
Abstract
The study aim is to describe the long-term clinical outcome of 102 chronic headache patients with analgesic daily use. They were assessed for daily drug intake (DDI), headache index (HI) and quality of life (QoL) and compared with a parallel group of patients with active chronic daily headache but no analgesic overuse. For the primary study group, baseline 1995 DDI was 1.80 ± 1.87 and did not differ significantly in 1999. Patients who daily continued to use analgesics had a higher 1995 baseline DDI (t = 2.275, P = 0.025), a longer drug abuse history (t = 2.282, P = 0.025) and a higher DDI (t = 4.042, P < 0.001) 4 years later. At 4 years of follow-up, only one-third of patients initially treated for chronic daily headache and analgesic overuse are successful in refraining from chronic overuse. Those subjects appear to have a persistence for combination analgesic agents; however, their QoL is slightly better than that of patients who revert to episodic headache or continue with chronic daily headache but do not overuse analgesic agents. Persistent analgesic overuse seems to be linked to the length of abuse and to the number of drugs ingested.
Introduction
Chronic daily headache (CDH) implies headaches that recur daily or near daily for months or years. The clinical features of CDH are extremely variable and the syndrome may encompass a number of divergent subtypes (1, 2). The current International Headache Society (IHS) classification system does not seem to offer an adequate niche for even the more common subtypes of CDH encountered in clinical practice (3). This deficiency of classification accounts for much of the difficulty involved in designing epidemiological, therapeutic and pathophysiological studies (4). The biology of CDH is still a matter for debate and there are various hypotheses regarding the relevance of central neurotransmitter involvement (5, 6). The incidence of chronic headache suggested by more recent investigations is around 3% of the general population (7).
Analgesic overuse is believed to play a major role in promoting CDH (8), but there is a wide variation in the reported prevalence of CDH associated with drug overuse (9, 10). Walker (11) reported a 53% incidence of analgesic rebound in CDH patients evaluated at a community hospital, but European headache centres have reported an incidence as low as 5–10% in CDH patients (12). Such discrepancy may reflect the lack of widely accepted criteria for this diagnosis; revisions of the existing criteria have been suggested by several investigators (13, 14). A number of studies have examined the neurophysiological and clinical outcome of CDH patients following withdrawal from chronic analgesics, and the reported rates of therapeutic success have varied between 47% and 91% (11, 14–22). In most studies the follow-up period lasted less than 12 months and the term ‘drug abuse’ usually was not defined in accordance with the IHS criteria.
The aims of the present study are: (i) to evaluate the clinical outcome of 102 patients treated 4 years ago for CDH and analgesic overuse, comparing the characteristics of those who were daily analgesic over-users and those were not; (ii) to identify possible prognostic factors with regard to analgesic consumption and evaluate the impact of analgesic use on quality of life.
Materials and methods
Our primary study group was comprised of 102 consecutively chosen subjects affected both by CDH and analgesic overuse in 1995, whom we had re-evaluated between November 1998 and April 1999, at that time examining the efficacy of different therapeutic approaches for reducing drug reliance (22). We collected information regarding headache frequency, daily drug intake (DDI=average number of analgesic doses per day, including analgesics sold with medical prescription and over-the-counter pills, only in cases of mixtures but not herbal or homeopathic products) and quality of life. Analgesic overuse was defined as use of at least one painkiller pill or suppository per day for 1 year or more. We evaluated the impact of headache with a modified headache severity index questionnaire (23), and quality of life by using the Migraine Quality of Life Questionnaire (MQoL) (24).
In this study we report the SF-36 results. The available data have been compared with the data sampled on the same subjects in 1995. Only 21 men and 69 women (mean age: 50.1 ± 12.5 years; 58.89% affected by migraine, 41.11% affected by chronic tension-type headache, CTTH; mean overuse length in 1995: 15 ± 13.6 years) adequately completed the interviews and were evaluated. For age-matched controls, we evaluated six men and 21 women (mean age: 53.0 ± 19.8 years; 62.96% affected by migraine, 37.04% affected by CTTH) not taking analgesics daily, and the same parameters were measured. To reduce the variability of answers to the item about the starting headache type, it was categorized as migraine-type headaches or as tension-type headaches; other specifications could be misleading, because the information for this item often refers to symptoms felt decades in the past. The analgesic over-users were admitted to the headache centre day hospital at least once during the observation period.
Data were collected by phone interview or during a visit to our headache centre and then entered into a computerized registry and analysed by SPSS 6.1.2, version for Window 95, statistical software. The Kolmogorov-Smirnov test was applied to assess the normality of the studied continuous data.
Results
In 1999, 94% of the studied subjects had overlapping primary diagnoses. Table 1 reports the main characteristics of daily and not daily analgesic over-users with regard to mean time from symptoms beginning (years) and mean time from analgesic overuse beginning (years). Patients who daily continued to use analgesics had a higher 1995 baseline DDI (t = 2.275, 88 d.f., P = 0.025), a longer history of drug abuse (t = 2.282, 88 d.f, P = 0.025) and a higher DDI (t = 4.042, 88 d.f., P < 0.001) 4 years later. No sex-related significant difference was observed among studied parameters. Moreover, no significant difference was found with regard to the prophylactic treatment between analgesic non-over-users and over-users as well as between the 1995 and 1999 surveys. Almost one-third of the analgesic over-user patients stopped the overusing habit during the follow-up.
Demographic data related to the daily use of analgesics
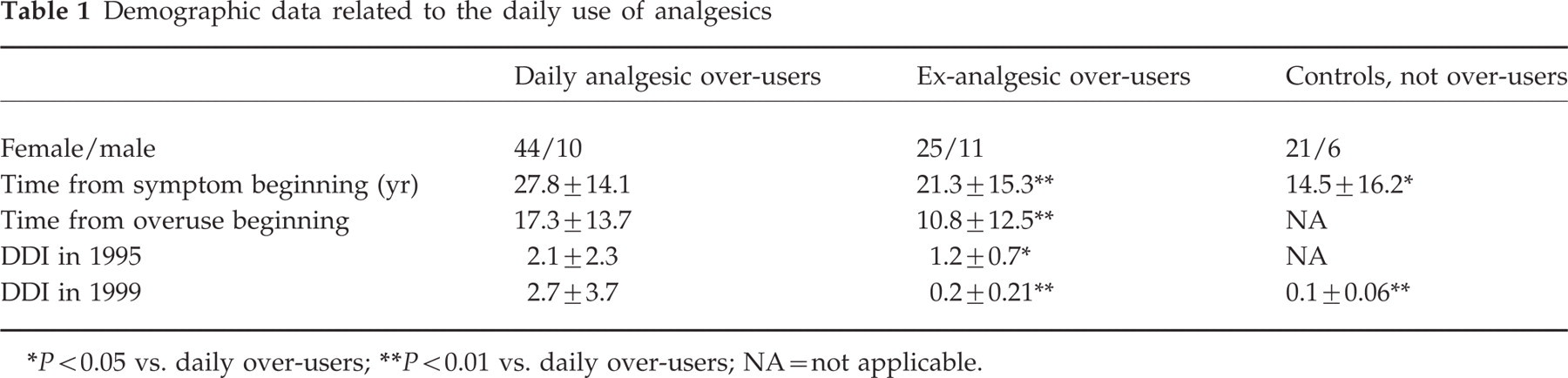
∗ P < 0.05 vs. daily over-users;
∗∗ P < 0.01 vs. daily over-users; NA = not applicable.
Table 2 reports on the types of analgesic abused. Changes in drug-dependency in the observation period are reflected in the number of patients abusing the drug at the outset as opposed to the end of the observation period. The patient pattern of drug abuse during follow-up and the change in the type of drug abused are reported in Table 3. The DDI of daily analgesic over-users significantly increases between 1995 and 1999 (P < 0.01), while the DDI of ex-over-users significantly decreased (P < 0.01). The quality of life and the severity of headache are the main considerations in evaluating the impact of this disease on the patient's life. The QoL measured in 1999 is significantly lower in ex-over-users (40.3 ± 5.12) than in daily analgesic over-users (48.5 ± 6.12) and control subjects (56.0 ± 2.8; P < 0.05), while no relevant difference among groups was found in the Headache Severity Index as quoted by Von Kroff (P > 0.05). The QoL value in relation to the diagnosis at the onset of headache is reported in Fig. 1. Once again, no sex-related significant difference was observed among studied parameters.
Patterns of drug overuse

∗Butalbital+propiphenazone+caffeine association.
†Indometacine+prodorperazine+caffeine association.
The time-patterns in abused drugs
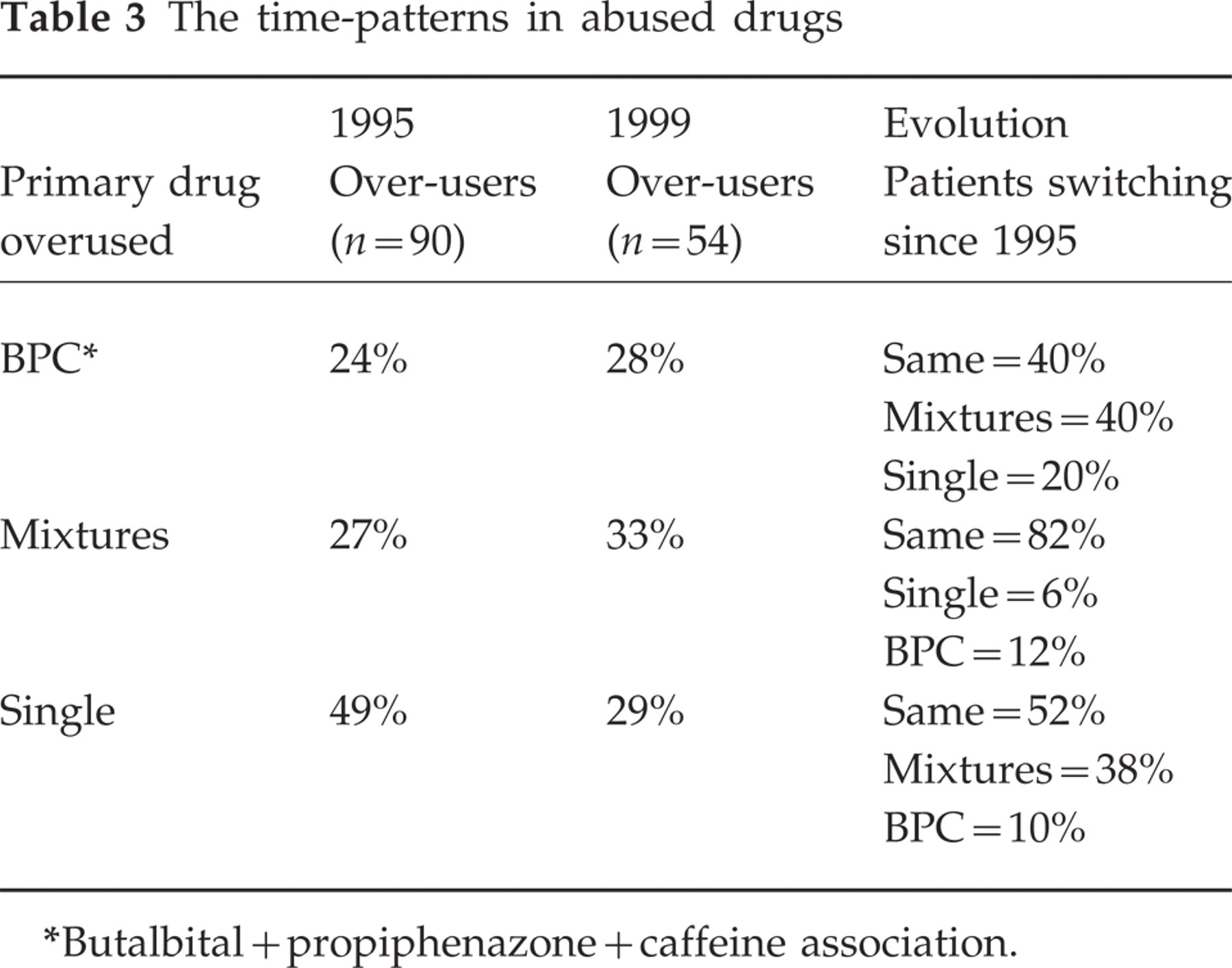
∗Butalbital+propiphenazone+caffeine association.

QoL value with respect to the headache type diagnosis (□ migraine, () CTTH) at the symptom onset (∗P < 0.001 vs. daily analgesic over-users).
It is interesting to note that there is a significant correlation between QoL and analgesic overuse duration (c.c. 2804, P < 0.05). A similar effect was found for both over-users and ex-over-users. However, distinguishing between migraine and CTTH affected, it is noteworthy that the first patients show an improvement in QoL with the persisting of analgesic overuse, while the CTTH patients' QoL decreases progressively with the duration of overuse (Fig. 2).

Analgesic overuse length and QoL in patients diagnosed with migraine (□, – – –) and CTTH (▪, ) at the symptom onset: linear regression lines. ( ) Total poulation.
Discussion
This follow-up study compared the 90 patients in 1999 with a group of non-abusers suffering from CDH and comparable for sex, age and diagnosis at the onset.
The overall values of DDI did not change significantly after 4 years; when patients were interviewed, we found that a third of them no longer used daily anti-migraine drugs nor reported daily headaches. We therefore decided to regard these patients as a separate group in order to highlight the possible differences between them and the patients still taking drugs on a daily basis. The demographic data of the latter patients showed significant differences in the duration of their headache history and in the length of their daily use of drugs. This group of patients also differed significantly in 1995 from other patients, on account of their reduced DDI. These data suggest that patients with a longer history of headache and of daily drug use, associated with a higher rate of drug consumption, are at greater risk of remaining habitual abusers and of suffering from daily headache.
Prophylactic treatments, as administered in day hospitals and outpatients departments, seem to have little influence on the evolution of CDH, thus confirming previously reported data regarding the outcome of similar patients after a 3-month follow-up (22). A number of these patients also underwent non-pharmacological treatment (psychotherapy and/or physiotherapy) but the data were not valid because of the differences in the type, length and reproducibility of the treatment involved. Moreover, there was a marked consistency in drug use during the follow-up period, suggesting that no new therapeutic strategies were implemented in that time.
Another crucial point was to determine the influence of the type(s) of drug in daily use and the relevant pattern of use over time. The patient habitual preference for a given drug or drug combination could determine the role of the single drug in maintaining the abuse. Drug-switching could indicate a habitual tendency to abuse drugs or use them frequently or (more simply) a lack of their efficacy in reducing pain, and mask the pharmacological role of individual drugs. In Table 3 we report the proportion of patients sticking to a single drug or drug mixture during the 5-year observation period, the patterns of drug abuse during follow-up and the change in the type of drug abused. For this purpose, we collected the mixtures with the association indomethacine + prodorperazine + caffeine (IPC), which we previously kept separate because it is a typical Italian market phenomenon. The association butalbital + propiphenazone + caffeine (BPC) was considered separately because it contains barbiturates. All other drugs such as NSAIDs, ergot and triptans, containing only one pharmacological active compound, were collected.
At 4 months follow-up we reported that patients taking barbiturate-containing mixtures relapsed into daily use more than others did. The 4-year follow-up confirmed this point with some differences: the percentage of patients daily using barbiturate-containing mixtures did not change significantly among abusers, whereas it decreased, though not significantly, in ex-over-users; however, 40% of these patients were daily taking the BPC drug association and almost the same percentage of patients had changed to other mixtures. Patients using mixtures in 1995 did not change their type of drug and in 80% of cases continued as drug-abusers. Only in the case of patients using drugs containing a single active compound was there a drop in the number of abusers and a corresponding increase in the number of ex-abusers. No significant difference was observed in the daily drug use overall pattern. When we compared the evolution of individual patients, we noticed a marked shift to mixtures of both barbiturates and prochlorperazine-containing drugs during the follow-up period; only half of the patients using single preparations maintained this preference. By contrast, as many as 90% of patients using mixtures daily did not change to single compounds.
The quality of life (QoL) of our patients was evaluated by the SF-16 (24, 25) and the Headache Severity Index (23). Both indexes proved consistent. Analysis of the relationship between the QoL and the duration of the disease in patients suffering from chronic tension-type headache without drug use (c.c. 0.17; P < 0.05) was negative, and in the same group the QoL and the severity of headache showed poor correlation (c.c. 0.366; P > 0.05). Interestingly, patients no longer taking drugs on a daily basis had a significantly worse QoL with regard both to analgesic over-users and CTH sufferers (P < 0.005). Daily drug users recorded a better score than CTH patients, whereas the HSI were similar. This datum seems to indicate that drugs taken daily serve to improve the patients' QoL, even though the severity of headache may be similar.
As reported in Fig. 1, there was no difference in the diagnosis of the two groups at the outset, but a correlation could be shown with the QoL and the diagnosis at the onset. Patients suffering from migraine scored higher in QoL than patients suffering from TTH (P < 0.05) in the group of patients no longer abusing drugs. There were no significant differences between non-abusers and abusers, in agreement with data reported by Monzòn (26). Physical role and social functioning are more affected in headache patients than in other chronic diseases (27), and this is also reflected in our data on patients not abusing drugs.
Conclusion
Our main findings are: (a) a majority of patients with CDH who are treated for that condition are able to refrain chronically from overuse; (b) chronic analgesic use in CDH patients may be associated with a better QoL than is reported by CDH non-over-users, despite no difference in HI; (c) over-users are particularly faithful to combined analgesics.
Thus, two conclusions can be drawn: first, prophylactic drugs, as administered in day hospitals and outpatients departments, have little influence on the evolution of CDH; secondly, there is a marked tendency to favour mixtures, both barbiturates and percholperazine-containing compounds, which seems to suggest that small doses of central acting drugs contribute in some way to the reinforcement of drug abuse.
The QoL seems to be affected by daily drug use, unexpectedly showing a higher value in patients daily taking analgesics than in ex-over-users, but not higher than in the control group. It is interesting to note that patients who use analgesics say that they improve their quality of life. However, this finding is not confirmed by the HI, which is almost identical among the studied patient groups. These scores improve, as expected, when the headaches reduce in frequency and there is a corresponding reduction in drug use in the group of patients no longer taking drugs on a daily basis. The type of headache at the outset does not seem to influence the follow-up (58% vs. 59%) with respect to the persistence of drug use. Patients not using drugs displayed a significantly better QoL when starting with a tension-type headache, whereas the QoL profile of transformed migraine sufferers worsened.
Finally, the present data suggest that long-term analgesic overuse by patients with CDH will persist in the majority despite aggressive treatment intervention. Duration of CDH, number of analgesics daily ingested and initial CDH subtype appear to predict long-term overuse. Analgesic overuse may be associated with a higher self-reported quality of life relative to non-overusing CDH patients and, as such, this pattern of medication use does not fulfil the DSM IV-R criteria for abuse. As their treating clinicians, we should admit the possibility that frequent analgesic use not infrequently may assist in improving the lives of these unfortunate patients.