
Abstract
Chronic daily headache (CDH) represents a challenge in clinical practice and the scientific field. CDH with onset in children and adolescents represent a matchless opportunity to understand mechanisms involved in adult CDH. The aim of this study was to evaluate the diagnosis, prognosis and psychiatric co-morbidity of CDH with young onset in the young. Fifty-nine CDH patients has been followed from 1997 to 2001 in our department. Headache and psychiatric diagnoses were made on the basis of the international system of classification (International Headache Society, 1988; DSM-IV). X2 test and multinomial logistic regressions were applied to analyse factors predicting outcome. The current diagnostic system allows a diagnosis in 80% of CDH patients, even if age-related characteristics have been evidenced. Psychiatric disorders are notable in CDH (about 64% of patients) and predict (mainly anxiety) a poorer outcome. Surprisingly, analgesic overuse is not involved in the chronicization process. Diagnosis of CDH needs further study. Psychiatric disorders predict a worse outcome and greater account should be taken of them in treatment planning.
Introduction
Chronic daily headache (CDH) represents a frequent and problematical challenge both in adult and paediatric clinical practice.
The prevalence of childhood and adolescent CDH ranges from 0.2 to 0.9% (1, 2). The prevalence in the adult population varies between 1.5 and 7%(3–5). The prevalence of CDH in clinical practice ranges from 15 to 20% of patients (6).
Many points in the aetiology, diagnosis and treatment of CDH need to be clarified. The diagnosis of CDH is based on a quantitative parameter (the almost daily frequency of the crises). We do not have clear qualitative parameters (a certain symptomatologic characterization of the crises), while a common system of classification is still lacking both in adults and in children and adolescents, even if proposals have been attempted (7–20).
In adults, the International Headache Society criteria (IHS, 1988) defined chronic tension-type headache (CTTH) as attacks occurring at least 15 days per month over a period of at least 6 months (21). Head pain is described as mild to moderate in severity, pressing or tightening in quality, bilateral and not worsening with physical activity. In adults, Silberstein's classification (7, 8) represents the first attempt to achieve a better systematization of the diagnosis of CDH, by the proposal of categories to classify primary and secondary varieties of CDH. According to Silberstein's classification the primary varieties (each with or without drug overuse) of CDH are:
Transformed migraine– There is a history of episodic migraine, with or without aura, in teens or twenties with episodic migraine and subsequent development of CDH. It is often difficult to distinguish between headache subtypes. These patients frequently have a family history of migraine, menstrual aggravation, identifiable trigger factors, and unilateral headache.
Chronic tension-type headache– Patients may have a history of episodic tension-type headache or it may begin de novo; they meet IHS criteria for CTTH; the headaches are more often diffuse and bilateral, frequently involving the posterior part of the head and neck, and may have some migrainous features. The major difference from transformed migraine is the absence of a clear history of episodic migraine.
New daily persistent headache– Patients may refer to fairly rapid onset, some remember the exact day or time when the headache started. Head pain is continuous, and there is no clear history of episodic migraine or tension-type headache; the patients are generally younger than those with transformed migraine.
Hemicrania continua– Continuous but fluctuating, moderately severe, unilateral headache that may alternate between sides, phono-/photophobia, nausea, and tearing. It cannot be triggered by neck movements, but tender spots may be present on the neck. It is an indomethacin-responsive headache disorder, and may occasionally be associated with autonomic disturbances, such as ptosis, mydriasis and sweating. The latter are post-traumatic headache, cervical spine disorder, headache associated with vascular disorders, headache associated with non-vascular disorders, and others.
Findings on the clinical characterization of CDH in children and adolescents are unclear. The application of Silberstein's model in the youngest age group does not give us an exhaustive diagnostic framework, leading to the hypothesis of specific symptomatological expression of CDH in children and adolescents. By the application of Silberstein's criteria (8), Gladstein and Holden (15) found that 35% of children and adolescents did not fit into these categories. However, by adding the category they called ‘co-morbid’ (migraine crises in co-morbid association with tension-type headache), all but one of 37 patients could be classified according to Silberstein's 1994 criteria.
According to Abu-Arefeh's findings (18), the IHS criteria for classifying chronic headache seem to apply even to the youngest, with all patients meeting the diagnostic parameters (70.6% with CTTH and 30.4% with CTTH and migraine without aura). No data support the hypothesis of a probable transformation of migraine or episodic tension-type headache to CDH, as suggested for adults (7, 8). Hershey et al. (17) found that 27% of CDH patients could not be classified according to IHS criteria. They underlined the predominance of migrainous characteristics of CDH in children and highlighted a temporal trend of the crises: frequent, daily intermittent and daily continuous headache. Migrainous characteristics of CDH in children have been evidenced and hypothesized to be related to the transformation of migraine over time, according to that suggested for adults (7, 8).
Recently, Koenig et al. (20) suggested the existence of a single CDH syndrome in children and adolescents, characterized by migrainous features in the worsening periods, rather than two coexisting primary headache disorders.
The prevalence of psychiatric disorders is greater in CDH patients than in other headache patients. Estimates of the prevalence of psychiatric co-morbidity in CDH patients range from 64–66.1% (22, 23) to 90% (24), mostly anxiety and/or mood disorders, with higher scores in women than in men with CDH (25, 26). A similar trend has been found in children and adolescents with CDH (6). Holden et al. (14) found a higher rate of psychiatric disorders (46%) in CDH compared with migraine (17%). According to Abu-Arefeh (18), 51% of CDH patients had ‘at least one significant health problem, family illness or stressful family event that preceded or coincided with the onset of CTTH’.
The presence of psychiatric co-morbidity is related to the chronicization of headache (27) and may make therapy more difficult (28, 29), making it necessary to assess and treat it as early as possible.
CDH with developmental age onset represents a unique opportunity to monitor the trend of the attacks over time, in order to identify the factors most probably involved in maintaining headache crises. In adults, stress has been placed on the role of analgesic overuse in the exacerbation and maintenance of headache over time (30–33). The examination of CDH with juvenile onset may clarify several aspects of adult CDH, related or not to ‘rebound headache’, offering a ‘purer’ basis for clinical investigations compared with adult ages. However, ‘rebound headache’ has been described even in paediatric age, even if mainly as case reports (34–36).
In adult migraineurs, the use of over-the-counter medication ranges from 60 to 90% (37, 38). Overuse may predispose to CDH, with symptomatic drug dependence and refractoriness to prophylactic medication (39).
It is essential to analyse the factors involved in the chronicization and prognosis of headache. The role of analgesic overuse cannot explain all the cases of CDH, as has been shown by the cases of CDH with onset in children or adolescents, in as much as only a minor percentage seem to be related to it (34–36).
We addressed four aims: (i) applicability of IHS criteria in child and adolescent CDH; (ii) analysis of psychiatric co-morbidity in CDH patients; (iii) analysis of the trend of CDH according to the presence of psychiatric disorders in a 4-year follow-up; (iv) analysis of the presence of analgesic overuse.
Materials and methods
Subjects
Fifty-nine CDH patients [37 female, 22 male; age 11.19 ± 2.4 years (mean ± SD); range 7–17 years] were enrolled from 312 subjects (155 female, 157 male; age 10.3 ± 2.9 years; range 4–18 years) first seen in our Child and Adolescent Headache Centre in 1997. The participants were selected on the basis of the frequency of headache attacks (>15 days/month for at least 3 months).
Headache diagnosis
CDH has been classified according to the IHS by means of a clinical structured interview. Even if other systems of classification have been advanced for classifying CDH with onset in children and adolescents (14, 17), we applied the IHS criteria, since it still represents the most common system of classification. The suitability of IHS criteria to diagnose CDH in the very young has been outlined recently (18).
CTTH, episodic or CTTH and migraine without aura, and CDH meeting all diagnostic criteria but one were taken into account, even though the diagnoses were made on the basis of 3 months’ duration. Studies on CDH with onset in children and adolescents have suggested reducing the ‘duration’ criterion for CTTH from 6 to 3 months (18). Furthermore, the proposal for the new IHS classification (in press) considers 3 months as such a criterion.
Compared with the first attenders, we assessed the evolution of headache after 4 years. The variable headache condition in 2001 (two levels: headache-free/headache sufferers) was computed considering as headache-free those subjects for whom headaches had been present less than once per month during the last 2 years, while subjects for whom headaches had been present once or more then once per month during the last 2 years were classified as headache sufferers.
In order to evaluate mild modification of headache pattern, a subclassification of headache sufferers was computed on the basis of the comparison between frequency and the intensity of headache attacks in 1997 and 2001. In both the structured interviews, the subjects were requested to rate the intensity of attacks on a graded scale at three levels of severity (0, continuation of daily activities; 1, interruption of activities; 2, the patient goes to bed and in the dark) and to report the number of attacks in the last 6 months. A minor/major self- reported impact on daily activities or a frequency lower/higher than 50% to the initial one were considered as an improvement. According to these two criteria, the variable follow-up (three levels: headache free, improved headache, stable–worsened headache) was computed. We considered improvement or worsening of headache if at least one criterion (frequency or intensity) had undergone variation. Unchanged headache was recorded when none of the characteristics of headache had changed. Subjects with attacks less than once per month during the last 2 years were classified, as above, headache free.
Psychiatric diagnosis
During 1997, all subjects were assessed for psychiatric co-morbidity (P-CO) by means of clinical interviews (with parent, child or adolescent) and with the aid of psychometric tests. TAT (Thematic Apperception Test) or CAT (Children Apperception Test) according to age, PIC (Personality Inventory for Children) and STAI-C (State-Trait Anxiety Inventory for Children) were administered. Combining the psychometric and clinical results, an expert clinical psychologist (F.G.) performed the diagnoses according to diagnostic criteria on Axis I of DSM-IV (40). The disorders occurring were the following:
Disorders usually first diagnosed in infancy, childhood or adolescence (enuresis, encopresis, tic disorder, separation anxiety disorder).
Sleep disorders (nightmare disorder, sleep terror disorder, sleepwalking disorder, breathing-related sleep disorder, dyssomnia not otherwise specified).
Anxiety disorders (generalized anxiety disorder, attention deficit/hyperactive disorder, conduct disorder, social phobia, specific phobia).
Mood disorders (major depressive disorder, dysthymic disorder, depressive disorder not otherwise specified).
Eating disorders (anorexia nervosa, bulimia nervosa).
Adjustment disorder (unspecified).
We considered all the sleep, anxiety and mood disorders as most represented in our sample. For each of these three categories of disorders, a dichotomic variable (presence/absence) was computed. The variable ‘other disorders’ (two levels: presence/absence) refers to all the other psychiatric disorders that were pooled together because of the slight prevalence in our sample (see below).
In order to point out the more general interaction of psychopathology in 1997 with the evolution of headache, we also considered three comprehensive categories of P-CO in 1997: (i) absence of disorders, (ii) presence of a single psychiatric disorder, and (iii) presence of multiple disorders.
Patients with multiple psychiatric disorders received indications for treatment with brief psychotherapy (41).
Analgesic overuse
Having no common diagnostic parameters for classifying it, we considered as analgesic overusers patients who took analgesic drugs for each attack over the period of 6 months (even before the diagnosis of CDH).
Statistical analysis
A χ2 test was used to test for significance of association of frequency data. This is used to test whether there is any association between the row variable and the column variable, to estimate whether the distribution of frequencies among categories of one variable is independent of their distribution among the categories of the other. Data were cross-tabulated and χ2 were computed for each comparison in a two-way table. On the other hand, in order to analyse multiway frequency tables (more then two variables) for evaluating the presence of two-way interaction effects of P-CO disorders in 1997 (anxiety disorders × sleep disorders, anxiety disorders × other disorders, sleep disorders × other disorders) on follow-up in 2001, multinomial logistic regressions were computed, in which follow-up was the dependent variable, and the P-CO categories were the predictors. It should be stressed that, in multinomial regression, χ2 values are computed as the change in the value of 2-Log-likelihood value if the tested effect is removed from the model: significant χ2 values indicate that an interaction between independent variables (predictors, P-CO in 1997) significantly influences the dependent variable (criterion, follow-up).
Results
CDH typology
Three subtypes of CDH were identified according to IHS criteria: 20 (34%) subjects were classified as CDH–CTTH; 28 (47%) as CDH–migraine without aura and episodic or CTTH), 11 (19%) as CDH-not classified according to IHS criteria.
CDH with chronic onset were 58%. CDH with later transformation from episodic to daily crises were 42%.
No gender differences (χ2 = 1.8; d.f. = 2; NS) were found among these three subtypes of CDH.
Psychiatric co-morbidity in 1997
The clinical situation in relation to the psychiatric diagnoses is summarized in Table 1. Of 39 (66.1%) subjects with P-CO in 1997, 39 had a single disorder, 16 had multiple disorders. 20 subjects (33.9%) did not have any psychopathological disorder.
P-CO in 1997 among chronic daily headache subtypes

CDH, Chronic daily headache; CTTH, chronic tension-type headache; ETTH, episodic tension-type headache; MOA, migraine without aura; NC, not classified; P-CO, psychiatric co-morbidity.
The most frequently diagnosed co-morbid disorders in 1997 were sleep (44.1%) and anxiety disorders (22%). No difference was found among groups in the presence of a singe or multiple P-CO. The only significant statistical difference in P-CO among groups was found for sleep disorders (χ2 = 7.4; d.f. = 2; P = 0.02]. Post-hoc comparisons showed that this difference was due to a smaller prevalence (1/10) of sleep disorders in CDH–not classified (NC) than in both the other groups.
Evolution of headache in 2001
Of the 59 subjects seen in 1997, 17 (28.8%) were headache-free while 42 (71.2%) were still headache sufferers. Of the 42 headache sufferers, for 35 (59.3%) there was an improvement in the frequency and/or the intensity of the attack, while for seven (11.9%) of the patients headache frequency and intensity remained stable. No subjects reported a worsening in intensity or frequency of headache attacks. A detailed description of the follow-up results among the three CDH groups is given in Table 2.
Follow-up among the three chronic daily headache (CDH) groups

CTTH, Chronic tension-type headache; ETTH, episodic tension-type headache; MOA, migraine without aura; NC, not classified.
A more careful examination of Table 2 shows that the most frequent improvement of CDH was reduction in the frequency of the attacks, as reported by 34/35 of the subjects. It is noteworthy that only 1/35 reported a reduction in the intensity but not in the frequency of the attacks. No difference was observed in the evolution of headache among groups (χ2 = 0.69; d.f. = 4; NS).
P-CO in 1997 and evolution of headache in 2001
Table 3 reports the clinical evolution of headaches in 2001 in relation to P-CO in 1997. The presence of a psychiatric disorder in 1997 was significantly related to the persistence of headaches (χ2 = 3.86; d.f. = 1; P = 0.05). In particular, 9/20 (45%) of the subjects who were diagnosed to be without any psychiatric disorders in 1997 were headache-free in 2001; while only 8/39 (20.5%) of the subjects who were diagnosed to be with one/any psychiatric disorders in 1997 were headache-free in 2001.
Evolution of headache in relation to P-CO in 1997
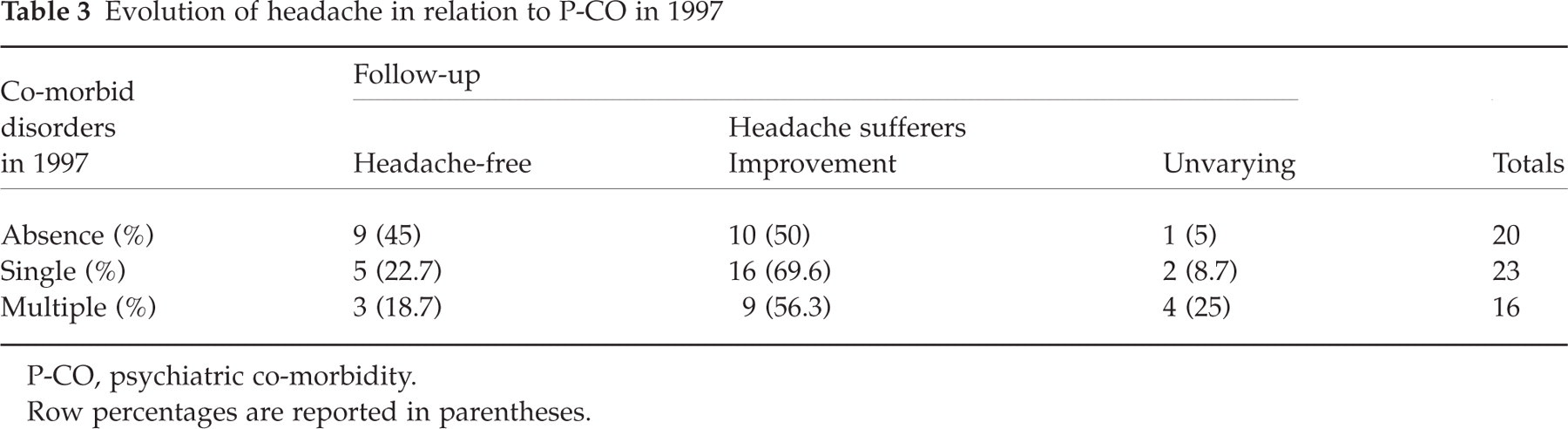
P-CO, psychiatric co-morbidity.
Row percentages are reported in parentheses.
If we consider the correlation between the number of psychiatric disorders diagnosed in 1997 (three levels: no disorder, single disorder and multiple disorders) and the follow-up in 2001 (three levels: headache free, headache sufferers with improvement, headache sufferers without improvement), a significant γ correlation coefficient was found (γ= 0.433; P = 0.026): with the increase in the number of psychiatric disorders there is an increasing probability that their diagnosis will be maintained without improvement.
In order to analyse which psychiatric disorder, diagnosed in 1997, predicts the follow-up, χ2 tests were conducted. Only anxiety disorders (see Table 4) significantly influenced follow-up (χ2 = 6.15; d.f. = 2; P = 0.046).
Anxiety in 1997 and follow-up
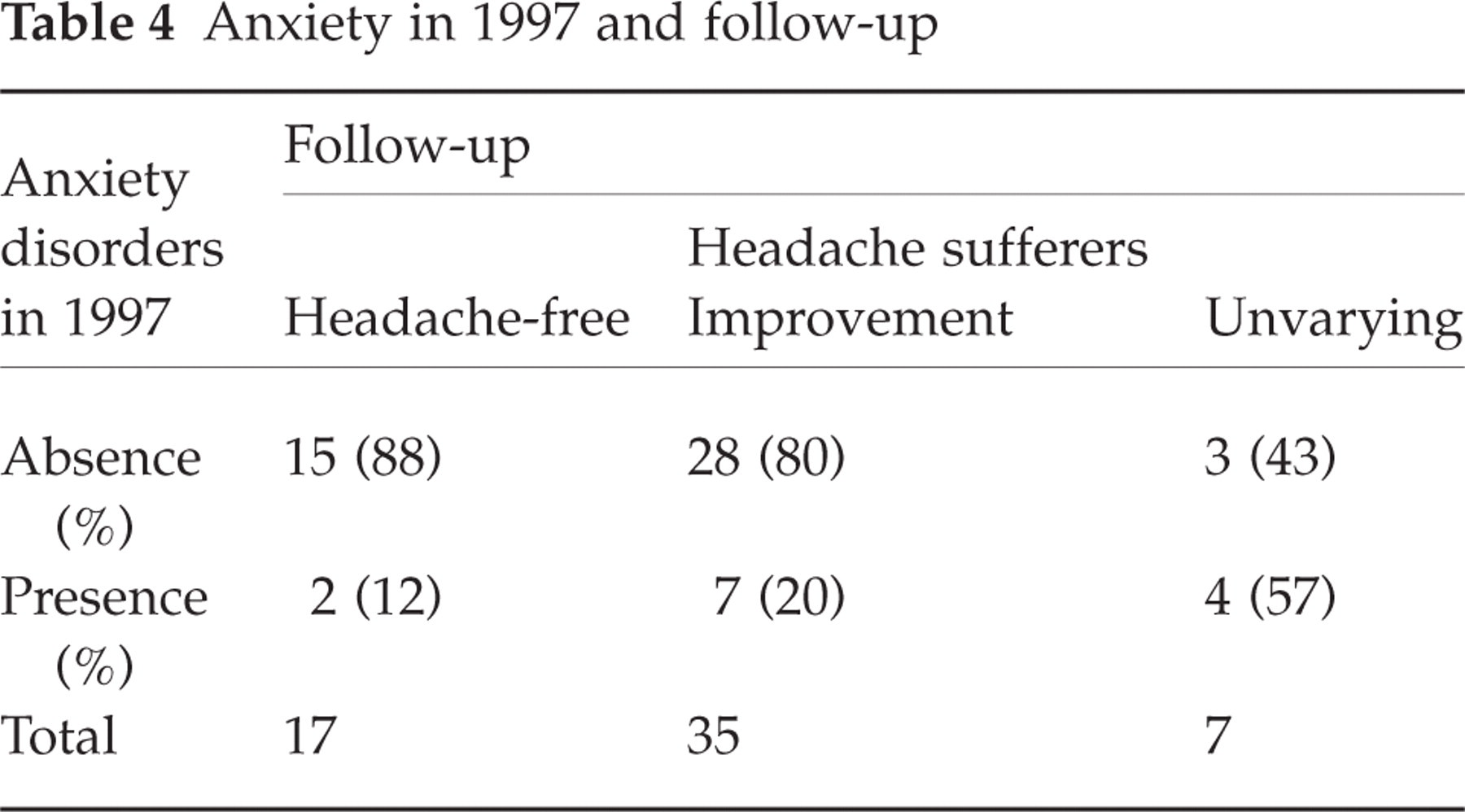
Considering the other psychiatric disorders diagnosed in 1997, follow-up was not significantly influenced by sleep disorders (χ2 = 1.98; d.f. = 2; NS) and other disorders (χ2 = 0.08; d.f. = 2; NS) did not significantly affect the headache condition in 2001. In respect of depression in 1997, it should be specified that the low number of patients with depression did not allow a statistical test to be carried out; however, it is noteworthy that none of the four depressed patients was headache free in 2001.
In order to evaluate possible interaction effects between psychiatric disorders, we tested the effects on follow-up of the two-way interaction (between predictors) by means of a multinomial regression analysis. None of the two-way interaction effects between disorders was shown to influence the follow-up significantly: anxiety disorders × sleep disorders (χ2 = 3.72, d.f. = 2; NS), anxiety disorders × other disorders (χ2 = 2.26, d.f. = 2; NS), other disorders × sleep disorders (χ2 = 2.15, d.f. = 2; NS).
Discussion
Applicability of IHS criteria to CDH types
Our findings supported the overall fitting of IHS criteria to CDH with onset in children and adolescents. However, according to Hershey's findings (17), about 20% did not fulfil diagnostic criteria, even considering 3 months as the shortest period for monitoring the frequency of the crises. In most cases (72%), the reason why CDH could not be classified was the presence of migrainous characteristics of the crises; in the other cases, the occurrence of different types and symptoms of crises in the brief period did not allow the fulfilling of IHS criteria. This category of CDH needs further investigation to clarify the probable occurrence of age-related features of symptoms in child or adolescent CDH.
CDH presents differences both in symptomatic features and in the time trend. The migrainous symptoms may represent the ‘marker’ for another diagnostic category of CDH in children and adolescents, supporting the proposal for a single CDH syndrome (20). The clinical characteristics of CTTH are satisfactorily fulfilled by IHS criteria according to other findings (18), even if the current criterion of 6 months of daily crises (21) should be reduced to 3 months at least. The co-occurrence (‘co-morbid pattern’) of (episodic or chronic) tension-type headache and migraine without aura crises has already been highlighted (15) and is satisfied by the current system of classification (21).
However, the temporal pattern of CDH crises is also an issue that should be discussed and possibly covered in the diagnosis.
On one hand, there is the timing of onset of daily crises (‘de novo’ or ‘transformed’ CDH). On the other hand, each headache attack may present a different timing in duration (frequent, daily intermittent and daily continuous headache) (17) and differences in length (from minutes to many days). A system of classification should recognize and allow a distinction to be made between the clinical characteristics and the temporal trend. The new system of classification of headache disorders (42) provides new diagnostic categories for CDH, as chronic migraine, probable chronic migraine and new daily persistent headache. The present study has been realized according to the previous classification (21). New-onset CDH seems more prevalent in children and adolescents than ‘transformed’ or ‘chronic migraine’ (more prevalent in adults), even if further studies are needed to verify it according to the new system of classification.
Analysing psychiatric co-morbidity in CDH patients
The occurrence of psychiatric disorders in CDH patients has been widely evidenced (21–23). CDH is characterized by the highest amount of psychiatric co-morbidity compared with other headache subtypes (6). The meaning in terms of aetiology, diagnosis and prognosis needs to be clarified. Sleep disorders are the class of disorder with the highest occurrence, followed by anxiety and mood disorders. Whether such disorders represent a causative factor of CDH or are the result of a common biological pathway is a matter of debate (43).
The exact role of these factors should be more carefully analysed, even though there is a strong possibility that use of a clinical sample influences these findings. However, any therapeutic intervention should consider the co-occurrence of psychiatric disorders and take them into account. Stress should be laid on the importance of psychological assessment in the management of CDH.
Compared with other studies, we found the highest amount of psychiatric disorders in the CDH sample. On the one hand, this could be explained by the different methods of psychological assessment and clinical diagnosis. On the other hand, the presence of sleep disorders (the most frequently represented in our sample) may explain such differences. The decision to include sleep disorders as a diagnostic category was taken because they are coded by DSM IV (40), even if sleep disorders may represent a cross-diagnostic parameter for other psychiatric diagnoses (e.g. anxiety and mood disorders) and the impact on patients’ life may be qualitatively different compared with other psychopathologies. The co-morbidity with headache has been widely evidenced (43–47), even if no epidemiological studies exist on their co-morbidity. At least four potential explanations have been advanced (47): headache may cause sleep disturbance; sleep disturbances may cause headache; headache and sleep may be secondary to a third condition; headache and sleep may occur coincidentally.
Analysing the trend of CDH according to the presence of psychiatric disorders in a 4-year follow-up
It is noteworthy that CDH is difficult to treat, with 71% of patients presenting persistent headache, even if they no longer had almost daily attacks. The frequency of headache attacks is the most likely to be reduced, and better explains the overall improvement (56.3%). Just one patient had an improvement in the intensity of the crises.
Compared with other headache subtypes (27), patients with CDH have a lower chance of becoming headache free. The presence of psychiatric disorders reduced the chance of improvement of headache, as the persistence of headache was related to the increasing number of co-morbid psychiatric disorders. The negative prognostic implication of psychiatric co-morbidity in headache sufferers has been demonstrated by other outcome studies (27–29), but, to the best of our knowledge, this is the first study to highlight it in very young CDH sufferers.
This study is not focused on the natural history of CDH with onset in the young, as specialized interventions have been planned and realized for 4 years.
Concerning non-drug therapy, a plan of psychological intervention has been suggested to parents and patients, according to the weight of psychiatric co-morbidity. Patients with no or single psychiatric disorders had suggestions for controlling trigger factors. Brief psychotherapy (41) had been suggested to the patients with multiple psychiatric diagnoses, but no one of the patients completed the psychotherapy.
Analysing the presence of analgesic overuse
It is noteworthy that just one patient (with CTTH) was found to have overused analgesics at first visit. This finding was unexpected. Hershey et al. (17) found 38.5% of CDH patients overusing analgesics, Abu-Arefeh 4.3% (18) and Koenig et al. 44% (20).
This finding stresses cultural-related factors in influencing the use of analgesic drugs. On the other hand, it opens the field to hypotheses other than drug overuse to explain the chronicization of headache. In adults, the abuse of drug medication has been considered one of the main causes of CDH (30–32). In children and adolescents, other factors need to be taken into account, and the occurrence of co-morbid disorders should be carefully assessed in clinical practice. However, we need further study to address the role of analgesic overuse in children and adolescents, on the basis of shared criteria in diagnosis.
During paediatric age, the culture of correct drug intake assumes preventive significance. From childhood, the prevention of drug overuse should be pursued as part of general management, alerting parents and, wherever possible, patients.
Conclusions
CDH represents a frequently recognized problem in tertiary headache centres, both in adults and children or adolescents. This study represents an effort toward a better understanding of questions related to classification, therapy and prognosis of CDH with onset in children and adolescents. We stress the importance of further studies on classification issues of CDH, with specific attention on the youngest age. On one hand, CDH of children and adolescents has different characteristics from that of adults, and a system of classification should take into account age-related symptoms. On the other hand, the study of CDH of the youngest may bring new insight to the understanding of adult CDH. An example is the different burden of analgesic overuse, not involved in the chronicization of headache of young patients. From childhood, it is noteworthy to stress the weight of psychiatric co-morbidity in CDH patients. Diagnostic and (negative) prognostic meanings need to be outlined in order to find the best therapeutic option.