
Abstract
The aim of the present study was to detect possible risk factors in migraine with aura (MA) by analysis of discordant twin-pairs. In a recent population-based twin study we established that environmental factors account for approximately 50% of the variation in liability to MA. A cohort of 5360 same-gender twin-pairs from the general population was screened for migraine. All twin-pairs with possible migraine were interviewed by a physician. A questionnaire provided information about living conditions and lifestyle. Of the 169 discordant twin-pairs 51 were monozygotic and 118 were dizygotic twin-pairs. Several putative risk factors—schooling, education, marital status, smoking status and alcohol consumption—showed no association with MA. The presence of migraine without aura or tension-type headache did not increase the risk of MA. Stress and mental tension, and bright light precipitated attacks of MA in, respectively, 44% and 28% of the twins.
Introduction
Migraine is classified as migraine with aura (MA) or migraine without aura (MO). Most migraineurs have only attacks of MA or MO, while a minority of migraineurs have co-occurrence of the two subtypes (1, 2). The relative strength of genetic and environmental factors in MA has been analysed in a recent twin study (3). The risk of MA for a monozygotic (MZ) co-twin was only 50%. Therefore, environmental factors are important. They can be divided into factors initiating onset of migraine and factors precipitating the individual attacks. Identification of the role of specific environmental factors is, however, complicated since they probably cover a wide spectrum of variables, including living conditions, exposures and psychosocial factors. Moreover, the influence of environmental factors is complicated by the fact that MA occurs in attacks and has an intermittent course throughout life (1).
The literature on environmental factors associated with MA is sparse. A Danish population-based survey found no association between migraine and social factors such as marital status, cohabitation or education, while migraine was associated with exposure to chemicals and fumes at work (4). An American survey screened for headache symptoms and socio-demographic factors and found that migraine was associated with household income, being more frequent in the lowest income group (5). No previous studies have evaluated potential risk factors for MA by the twin method. The present study analyses twin-pairs discordant for MA and the association to schooling, education, marital status, smoking status and alcohol intake. Precipitants of MA may be numerous and vary from attack to attack. The importance of some commonly reported precipitants—stress and mental tension, bright light, physical activity and alcohol—was analysed.
Subjects and methods
Sampling and variables
The New Danish Twin Register is a nationwide population-based twin register which is representative of all Danish twins born in the period 1953–82 (6). The zygosity of the twins has been established by means of a questionnaire regarding intrapair similarity. This method classifies about 95% of the twin pairs correctly (7, 8). A cohort of twin-pairs born during 1953–60 comprising 2026 MZ and 3334 dizygotic (DZ) same-gender twin-pairs was screened by questionnaire for migraine (9). A total of 87% of the twins completed the questionnaire (9). The questionnaire also included variables related to education and lifestyle. All twin-pairs where at least one of the twins had reported migraine or possible migraine had a semistructured headache interview by telephone by one of two neurological residents specially trained in headache diagnoses (V.U., M.G.). The zygosity and response to the questionnaire were blinded for the interviewers. The criteria of the International Headache Society (IHS) were used (10). The participation rate of twins in the interview by telephone was 90% (9).
The present analyses included all twin-pairs discordant for MA. A detailed description of the methods used in the study can be found elsewhere (3, 9). Table 1 shows the different variables which were analysed. Twins who were married or lived with a partner were classified as married, and twins who were living single were classified as unmarried. The twins were classified according to smoking status to evaluate the effect of smoking. Smokers were defined as currently smokers if they smoked daily or occasionally. Non-smokers were defined as individuals who never had smoked daily or occasionally, and former smokers as smokers who previously had smoked daily or occasionally. A minority reported to drink more than seven drinks of alcohol a week, and for the analyses weekly drinks of one to seven were compared with weekly drinks of more than seven drinks. The interviews of the twins included questions of different possible precipitants of attacks: stress and mental tension, bright light, physical activity and alcohol.
Variables in the structured questionnaire
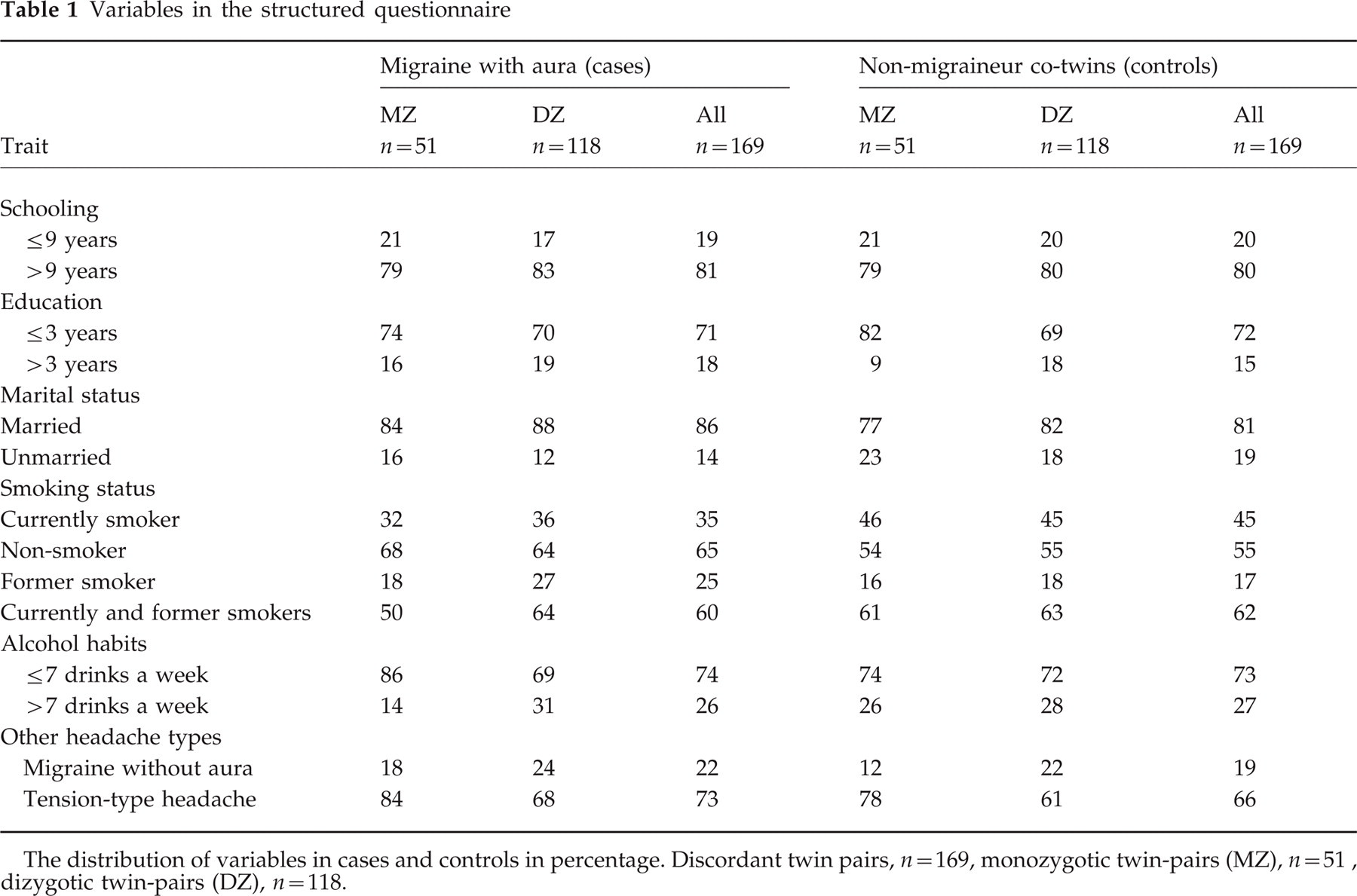
The distribution of variables in cases and controls in percentage. Discordant twin pairs, n = 169, monozygotic twin-pairs (MZ), n = 51, dizygotic twin-pairs (DZ), n = 118.
Statistical analysis
A matched case-control study was performed to evaluate the association between MA and the possible risk factors. The cases were the individuals with MA and the controls individuals who had never had MA. The cases and controls were matched optimally since they were twins, the MZ twins sharing 100% of their genes, and the DZ twins sharing on average 50% of their genes. An approximate estimate of the relative risk of a disease associated with exposure was given by the odds ratio, analysing pairs with cases and controls being discordant for the exposure (11). The significance of the odds ratio was found by means of McNemar's test (12). The 95% confidence intervals for the odds ratio were calculated using methods for confidence intervals for proportions (11). Frequencies were compared by Fisher's exact test, and means by Student's t-test. Paired sample tests were used to evaluate mean values of variables in cases and controls. The significance level was 5%.
Results
In total 169 pairs discordant for MA were identified. The distribution of zygosity was 51 MZ and 118 same-gender DZ pairs. The male to female ratio was 1:1.4. The overall lifetime prevalence of MA in the twin sample was 7.1% with a male-to-female ratio of 1:1.1 (9). The overall mean age of onset of MA in the twin sample was 21.4 years and did not depend on gender or zygosity (9). Co-occurrence of MA and MO was found in 7% of the twins (9). The variables occurred with similar percentages in cases and controls (Table 1). No significant variation was found between males and females, or between MZ and DZ twins regarding the variables. The mean values of number of cigarettes a day was similar in cases and controls, and in males and females (16.4 cigarettes vs. 15.6 cigarettes, P = 0.60, and 16.2 cigarettes vs. 14.2 cigarettes, P = 0.23, respectively). The mean age at onset of smoking was significantly lower in cases compared with controls (15.1 years vs. 16.5 years, P = 0.03), while the mean age at onset of smoking was similar in males and females (16.4 years vs. 15.6 years, P = 0.20). Three twins reported never drinking alcohol. The majority of twins reported drinking one to seven drinks a week with no significant differences regarding gender or cases and controls.
Females had a higher frequency of MO than males, although the difference was not significant (25% vs. 15%, P = 0.09), the male to female ratio being 1:1.7. The majority of the population had tension-type headache (TH), and it occurred with similar frequencies in males and females (62% vs. 75%, P = 0.30), the male to female ratio being 1:1.2.
Table 2 shows the odds ratios of MA in relation to the different variables. None of the odds ratios reached significance. There was a trend that being married vs. living single increased the risk of MA. An increasing number of weekly drinks of alcohol indicated a lower risk of MA. Analysing the odds ratios there was found to be no significant difference regarding zygosity and gender.
Putative aetiological parameters and migraine with aura analysed by odds ratios

MO, Migraine without aura; TH, tension-type headache.
Table 3 shows different precipitating factors of attacks of MA. The most frequent precipitating factors were stress and mental tension, and bright light. Only a minority reported physical activity and alcohol as precipitants. There were no significant differences of precipitating factors between MZ and DZ twins, or between males and females.
Precipitating factors (in percentage) of migraine with aura

Discussion
The New Danish Twin Register is population-based and therefore less likely to be biased by selection due to diseases compared with volunteer samples. The study population born 1953–60 was chosen in order to ensure that most participants would be past the age of onset of MA. This occurs before age 40 years in the great majority of cases (1, 13). The lifetime MA prevalence of 7.1% is similar to results of studies in non-twin populations (1, 13, 14), emphasizing that status as a twin does not affect the occurrence of MA. The high questionnaire response rate and high participation rate support the representativeness of our study population. We used matched case-control study, since twin pairs are genetically matched, MZ pairs sharing all of their genes and DZ pairs half of their genes on average, thus minimizing genetic confounding. The case-control study was matched with control of age, gender and childhood environment as potential confounders. Analysing only discordant pairs emphasized the potential influence of environmental factors. Since none of the possible risk factors analysed reached significance the odds ratios were not calculated using a logistic regression model. Odds ratios were presented for all twin-pairs since no differences were found between MZ and DZ pairs analysing the variables.
Our study is the first twin study analysing various environmental factors which may be associated with susceptibility to MA. We found no association between MA and schooling, education and marital status. This is in accordance with a Danish non-twin epidemiological survey (4). Previous twin studies have shown smoking to be a risk factor for various diseases (15, 16). However, this was not found in the present study. Being a former smoker also did not affect the risk of MA. Relatively few twins consumed more than seven drinks a week, leaving the effect of alcohol an open question. The prevalence of twins with both MA and MO was comparable with prevalences of co-occurrence of MA and MO found in other population-based studies (1, 2). Co-occurrence of MO or TH did not influence on the risk of MA, supporting the conclusion in two recent studies, that MA, MO and TH are to be regarded as separate clinical entities (14, 17). The different male to female ratios of TH, MA and MO are also supportive for the differentiation of migraine and TH. Thus, we were unable to demonstrate any effect of the risk factors we analysed on MA.
The fact that the twins were brought up together may actually eliminate the effect of environment due to equal pairwise living conditions. Adoption studies of twins reared apart are in this respect a better approach for analyses of effects of environment, but such pairs are very rare. It may be postulated that MZ twins are more likely to share intrapair environment than DZ twins. However, any potential biases due to possible intrapair variability in environment are presumably most important in studies of behavioural and psychological traits. Reports of possible precipitants of migraine attacks are numerous, although divergent conclusions have been drawn and precipitants have for the most part not been reported for MA and MO separately. The most common precipitating factor in the present study was stress and mental tension, in agreement with results of previous studies (17–20).
Risk factors may be understood by comparison of prevalences of MA in different cultures. Prevalence of migraine has been reported to be much lower in Asians than in Europeans and Americans (21, 22). The observed different prevalences may reflect variations in diagnostic criteria and constitutional factors and may not be due to different environmental factors. An American study of variation in migraine prevalence by race found that Africans and particular Asians living in the USA had lower prevalence than Caucasians (23), indicating an important role of genetic influence in MA. However, that study included only relatively few Africans and Asians compared with Caucasians, which may have skewed the results. The prevalence of MA is very similar in Europe and the USA (1, 5), where living conditions and exposures vary to a large degree. Thus, exploring the importance of environmental factors in the aetiology of MA by analyses of different cultures does not give any obvious results and may not be feasible. Research into the aetiology of MA has until now for most part focused on the genetic component. However, the influence of environmental factors in MA is equally important, not least because an identification of environmental factors could lead to non-pharmacological prevention. Although no associations could be shown between MA and environmental factors in the present study, further studies are much needed.
Footnotes
Acknowledgement
Appreciation is expressed to Professor Jaakko Kaprio (University of Helsinki, Finland) for valuable comments and advice during preparation of the manuscript.