenic inflammation is characterized by the release of the various vasoactive peptides, such as GRP, from trigeminal perivascular nerve endings (trigemino-vascular system), to produce vasodilatation, plasma protein extravasation around cranial blood vessels, and sensitization of perivascular sensory afferents leading to increased transmission of nociceptive information to the brainstem (8–12). There is evidence that NO stimulates the release of CGRP from perivascular trigeminal terminals in cats (7), while other studies on animals indicate that NO can directly induce plasma protein extravasation at the level of the dura mater (20). An increase in CGRP levels within the blood of the external jugular vein has been reported during spontaneous migraine attacks and also during NO-donor-induced CH headaches (10–12). Other studies, however, have cast doubts on this scenario. Edvinsson et al. (21) did not find that endogenous NO was important in trigeminal fibre-mediated dilatation of cerebral blood vessels in the cat, while the lack of increased extravasation (by angiography) in the human retina during migraine attacks (22) and lack of anti-migraine efficacy of potent blockers of neurogenic inflammation (23, 24, 14), suggest that neurogenic inflammation may not be involved in the pathophysiology of primary headaches.
Our data indicate a basal hyperactivity of NO-producing mechanisms in migraine and CH patients. According to the synthesis of migraine mechanisms proposed by Olesen and Goadsby (25), it can be hypothesized that many factors are involved in the pathogenesis of neurovascular headaches: genetic factors, environmental predisposition, interictal physiological/biochemical traits, precipitating factors, and pain expression. We suggest that hyperactivity of NO-producing mechanisms may be one of the biochemical abnormalities that are present outside attacks in patients with migraine and CH. In these subjects several precipitating factors (e.g. menstruation and some foods in migraine, alcohol and variations of light/dark cycles in CH) could aggravate one or more of these abnormalities. L-arginine-NO pathway hyperactivity could be enhanced directly or via increases in neurotransmitter concentration by some known headache triggers (26) (e.g. administration of NO donors in both migraine and CH, hormones in migraine, alcohol in CH), giving rise to the individual attacks.
In conclusion, our findings in ample-sized groups of migraine and CH patients compared with controls suggest that NO could be involved not only in the headache phase, but also in the mechanisms underlying susceptibility to migraine and CH.