
Abstract
Epidemiological studies have shown that 3–7% of the paediatric population suffer from migraine. Despite this high prevalence little has been published about the natural history of migraine or of its prognosis. The objectives of this study were: (i) to outline the natural history of migraine in childhood; and (ii) to identify early predictors of an unfavourable clinical evolution. A prospective, longitudinal, 10-year follow-up study was conducted of the clinical evolution of 181 paediatric patients with migraine. Data analysis was performed by statistical significance and logistic regression tests. In our study 24.3% of children with migraine had their onset before age 6 years and another 57% between 6 and 10 years of age. A positive family history of migraine was recorded in 77.5%. Eighty-eight percent of patients followed a favourable clinical course. The remaining 12% of patients had to be placed on prophylactic treatment owing to the increasing of their headache. Of all parameters investigated, the age of onset was the only statistically significant predictor of an unfavourable clinical evolution. We conclude: (i) most patients with migraine headache starting in childhood do not require prophylactic treatment; (ii) the earlier the disease begins the more likely is an unfavourable clinical course; (iii) genetic factors play an important role in the phenotypic expression of the disease; (iv) our study suggests the existence, at least, of two different populations among childhood migraine patients.
Introduction
The first description of different types of headache in children and their clinical characteristics dates from 1949 (1). Since 1962 a growing number of studies dealing specifically with childhood headache have been published (2–8) and from them it would seem that, either the incidence of cephalalgia in the paediatric age group is higher than was generally suspected or it has been progressively increasing from what was initially recorded (8). Recent studies (8–11) state that 14–25% of children experience headache episodes and that migraine involves 3–7% of the paediatric population.
Migraine is still defined and diagnosed by its clinical findings but, depending on the age of the population studied, its clinical manifestations vary. Many clinical characteristics of migraine presenting in childhood differ from that starting in adulthood. Childhood migraine tends to manifest before the age of 10 years (2, 5, 8, 12, 13), its incidence is greater in males than females < 10 years of age, but increases in females around and after the age of menarchy (2–4, 9, 12–15). Some clinical findings of childhood migraine change with time: attacks become progressively more frequent and intense in females (2, 4, 16); localization moves from bifrontal to hemicraneal (13, 14); remission periods, that can occur between 9 and 18 years, tend to be infrequent beyond 20 years of age (12, 17, 18). A positive family history of migraine is more commonly recorded in children than in adults (2, 7, 12–14, 19, 20) and, in fact, some of these families have mitochondrial diseases (21, 22) or, as in the case of familial hemiplegic migraine, the cause of the disease has been linked to chromosomes 1 and 19 (23, 24).
The clinical study of Bille (17, 18) of 73 children with migraine, followed up for > 40 years, reveals that 50% of them continued to suffer migraine crisis throughout their life. More than half of adults with migraine recall that their headache started before they were 15 years old (25), but no data are available on the pattern of evolution of migraine depending on whether the headache started before or after puberty. Finally, studies trying to define factors anticipating a severe or complicated clinical course of migraine starting in childhood are unavailable and therefore there are no clues as to which children are more likely to require prophylactic treatment.
A deeper knowledge of the presenting symptoms of migraine in childhood and, particularly, its natural history will help to delineate possible different migraine phenotypes and thus provide a better ground to decide prophylactic treatment and evaluate its effectiveness. With these purposes in mind we conducted a 10-year prospective longitudinal study involving 181 childhood migrainous patients.
Patients and methods
Since 1985, all patients suffering from headaches coming from the neurological units of the Hospital Materno-Infantil Vall d'Hebron and the Hospital de Niños de Barcelona were included in the study. All patients systematically received the same protocol of anamnesis and physical examination used in previous studies (26, 27). In this protocol they were questioned about antecedents, evolution and characteristics of the headache (frequency, duration, localization, quality, intensity and accompanying or modifying factors). The family history of migraine only included parents, grandparents or brothers and sisters. Those acceptable as having a positive family history were those relatives that complied with the criteria of the International Headache Society (IHS) (28, 29) obtained by means of direct anamnesis and those that supplied documentation of diagnosis by another doctor. For selection of paediatric patients with migraine the diagnostic criteria proposed by Prensky (30) were applied. At the beginning of the study and arbitrarily it was established that the pattern of follow up should not be less than at 3, 6 and 12 months during the first year, 6 monthly during the second year and yearly in continuation. A favourable evolution was defined in our study as migraine crisis which presented less frequently or which maintained frequency and/or intensity with respect to the previous control and these responded to symptomatic treatment. Migraine of an unfavourable evolution was considered as that which presented an increase in frequency and/or intensity of the headache and which, in the opinion of the doctor responsible for the patient, made prophylactic treatment recommendable.
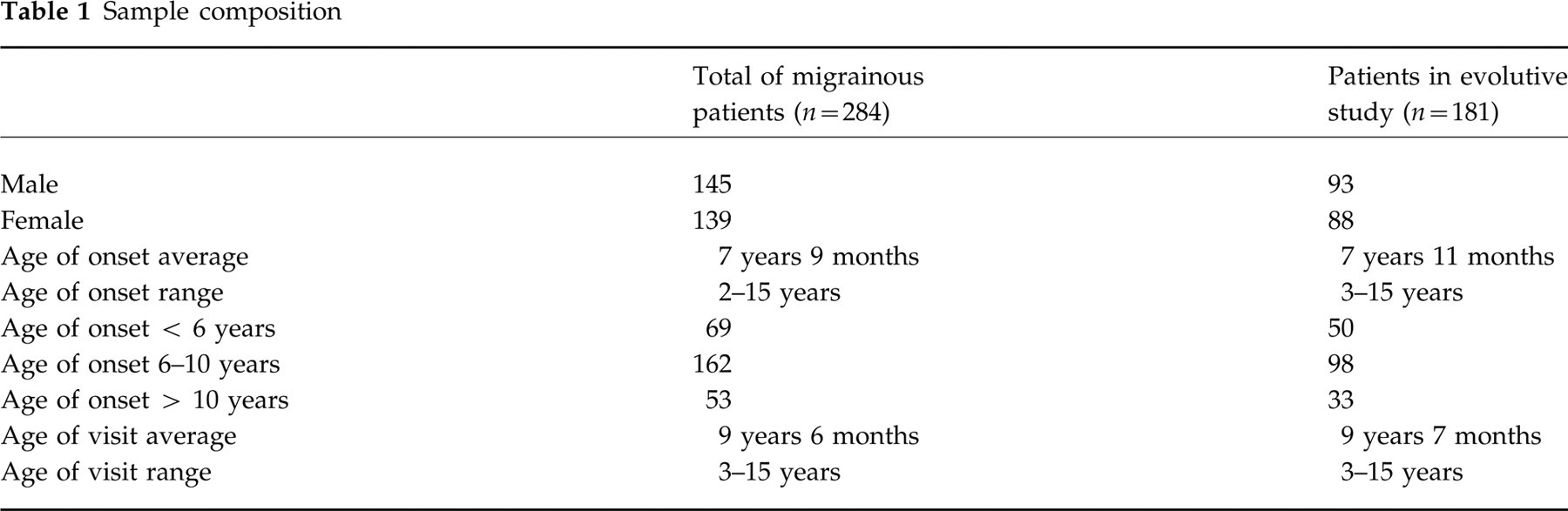
Between 1985 and 1994 a total of 717 patients with headaches was compiled, of which 284 complied with the migraine criteria proposed by Prensky (30). Of these, 103 were eliminated from the cohort dedicated to the evolutive study as they did not comply with the minimum criteria for follow up. Of the remaining 181, 21 required prophylactic treatment and from this time on they were also excluded from the evolutive study (Table 1).
Sample composition
In order to realize statistical analysis of migraine evolution during the paediatric age, all the parameters of antecedents and anamnesis obtained by application of the protocols were adapted and converted into variables, and these in turn were analysed in function of the time of evolution elapsing since the first visit. To facilitate the study, the time elapsing since the first visit was fractioned into seven periods: 1–3 months, 4–6 months, 7–12 months, 1–2 years, 2–3 years, 3–5 years and > 5 years, and the data obtained from each patient in each of the follow-up periods were taken into account during statistical analysis. All the variables included in the protocol were compared in function of sex, age of initiation and type of clinical evolution. All variables were submitted to analysis by means of the χ2 test, Student's
Results
Starting age
The starting age of the 284 patients follows a normal distribution curve (Fig. 1) with a range between 2 and 15 years, a peak between 6 and 8 years and a mean of 7 years and 9 months. The age at which the patients were referred to a child neurologist had a similar distribution, with a peak of maximum frequency between 10 and 12 years. The mean of debuting age was somewhat higher in the girls, although without statistical significance. However, the percentage of girls was significantly higher (62.3%) in the group that started their symptoms after 10 years of age.

Graph showing age of onset of symptoms and age of first visit to the Hospital. ▪, Age of onset; □, age of visit.
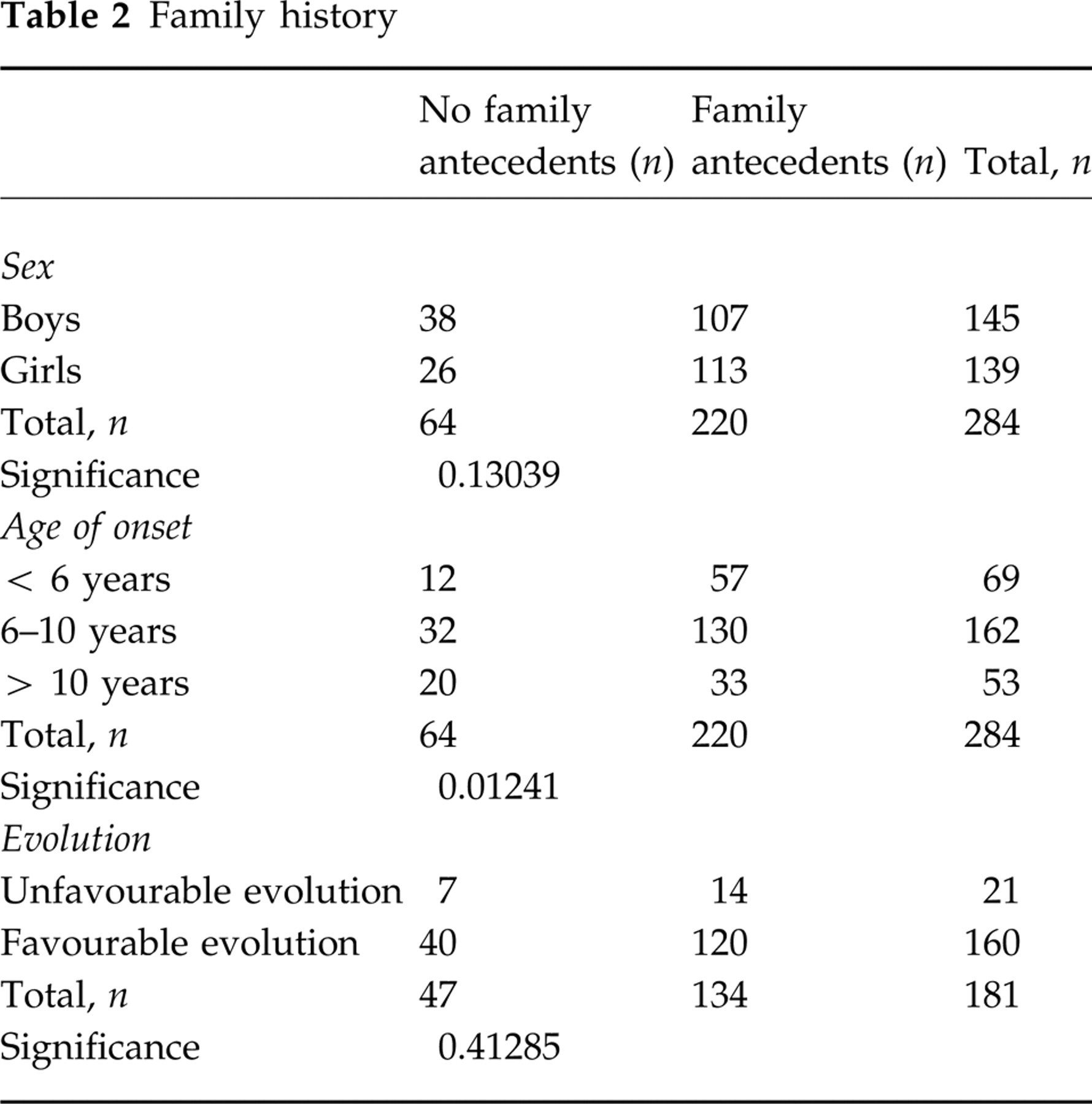
Family history
A positive family history was recorded in 77.5% of our patients. There was a significantly higher number of family members with migraine in those children whose symptoms began before 10 years of age. This finding however, does not have statistical significance when it is related to the types of migraine evolution (Table 2).
Family history
Types of migraine
As our study started before 1988, the different subgroups of migraine recognized by the IHS (29) were not recorded. Of the 284 patients of our series, 11.6% presented some type of prodromal manifestation. In more than half (58.3%) of them the headache appeared after 10 years of age. Comparison of the patients with prodromes or without them did not show significant differences concerning sex, starting age or type of evolution.
Presenting symptoms of migraine
Of the 284 migrainous patients, 116 were referred to our neurology units within the first year of the beginning of headaches, 111 between 1 and 3 years and 57 after 3 years of evolution of symptoms. For the study of the presenting symptoms of migraine the 116 patients that had less than a 1-year evolution since the beginning of symptoms were analysed. In 43.1% of these children worsening of the symptoms, perceived by either the patient or the family, was the main reason for consultation. In more than 60% of these children, the motive of consultation was that the intensity of the headache interfered with the activity being performed by the patient at the time of onset of the symptoms. Frequency of the crisis in this group of patients was weekly in 39.7%, monthly in 31.9% and only 7.7% showed asymptomatic intervals of more than 1 month between crises. It was difficult to be precise about the duration of the crises, as they were modified by pain relievers administered by the parents and/or by sleep. However, 47.4% of the patients presented durations of < 2 h, 40.5% of between 2 h and 24 h and 9.5% of > 24 h. The headaches improved with sleep or rest in 78.4% of all these patients. Psychical tension was the only triggering factor that showed significant differences when related to the starting age: in 47.1% of patients that experienced this apparent trigger, their headache started after 10 years of age.
Natural history
Of the 181 patients chosen for the evolutive study, 21 (11.7%) complied with the criteria of migraine of unfavourable evolution, and of these 17 (80.9%) required prophylactic treatment within the first 2 years of follow up. Figure 2 shows the accumulated percentages of patients with an unfavourable evolution throughout the different periods of follow up: the slope of the survival curve is levelled as from the year 2 of evolution. Although the structure and duration of the study do not allow identification of the existence of remission periods, it has been possible to identify patients free of symptoms: 41.3% of patients followed up for > 5 years have been proven to be asymptomatic for > 1 year. Analysis of the factors that motivated initiation of prophylaxis shows that: half of the patients with a headache duration of > 24 h were placed on prophylaxis. Patients with crisis that lasted ≥1 day received 2.24 times more prophylaxis than those with a duration of < 24 h; 32.4% of patients that had stress as the triggering agent or aggravating factor of the crisis received treatment.

Cumulative percentage of patients subjected to prophylactic treatment over the period of follow up.
Markers of prognosis
In order to evaluate the existence of markers of unfavourable evolution all variables obtained by the application of the protocols were compared between the populations of patients with favourable and unfavourable evolution of their migraine (Table 3). The starting age demonstrated significant differences: the proportion of patients with headache of favourable evolution was higher among those that started symptoms after 6 years of age (93.9% and 84.8%) than among those that started earlier (80%). The rest of the antecedents and clinical characteristics do not demonstrate significant differences between the two populations studied.
Anamnesis according to evolution


To isolate the variable ‘starting age’ from the possible influence of other characteristics of antecedents or anamnesis, logistic regression analysis was carried out, which again demonstrated statistical significance (Table 4). On comparison of the population that started migraine between 6 and 10 years with the group of initiation at < 6 years, a relative risk was appreciated of 0.24 for developing an unfavourable evolution: the latter group was 4.2 times more exposed to an unfavourable evolution than the former group. Patients that started their migraine after the age of 10 years had a possibility 0.65 times greater of developing an unfavourable evolution than the group with an earlier starting age, but this difference was not significant.
Relative risk of unfavourable evolution

RR, Relative risk (logistic regression);
Discussion
The starting age of symptoms referred by the relatives of the patients of our study shows an incidence peak of between 6 and 8 years, with a range oscillating between 2 and 15 years. The higher limit of the range is conditioned by the limit of the paediatric age established by our Hospitals (15–16 years). In the group of patients > 10 years of age at the initiation of symptoms the girls predominated significantly (62.3%). Interestingly enough, these results coincide with those obtained in other studies (2, 3, 7, 9, 13, 15, 30) in spite of the differences in diagnostic criteria.
The high incidence of family antecedents in migrainous patients has been used as an argument that supports the existence of genetic factors in the aetiopathogenesis of this type of headache (20, 33, 34). More than 75% of the direct relatives of our patients suffer from headaches of a migrainous form, a fact that coincides with many articles published (2, 7, 10, 12, 13, 30). In a recent study, Stewart et al. (20) found that the risk of migraine is 50% more likely in relatives of migraine probands with ‘disabling migraine’. These authors consider that previous studies have given too much importance to family factors in the migrainous population due to a lack of precision in the anamnesis and by including in the diagnostic criteria the family antecedents of migraine. The majority of the relatives of our patients were questioned directly at the time of consultation and only those that complied with the diagnostic criteria proposed by the IHS for adults were admitted (28, 29). Moreover, of the 433 patients with non-migrainous headaches controlled in our Hospitals and submitted to the same type of anamnesis, the presence of family antecedents of headache was noted in only 28%. On the other hand, the last study of Bille (18) offers new evidence about the hereditary nature of migraine, on demonstrating that at the time of the study, one-third of the children of parents with migraine followed up in the study for 40 years had presented episodes of migraine.
There are few data published in the literature that refer to the evolution or prognosis of migraine that starts in the paediatric age, and each one of them uses different concepts and different periods of follow up. Congdon & Forsythe (12) found 34% of remissions in a population of 300 children with migraine followed up between 4 and 10 years. Sillanpää (3) found 22% of remissions in 355 children with migraine followed up for 7 years if the starting age was before 8 years of age and 25% if starting age was after 14. Hinrichs & Keith (35) found improvement in almost 80% of their patients after 14 years of follow up. Of the 73 patients followed up by Bille for more than 40 years, 46% were free of symptoms and in 22% the migrainous headaches persisted, although with less frequency and/or intensity (2, 17, 18). In a recent study (36), Guidetti & Galli reviewed the 8-year evolution of 100 patients with headache (migraine and tension-type) and recorded remission in 34% and improvement in 45%.
Given the relatively short period of follow up (2–10 years) of our study, we opted for grouping patients with regard to the tolerance of their headache (migraine of favourable evolution vs. migraine of unfavourable evolution). In our population of migrainous patients 88% followed a clinical course of stability or improvement with regard to the frequency and/or the intensity of the crisis. Moreover, 41.3% of these patients followed up for > 5 years referred to asymptomatic periods for 1 year minimum. Statistical analysis of all the variables used in our study shows that an early starting age of symptoms is the only significant marker for an unfavourable prognosis (Tables 2 and 3). Children who start their headache before the age of 6 have 4.2 times more risk of an unfavourable evolution than those whose symptoms appear between 6 and 10 years of age (Table 4). Guidetti & Galli (36) found no differences in prognosis related to age onset. However, in their study they applied IHS criteria, their migrainous population was of 64 children and the evolutive data were obtained with different methods.
On the other hand, of the 21 patients of our series that presented an unfavourable evolution, this was shown during the first 2 years of follow up in 17 of them. Given that the incidence of family antecedents is significantly higher in the group of children in our study that started symptoms before the age of 6 years, it would seem reasonable to propose that the greater family/genetic load plays an important role in the earlier debut of migraine and that this consequently conditions a worse prognosis. However, this reasoning has not been supported by the statistical analysis of the data of our study (Table 2).
Nowadays there is a tendency to distinguish different types of migraine or migraine phenotypes (with aura, without aura, hemiplegic, ophthalmoplegic, etc.) and it is believed that they represent different diseases amongst migraine patients (37). Our study suggests the existence of at least two different populations amongst childhood migraine patients. The largest group suffers migrainous headaches during the paediatric age, which ceases to worry them and becomes less frequent or disappears before 18 years. We do not know whether the headache reappears later on in this group of patients. The second group, which starts symptoms before the age of 6 years and possibly with a greater incidence of family antecedents than the former, has greater possibilities of requiring prophylactic treatment during the paediatric age. More prospective studies are necessary that extend the evolution of migraine into adulthood in order to acquire a deeper knowledge of the different phenotypes of migraine that starts in the paediatric age, and their respective prognoses.
Footnotes
Acknowledgements
We thank Dr Titus Albareda for his critical evaluation of the final revision of the article. We also thank Mrs Terry Berry for her invaluable help in the preparation of the English version of the manuscript.