
Abstract
The primary aim of this study was to estimate the prevalence of cold-induced headache and to test if it is associated with migraine. Women attending a population-based mammography screening programme were asked to participate in the study. Fifty-one of 669 women (7.6%) experienced a headache after ingesting 150 ml of ice-cold water through a straw. Women who had experienced one or more migraine attacks in the last year (active migraine) were twice as likely to experience a headache from ingesting the cold water as women who had never suffered from migraine. Ninety-five women who had experienced their most recent migraine attack more than 1 year ago (inactive migraine) were not at increased risk. The prevalence of active and inactive migraine was 19.4 and 14.2%, respectively. Headache caused by drinking cold water is common in women. The results indicate that active migraine facilitates the perception of forehead pain induced by a cold palatal stimulus.
Introduction
Ice cream headache is a well-known headache entity that is recognized by the International Headache Society (1) as cold-stimulus headache due to ingestion of a cold stimulus. A cold stimulus placed against the roof of the mouth produces head pain in susceptible persons. The pain is of short duration, from a few seconds to a few minutes, and it is occasionally intense. It is located in the middle of the forehead, but it may be experienced on one side of the head or in the back of the head when swallowing. A cold stimulus applied to one side of the palate induces a headache on the same side (2). Ice cream headache affects people of all ages, including small children. Rarely does anyone seek medical attention because this condition is avoidable. In a population-based study (3), 15% of the participants experienced headaches due to the ingestion of cold stimuli or due to external cold stimuli such as cold weather. No gender difference was detected. Studies using more selected samples (2, 4, 5) noted a higher frequency of ice cream headache (27–93%). Age-specific prevalence rates are not available.
Migraineurs may feel an ice cream headache on the side where their migraine is located (4). Among patients referred to a hospital service because of recurrent headache, the number of migrainous symptoms was larger in patients with a history of ice cream headache than in patients without a history of ice cream headache (4). Ice cream headache (5) and cold-induced headache (3) have been associated with migraine. The pathogenetic mechanism of ice cream headache is largely unknown. It has been suggested that it may represent a vascular phenomenon (6) or a neurovascular disturbance (4). Migraine pathogenesis is believed to have components from the trigeminovascular system (7–9) and the brain (10). It has been suggested that segmental disinhibition of central pain pathways in migraine patients may be the biological basis for the proposed association between ice cream headache and migraine (11). However, in the only large experimental study (2) conducted so far, it was concluded that ice cream headache seemed not to have any special significance for migraine patients.
The aim of this study is to estimate the prevalence of cold-induced headache and to test if cold water-induced headache is associated with migraine in a non-clinical population. We took advantage of the fact that a large proportion of Swedish women aged 40–74 years attend a mammography screening unit, where they were asked to participate in this study. Little is known about factors affecting the prevalence of cold-induced headache. Middle-aged and older women undergo changes that may be relevant to primary headache disorders. Age and age-dependent factors such as educational level, menopausal status, hormonal replacement therapy (HRT), beta-blocker therapy and hypertension have been discussed in the aetiology of migraine. If CWIH and migraine are associated it is interesting to search for associations between these factors and CWIH.
Participants and methods
Participants
All women aged 40–74 years in Östhammar, a small region on the Swedish coast of the Baltic Sea, are invited at fixed intervals to a mammography breast cancer screening programme (MSP). The attendance rate at the local mammography screening unit (MUT) was estimated to be 79.1% for the first 6 months of 1998. From November 1997 to October 1998, 838 women who attended the Östhammar MUT were asked to participate in the study. Six hundred and eighty-six women agreed (81.9%). Details of the design of the present study have been published previously (12).
Methods
Prior to the cold water test (CWT) participants filled out a questionnaire which asked them about their experience with headaches caused by ingesting cold water or ice cream. In addition, the questionnaire asked them to report their intake of analgesics or anti-migraine drugs during the 3 days prior to the study and about treatment for hypertension. Participants were interviewed directly by the author, who did not know the results of the CWT at the time of the interview. The nurse who conducted the CWT was blinded to the migraine status of the participants. Data on education (five levels: elementary, comprehensive, secondary, upper secondary school, or university), natural menopause (yes vs. no), HRT (yes vs. no) (ATC codes G03C, G03D and G03F) and beta-blockers (yes vs. no) (C07A A05, C07A B02 and C07A B03) were obtained in the interview. Women in natural (non-surgical) menopause had their last periods at least 1 year prior to the study. The participants rated the pain intensity during mammography on a standard 100-mm visual analogue scale labelled ‘No pain’ on the left side and ‘Pain as intense as you can imagine’ on the right side.
In a pilot study five of 50 participants experienced head pain and no discomfort from the teeth. It was found that water ingested through a straw is very likely to flow over the palate. Participants were informed about the possibility that the cold water may induce a headache and that they were free to withdraw at any time. They were screened for dental problems.
The participants were asked to signal if they felt a sensation in the head. A nurse instructed participants to drink 150 ml of ice water (0–4°C) through a straw (length 210 mm, diameter 7 mm) placed against the roof of the mouth without pausing. The exact location of the end of the straw against the palate and the magnitude of water flow could not be controlled. Participants were sitting. After ingesting the water, the participants were asked about sensations they felt on their palate (Table 3) and in their head (Table 1). The latter were further characterized according to predetermined alternatives (Table 2). Participants experiencing pain from the test rated the intensity on a 100-mm standard visual analogue scale labelled ‘No headache’ on the left side and ‘Headache as intense as you can imagine’ on the right side. The duration and time to onset of sensations in the head were difficult to obtain and were approximated in some women. In general, characteristics of painless sensation were more difficult to obtain than the characteristics of CWIH (CWIH=painful sensations). Data on painless sensations were obtained to separate painless from painful sensations. Data on the characteristics of painless sensations were not collected from the beginning of the study because they were not expected to be very frequent.
Stratum-specific distribution of cold water-induced headache and stratum-specific odds ratios for cold water induced headache by migraine. Crude odds ratio was 2.2 (1.2–4.1)
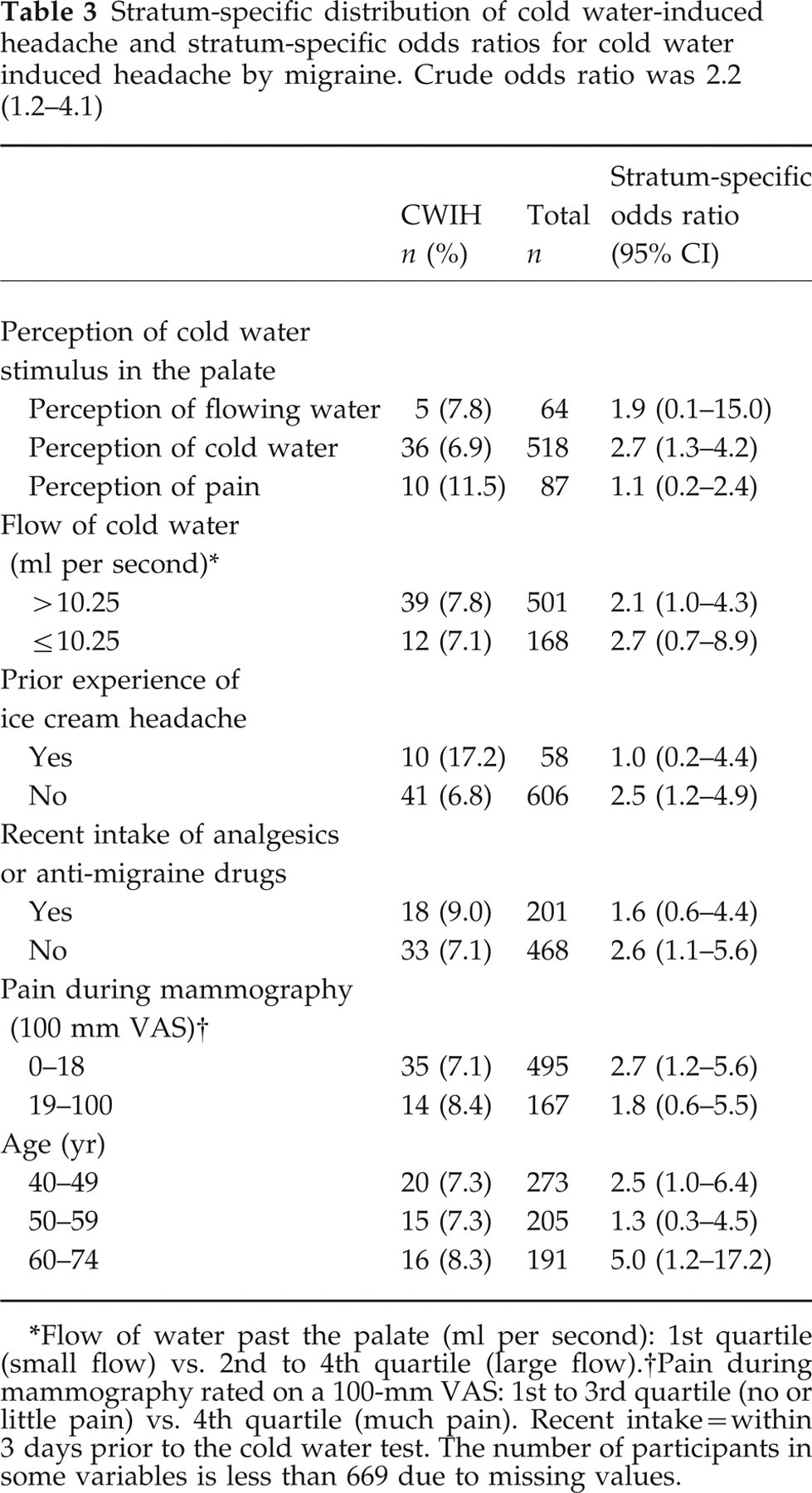
Flow of water past the palate (ml per second): 1st quartile (small flow) vs. 2nd to 4th quartile (large flow).
Pain during mammography rated on a 100-mm VAS: 1st to 3rd quartile (no or little pain) vs. 4th quartile (much pain). Recent intake=within 3 days prior to the cold water test. The number of participants in some variables is less than 669 due to missing values.
Distribution of characteristics of painless (n = 152) and painful (n = 51) sensations in the head from the cold water test

In each variable there were 14–17 missing values for painless sensations and one for painful sensations.
Results of the cold water test according to migraine status

Four women who withdrew early during the CWT and 13 participants who wore a dental plate were excluded. This left 669 women for the analysis.
Migraine in this study corresponds to migraine headache, that is migraine without aura of the IHS classification (1) or migraine with aura with a pain phase equivalent to the pain phase of migraine without aura. Active migraine headache (labelled ‘active migraine’) was defined as one or more migraine attacks in the previous year. Inactive migraine headache (labelled ‘inactive migraine’) was defined as migraine attacks experienced in the past, but not in the previous, year. The disability of the attacks in women with migraine was at least moderate (inhibiting daily activities) or severe (prohibiting daily activities). Frequency was measured in 10 predetermined categories as the number of days in the previous year during which the women experienced a migraine attack. Migraine and CWIH were the only types of headache that were studied.
Statistics
The statistical package JMP (version 3.2.2.) was used. Differences in proportions were analysed by the likelihood ratio chi-square method. Logistic regression analysis was used to regress the outcome variable CWIH on discrete and continuous variables. Confidence intervals in logistic regression were calculated via maximum likelihood estimates. The Wilcoxon–Mann–Whitney U (WMW) method was used to analyse differences in non-normally distributed continuous or ordinal data between groups. P-values less than 0.05 were considered significant. Ninety-five per cent confidence intervals were used. All tests were two-tailed.
The Ethics Committee of the Medical Faculty, University of Uppsala, approved the study (No 97 307). Informed consent was obtained from all subjects.
Results
The mean age of participants was 54 years. Sixty women (8.8%, five missing values) reported that they had experienced headache from eating ice cream or ingesting cold beverages earlier in their lives. Four women, who had unpleasant experiences from drinking cold beverages, withdrew early during the CWT. Another 13 women were excluded because they used a dental plate. None of the 17 women who were excluded had active migraine. Six hundred and sixty-nine participants were left for the analysis of the association between migraine and the outcome of the CWT. In the CWT, 51 (7.6%) and 152 (22.7%) of the 669 women (Table 1) experienced painful and painless sensations, respectively. The median time taken to drink the water was 21 s (5–157 s). The median flow of cold water intake was 7 ml/s (1–29 ml/s). Ten participants left more than 10 ml but less than 60 ml of water. The 1-year and lifetime prevalence of migraine was 19.4 and 33.6%, respectively.
Characteristics of sensations in the head
The median of the approximated time to onset of painless and painful sensations in the head was 20 s. The median of the approximated duration of painless and painful sensations was 14 and 20 s, respectively. The quality (chi-square = 23.3, 4 d.f., P < 0.0001) of sensations differed between the groups due to the large contribution to the total chi-square sum from the quality ‘unclassifiable’. The median pain rating of CWIH on the 100-mm VAS was 36 mm (6–100). There was no statistically significant difference in the location, quality or duration of the CWIH between participants with and without active migraine.
Migraine as a predictor of CWIH
One hundred and ninety-five women out of the 426 (31.4%) women without any experience of headaches from drinking cold water or eating ice cream had a history of migraine and 28 of the 60 (46.7%) women with experience of headaches from drinking cold water or eating ice cream at any time during their lives had a history of migraine (OR = 1.9, 95% CI 1.1–3.3). Active migraine was a significant predictor of CWIH (Table 1) but inactive migraine was not. Inactive migraine was therefore disregarded in further analyses; that is, women with inactive migraine were treated as if they had never had a migraine attack. The crude odds ratio for CWIH by migraine was 2.2 (1.2–4.1) and the explained variance was less than 2% (R 2 = 0.017). Stratum-specific crude odds ratios were calculated for age and some other variables related to the CWT (Table 3) that could possibly confound the association. The effect of migraine on CWIH was statistically uniform over strata within each variable. In a model taking all variables in Table 3 into account the odds ratio for the effect of migraine on CWIH was 2.4 (1.2–4.8). Because of the limited number of cases for this analysis, the variable ‘perception of cold water stimulus in the palate’ was collapsed into one class (perception of palatal pain vs. no palatal pain) and the variable ‘age’ was treated as a continuous variable. The whole model was significant (n = 657 due to missing values, 7 d.f., LR chi-square=16.1, P = 0.02).
Association of other variables with CWIH
‘Experience of cold-induced headache’ (P = 0.01) was associated with CWIH in univariable analysis. ‘Age’, ‘education’, ‘menopause’, ‘hypertension’, ‘HRT’, ‘pain during mammography’, ‘beta-blocker therapy’, or ‘perception of cold water stimulus on the palate’ (pain vs. no pain) were not associated with CWIH in univariable analyses.
Relationship between painless sensations and migraine
To analyse the importance of painless sensations in relation to migraine the P-value for migraine was compared in different statistical models. The variable ‘sensations of the CWT’ was either considered to be an ordinal outcome variable (no sensation<painless sensations<CWIH) or a nominal outcome variable (absence vs. presence of CWIH). Analysis of the crude data (Table 1) indicated that the effect of migraine on the variable ‘sensations of the CWT’ was statistically larger in ordinal logistic regression (P = 0.0013) than in nominal logistic regression (P = 0.014). However, this difference disappeared when the variables in Table 3 were taken into account (P = 0.014 for migraine in the nominal model and P = 0.038 in the ordinal model). The P-value for the variable ‘prior experience of cold-induced headache’ decreased from P = 0.02 in the nominal model to P = 0.00001 in the ordinal model.
Frequency of migraine headache attacks in relation to CWIH
Among women with migraine attacks in the last year there was no difference in the distribution of the number of days with migraine between the women who experienced and the women who did not experience CWIH. The median number of days during which women with active migraine experienced migraine in the year prior to the study was 7–9 days.
Discussion
In this study 8% of women aged 40–74 years experienced a headache from drinking a glass of cold water. This indicates that headaches caused by ingesting a cold stimulus are common among women in the general population. The most important finding was that women with active migraine were twice as likely to experience a headache in the CWT as women who never experienced migraine. Ninety-five women with inactive migraine were not at increased risk.
The author, blinded to the results of the CWT, interviewed all participants about migraine. Two nurses blinded to the migraine status conducted the CWT. A limitation of the study is that the CWT only could be moderately well standardized. Participants with prior experience of cold-induced headaches may have adjusted how they ingested water with the intention to avoid pain associated with CWIH. However, the association between migraine and CWIH was statistically significant in participants who had no experience of cold-induced headaches (n = 606, Table 3). The crude odds ratio and the odds ratio adjusted for some potential confounding factors were similar. To conclude, through the large sample size and the actions that were taken to minimize confounding, it is likely that the methods were valid with regard to the association between CWIH and migraine. This conclusion receives support from the similarity in strength of the association between cold-induced headache and migraine measured as lifetime experience (OR = 1.9) or measured within the context of the CWT (OR = 2.2). The generalizability of the results is limited to women attending an MSP, which is based on the population register of all women aged 40–74 years living in a rural district in mid-Sweden. The attendance rate of the MSP and the participation rate in the study were approximately 80%.
As expected, the CWIH had characteristics similar to ice cream headache (2). Because the position and magnitude of the water flow could not be controlled, the study was not planned to make comparisons between the characteristics of CWIH and migraine headaches. The lifetime prevalence of headache caused by ingesting a cold stimulus was 9%, comparable with cold-induced headache (15%) in Denmark (2) but lower than ice cream headache in more selected subjects (27–93%) (2, 4, 5). The significant association found in this study between previous experience of cold-induced headaches and migraine at any time during life is in line with previous findings (3, 5). Interestingly, the strength of association in this study (OR = 1.9) and in the study by Rasmussen and Olesen (3) (OR = 1.7) was almost identical. Bird et al. (2) reported that an ice cream headache was produced in a larger proportion of students than of migraineurs. The authors did not present a formal analysis of this difference. The ice cream used for the students was colder than that for the migraineurs. Differences in sociodemographic variables, in the selection of participants, and in the methods used to collect and analyse data, may explain the contradictory findings between the Bird et al. study and this study.
Smith described painless sensations from a cold palatal stimulus (6), but their high prevalence (22.7% in this study) had been not recognized previously. The data suggest that migraine does not predict painless and painful sensations better than it predicts painless sensations alone. The painless sensations resemble CWIH and may represent intermediate sensations between no pain and true pain. The data indicate that they are associated strongly with prior experience of cold-induced headache and they are much less associated with active migraine. This could mean that women with experience of cold-induced headache adjusted the way they ingested water to avoid a headache. However, if not recognized and separated from painful sensations, they may be a source of variation in studies.
This study allows some conclusions about the basic pathogenetic mechanisms of CWIH. Systematic studies of the importance of the quality and intensity of the palatal stimulus are not available. In this study women with CWIH experienced palatal pain more often than women with no CWIH, but the difference was not significant. Thus, palatal pain seems to be of no or little significance for CWIH, underlining that CWIH is not only a referred pain (palate to head) but also a transformed sensation (cold to pain), possibly favouring a central nervous mechanism before sensitization of peripheral structures.
Since active migraine but not inactive migraine predicted CWIH, the possibility remains that CWIH is related mainly to the activation process itself (facilitation or disinhibition of pain impulses or their perception). This finding raises the question of whether CWIH also may be related to primary headaches other than migraine. Two observations indicate that activation may not be temporally tied to migraine headache attacks or to the following few days after migraine headache attacks as expected from central sensitization (13). First, CWIH and migraine were associated in women (n = 468, Table 3) who did not take analgesics or drugs for the acute treatment of migraine during 3 days prior to the CWT. The variable ‘recent intake of analgesics or anti-migraine drugs’ was used as a surrogate variable for ‘the presence of migraine or any pain requiring medication in 3 days prior to the study’ and to account for the analgesic effect of such medications. Only 10 women stated that they did not treat migraine attacks pharmacologically. Secondly, among women with migraine (n = 130) there was no difference in the distribution of the number of days with migraine during the previous year between the women who experienced (n = 51) and women who did not experience (n = 79) CWIH. However, central sensitization cannot be entirely excluded, but a memory-like mechanism (14) — extending its effect over several months — appears to be a more likely explanation. Such a mechanism related to episodic or paroxysmal disorders could be kindling or an equivalent mechanism not yet identified.
A cold water-induced painful palatal sensation and pain during mammography did not predict CWIH nor did they confound the association between CWIH and migraine, indicating that generalized pain sensitivity is not a probable mechanism. Age, educational level, HRT, menopausal status, beta-blocker therapy and self-reported hypertension were not aetiological factors in CWIH.
The prevalence of CWIH and the magnitude of the crude odds ratio between CWIH and migraine was unrelated to age (Table 3), whereas the prevalence of migraine declined with age (12). Migraine exerts a significant although not very large effect on CWIH. This explains why a positive correlation cannot be expected between age-specific prevalence estimates of CWIH and migraine.
This study focuses on the prediction of CWIH by migraine. However, whether the susceptibility to headaches caused by the ingestion of cold material precedes, follows, or begins at the same time as, the susceptibility to migraine cannot be determined.
To conclude, this study provides evidence that headaches from drinking cold water are common among women and that there is a significant association between CWIH and migraine. It is suggested that the association is based on the activation of a shared pain-modulating mechanism. Future studies may focus on the basic pathophysiology of cold-induced headache and whether repetitive cold stimuli or serotoninergic drugs used for the treatment of migraine may modify the characteristics of cold-induced headache.
Footnotes
Acknowledgements
Many thanks are due to Professor PO Lundberg for advice during this study and comments on the manuscript and to Professor P Hartwig for comments on an early version of the manuscript. The author thanks Dr E Thurfjell at the Department of Diagnostic Radiology, and Gunnar Berglund and Marita Berglind at the Östhammar Mammographic Screening Unit for their kind co-operation. The author also thanks Marita Jonsson, Lille-Mor Jansson, Yvonne Björn and Ingrid Lindquist for technical assistance. The author also thanks Marie-Louise Nordström, Department of Information Science, Division of Statistics, Uppsala University, for statistical advice. This study was supported by grants from the Erik, Karin and Gösta Selanders Foundation, the Research Foundation at the Uppsala University Hospital, the Foundation for Psychiatric and Neurological Research at Uppsala University, and the Swedish Migraine Society.