
Abstract
A developmental psychopathology approach suggests that stressful events may differentially affect individuals across the life span. This may be due to variations in how a potential victim integrates biological, emotional and behavioural systems and age appropriate differences in individual-context, individual–peer and individual–family interactions. Central to such an approach is the idea that effects are transactional between broad categories of events. Some theorists have emphasized environmental, contextual and familial factors and the interplay between such factors [1]; that the effects of stressful events are multidetermined [2]; and that no single pathway to a particular outcome is likely [3]. Further, individual and family characteristics and life experience may be either a protective or vulnerability factor, causation being complex rather than a simple, direct, event-outcome relationship [4]. A developmental approach has particular theoretical utility in a postdisaster environment given that no two individuals will have an exactly similar experience of a disaster or the range of potentially altered postdisaster interactions. The latter may include adversity in the social, family, school and individual domains [5].
In the context of broader child and adolescent psychopathology, the adoption of a developmental approach has been partly driven by advances in child and adolescent mental health epidemiology. Significant age-related effects, where age is a proxy for a range of more specific developmental issues such as cognitive style, language, social and peer orientation and biological change, have been demonstrated from parent report of emotional and behavioural symptoms in children. Using the Child Behaviour Checklist [6], cross-sectional studies have found elevated total symptom scores with younger children [7]. Over a 4-year longitudinal study total symptom scores decreased with increasing age [8]. This profile differs for the adolescent context. Using the Youth Self Report [9], adolescents reported an increase in total problem scores over a 2-year period from an initial assessment age of 11–16 years [10].
Age and gender-dependent effects for specific symptom clusters have also been reported. Verhulst reported increased symptoms of both depressed mood and clinical depression across the 11–15 years age range [7]. Kashani, and more recently McGee and colleagues reported the sex ratio (female:male) of depression as 1:1 prior to 12 years, 5:1 from 12–15 years, and 3:1 after age 15 [11, 12]. While depressive symptomatology is of specific interest in the current study, the prevalence of a range of mental health phenomena varies with age, for instance weight and eating concerns [13] and dissatisfaction with physical appearance [14].
Developmental approaches have not been widely used in child and adolescent posttraumatic stress disorder (PTSD) research, although developmental models for traumatic stress have been published [5]. An advance has been including variables other than exposure in causal models. Postdisaster coping behaviour [15], internal causal attribution [16], self-efficacy in the postdisaster environment [17] and perceived life threat have been investigated. The latter factor has been reported to be important in both adult [18] and child [19, 20] samples. Some reports have included multidomain analysis of the impact of traumatic events; findings in traumatized child and adolescent samples include diminished academic performance [21, 22], alterations in family functioning [23], and parent psychopathology [24]. The study of Handford and colleagues found that parent overreaction or non-competent response to a traumatic event was associated with greater child report of anxiety [25]. In the area of child abuse and neglect, Ciccheti and Toth [3] reviewed a series of ‘stage salient issues’ using a broad developmental perspective. They concluded that evidence exists for trauma-induced deficits in a diverse range of systems: affect regulation, attachment, adaptive representations of the self, and peer relationship function in maltreated children.
The effect of developmental stage and gender on the prevalence of PTSD and other post-event psychopathology remains unclear. Reports from children exposed to the effects of a dam collapse and a hurricane suggest that female children and adolescents report more PTSD following natural disasters [22, 26]. However, there is a female-male equivalence of PTSD prevalence following the experience of civil and war-related traumatic events [27–29]. If this finding is replicated, the explanation may be differential male-female trauma exposure during the event such that boys and men may be more exposed to war-related traumatic events given their role as combatants, even as young children. Against this notion, is the increased occurrence of physical and sexual assault against women during such conflicts. A hypothesis with possibly more explanatory power may be the cognitive dissonance experienced by males between their belief that they can protect family members during conflict versus the reality of random and uncontrollable violent and traumatic events. Age effects are more difficult to interpret. Published findings include no effect of age on PTSD prevalence [28, 30, 31], and conflicting reports that older children and adolescents [24, 32, 33] and younger children [34] have a higher rate of PTSD. From a theoretical perspective, causal models that incorporate concepts such as coping or attribution style would suggest at least a moderate positive relationship between such mechanisms with increasing age and life experience, hence decreased vulnerability to PTSD with increased age. The aim of our study was to investigate age- and gender-related patterns of psychopathology across the primary, junior and senior school developmental range in a large postdisaster sample of Australian children. A further aim was to investigate the relationship between disaster-related variables such as disaster exposure, evacuation experience, life threat to self and others, and depressive and PTSD psychopathology across this developmental range.
The Sutherland Bushfire Trauma Project (SBTP) was a post-bushfire disaster mental health service provision initiative in one Department of School Education administration area in response to a devastating bushfire that afflicted the state of New South Wales during 1994. Over a 5-day period 600 000 hectares of land was burnt; 185 houses were destroyed; 113 further homes were damaged; and 4 people died. In the area covered by this project, 86 houses were destroyed, one primary school was completely razed, two others were damaged and (miraculously) only one life was lost.
During the early postdisaster period anecdotal reports of children and adolescents with probable disaster-related emotional or behavioural disturbance were received by child and adolescent mental health professionals. Reports from parents, teachers and aid workers included the likely increased prevalence of sleep disturbances and nightmares, children being more fearful, especially of smoke, loud noises or around areas with visible evidence of fire damage. Some parents reported their child experienced a ‘personality change’, becoming quieter, withdrawn and anhedonic. Three cases of fire lighting were reported. One 4-year-old child with a daily ritual of drawing red flames on all accessible walls in the family home was referred. Given these reports and referrals, in the context of the usual postdisaster scenario of limited psychological resources and a perceived need for a substantial intervention, a proactive screening approach was adopted with the rationale of providing resources to individuals with the greatest need. For a more detailed discussion of the screening rationale and project implementation see an earlier paper [20].
Method
Participants
The study population consisted of all children in grades 4–12 (the latter being the final year of secondary school education), attending State school education in the designated disaster area. Schools were included in the project if: the school was destroyed (1 school) or damaged by fire; homes of children attending the school were destroyed or damaged by the fire; or large areas of blackened, fire damaged land needed to be traversed to attend school. Eleven primary schools fulfilled one or more of these criteria. Primary school size varied greatly from small cottage schools (n = 30 students) to schools with several hundred students. Two secondary schools fulfilled the inclusion criteria.
Procedure
Screening personnel were clinical or school psychologists, psychology masters students or mental health professionals from the only child and adolescent mental health team in the area. Screening was standardized, protocol directed and followed a brief training module. Self-report questionnaires were administered to students in their classroom in groups of 20–30 children. All primary school children had questions read to them to standardize for reading ability. No child was screened without signed parent consent; adolescents gave their own-signed consent. Parents of adolescents were provided project information and could exercise an opting-out veto.
Measures
The self-report battery included the Impact of Event Scale (IES), a 15-item scale with four answer fields [35]. The Revised Manifest Anxiety Scale (RMAS), a 37-item trait anxiety measure with a True/ False format [36]; and the Birleson Depression Inventory (the acronym BDS is used to avoid confusion with the Beck Depression Inventory), an 18-item questionnaire with three answer fields [37]. During a pilot phase significant numbers of younger children (generally those age 8 and 9) expressed difficulty understanding and sought clarification for two IES questions. Accordingly, these questions were removed and subjects answered an IES-13 questionnaire. A measurement of the internal consistency [38] of the IES scale for this sample of younger children indicated that this instrument was suitable for research use (Cronbach alpha = 0.86). For primary school children, parents provided disaster-related information: the child's location during the week and on the day of the bushfire; home damage; evacuation experience; residential dislocation experience; and comments by the child concerning the child's perception of threat to themselves and/or their parent (Table 1). This information was collected by self-report from secondary school children.
Characteristics of study population (n = 2379)
Statistical analysis
The continuous outcome variables were a depression index created by summing the 18 BDS questions (BDSSUM) and an emotional distress index created by summing the 13 IES questions (IESSUM). Explanatory variables analysed were relevant factors reported in the self-report and parental questionnaires. Based on our conceptualization of elevated trait anxiety as a vulnerability factor for a poor postdisaster psychological outcome, a further explanatory variable was created by summing the 37 RMAS questions (RMASSUM). The influences of various potential confounders such as sex and school attended were also investigated.
Gender was analysed as a binary covariate. Age, IESSUM, BDSSUM, and RMASSUM were analysed as continuous variables. School attended was analysed as a factored (nominal) variable. IESSUM, BDSSUM and RMASSUM were skewed with long righthand tails, and so were log e transformed prior to analysis. A constant of 3.0 was added to allow log e transformation when the value was zero.
Bivariate analysis used χ 2 tests in the case of pairs of categorical variables, two-tailed t-tests in the case of a categorical and a continuous variable, and correlation coefficients in the case of pairs of continuous variables. Generalized linear models (linear regression) [39] were used to model the effects of multiple covariates on the continuous outcomes IESSUM and BDSSUM. Both forward and backward stepwise modelling procedures were used to select a useful subset of independent predictors of an outcome of interest. Checks of goodness of fit [40] included an investigation of the need for interaction or polynomial terms, analyses of Pearson residuals, and examination of the effect of observations with high regression leverage. Definitive final models were shown to provide a valid summary of the observed data.
The regression models constructed included the following variables as initial possible explanatory covariates: age; gender; grade at school; exposure to bushfires; experience of evacuation procedure on day or week of fire; perceived threat to self; perceived threat to parent(s); separation of child from parents; damage to home; destruction of home; and RMASSUM. The BDSSUM index was included as an initial possible explanatory covariate in the model of IESSUM as the outcome and vice versa. To investigate any school-specific clustering effects in the data, further models were constructed for each outcome using Generalized Estimating Equations (GEEs) [41] to adjust for any correlations due to school attended. Minitab for Windows v12 (Minitab Inc., State College, PA), SPlus v4.5 (Mathsoft Inc., Cambridge, MA) and Stata v5.0 (STATA Corp, College Station, TX) were used to manipulate and analyse data. Statistical significance was defined at the standard 5% level.
Results
The study population comprised 2379 primary and secondary school students, aged from 8 to 19 (mean = 13.43 years, SD = 2.49 years). The majority of the children (n = 1449, 60.90%) were in secondary school. The children were distributed evenly among grades 4–12 (between 183 and 329 children in each grade). The gender ratio was balanced (47.77% male). Participation rates, 76% for primary and 97% for secondary school students reflect the different primary–secondary school consent procedure. As well as non-participating, parents of primary school students often cited being ‘out of the area’ during the fires and therefore the project did not ‘apply’ to them.
Participants lived in an area where 81% of residents were Australian born and where only 0.03% were Australian Aboriginal or Torres Strait Islanders. Residents who were not born in Australia emigrated from an English speaking country (8.8%), a non-English speaking European country (3.3%) or Asia (1.7%). The median annual household income was $AUD 40 000–50 000 and 46% of adult residents had obtained some post-school qualification, consistent with this area being considered ‘middle class’ in the Australian socioeconomic context. There were relatively few single parent households (10.4%) [42].
Postdisaster posttraumatic stress and depressive symptoms
Multivariate modelling suggested that the IESSUM emotional distress index, the total anxiety score (RMASSUM), grade at school, experience of evacuation during the week of the fires, and experience of evacuation on the day of fires to either a refuge or to friends/relatives significantly predicted the BDSSUM index independently of the other possible covariates (see Table 2). Gender did not significantly predict the BDSSUM index. However, evidence of a significant interaction between sex and grade at school was found (not shown in Table 2; β = −0.011, SD = 0.005, p = 0.03), this suggested that BDSSUM levels were systematically lower across all school grades in males than in females. Symptom scores for anxiety and emotional distress demonstrated a non-linear relationship with symptom scores for depression (see Table 2). Higher symptom scores for anxiety and emotional distress were associated with increased symptom scores for depression. Class at school, a variable likely to reflect both chronological age and developmental maturity, also demonstrated a non-linear relationship with symptom scores for depression (see Table 2). Adjusted symptom scores were highest in the lower and higher grades, and lowest in the middle grades (i.e. grades 8–10). Experience of evacuation on the day of fires to either a refuge or to friends/relatives was also associated with increased symptom scores for depression. Experience of evacuation during the week of the fires was associated with decreased symptom scores for depression.
Multivariate associations of BDSSUM and IESSUM scores with explanatory covariates. Results of generalized linear modelling (final models)
Multivariate modelling suggested that symptom scores for depression (BDSSUM index), perceived threat of death to self, perceived threat of death to parents, grade at school, and experience of evacuation during the week of the fires significantly predicted the IESSUM index independently of the other possible covariates (see Table 2). Gender did not significantly predict the IESSUM index. Symptom scores for depression (BDSSUM) demonstrated a non-linear relationship with symptoms of emotional distress (see Table 2); increased symptom scores for depression were associated with increased symptoms of emotional distress. Class at school also demonstrated a non-linear relationship with symptom scores for emotional distress (see Table 2, Fig. 1). Adjusted symptom scores were lowest in the lower and higher grades and highest in the middle grades (i.e. grades 7–9) (Fig. 1). The experience of evacuation during the week of the fires and the presence of a perceived direct threat to the life of either the parent or to self were also both associated with increased symptom scores for emotional distress.
Modelled relationship of emotional distress symptom score (IESSUM) to class at school.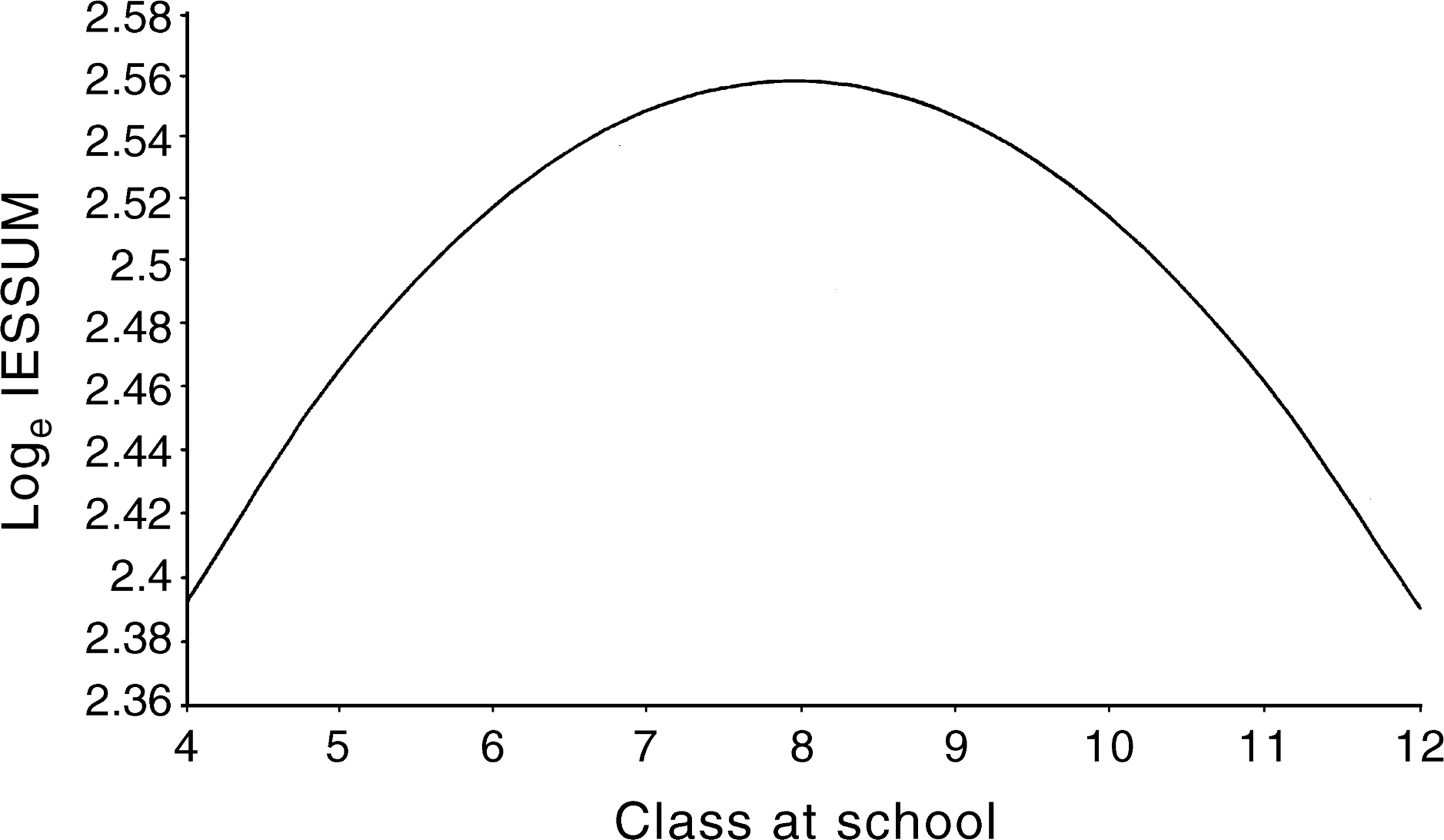
All reported associations of response variables with explanatory covariates were independent of the other possible covariates. Extended modelling using GEEs indicated no substantial clustering effects by school for either of the outcomes investigated (data not shown). The results of the bivariate analyses are not presented, but were consistent with the results of the more informative multivariate analyses.
Discussion
This study investigated a large sample of school students, across grades 4–12, who completed a self-report battery following a bushfire disaster. We found that the number of postdisaster depressive symptoms was significantly associated with an individual's higher trait anxiety, earlier school grade (although depressive symptoms rise again after grade 10), evacuation experience and emotional distress score. When depressive symptoms were stratified by age, there was a greater age-dependent effect in females than in males. In our predictive models, school grade was a more significant covariate than the child's age. This is consistent with our experience that school grade is a better approximation of an individual's developmental level than age.
Students in grades 8–10 (approximate age range 13–15 years) had the lowest depression scores. Depression scores increase in grades 11 and 12, consistent with epidemiological studies that report increasing rates of depression and depressive symptoms in older adolescents. A previous paper [20] reported the level of depression in primary school students in this postdisaster sample was similar to report rates cited in recent reviews of childhood depression [43, 44]. In this more extensive sample the greater self-report of depressive symptoms was in younger children (grades 4–6, age range 9–11 years) rather than adolescents. Our findings of the relatively elevated child depression scores and the independent relationship between depression scores and emotional distress and disaster variables such as evacuation experience are consistent with the hypothesis that younger children are more vulnerable to postdisaster depressive symptoms. Pynoos and colleagues postulated several mechanisms to explain the PTSD-depression co-occurrence: secondary depression due to persistent PTSD symptoms; chronic PSTD effecting family resources; and behavioural concomitants of PTSD causing secondary adversity [5].
Our cross-sectional methodology was unable to differentiate persistent primary versus secondary depression. However, there are several possible explanations for our findings. It is possible that depressive symptoms are inherent to the postdisaster emotional response of younger children, or that perceived loss (actual loss of life, housing and possessions was not extreme in this disaster) is a more powerful aetiological factor for depressive symptoms in the younger age group. Alternatively, there may be a strong postdisaster relationship in younger children between the prevalence of exposure to causal factors for both depression and emotional distress, (e.g. co-occurrence of experience of loss and fire exposure). Further research is required to address these questions.
Symptoms of emotional distress were significantly associated with damage to home, the individual's perceived threat to themselves and threat to their parents, earlier school grade and depressive symptom score. These findings are consistent with earlier work relating perceived threat to self to greater emotional distress [18–20] and extend such findings by reporting the potentially traumogenic effect of the child's perception that their parent may die during a natural disaster. In this postdisaster sample, the reports of Green et al. [26] and Shannon et al. [22] citing a female preponderance of emotional distress symptoms was not replicated.
A complex, non-linear relationship between emotional distress symptoms and school grade was found. Children in middle grades (7–9) reported the most emotional distress symptoms. Older adolescents and younger children reported fewer symptoms. The finding in adolescents was possibly due to a greater ability to adapt on the part of these older children, both to the disaster and to the postdisaster environments. Better adaptation with age may reflect the utilization of cognitive responses such as mature defensive styles, external attribution and internal locus of control. This group may also demonstrate greater ability to articulate distress and therefore receive both nurture and assistance in reprocessing disaster related cognitions and feeling states.
The finding of fewer emotional distress symptoms in younger children (grades 4–6) is counterintuitive to the organizational perspective equation of greater distress scores with less sophisticated adaptation. The explanation in this sample does not appear to be instrument reliability or measurement error problem. Furthermore, the two most problematic questions were removed from the battery during the pilot phase. Possible explanations may involve transactional factors not measured in this research. Such factors may include: protection from emotional distress by greater parent proximity to younger children during a disaster; differential levels of parent distress across parental age and changes in the individuals coping; and other protective and vulnerability factors across the child and adolescent developmental span.
Inherent limitations in our research stem from its service provision focus. Given the lack of research resources and links with academic mental health, many complex constructs, such as bushfire exposure, were treated as simple binary variables. Future research should ‘unpackage’ such phenomena. Including more complex constructs such as children's coping and parent emotional responses would allow more complex modelling of developmental hypotheses. The large sample size of this project and high participation rates, especially of adolescents, suggests integrated service provision and research is possible in the postdisaster environment.
Conclusion
Research in a postdisaster environment with school students across a wide developmental range found evidence of depressive and emotional distress symptoms in this group. Significant independent associations were found between total depression and emotional distress scores. Both symptom groups were also independently associated with event-related variables and exhibited complex, non-linear relationships with the child's school grade. Younger children were at specific risk of depressive symptoms in the postdisaster environment. Children in the ‘middle’ school years were at greatest risk for posttraumatic stress symptoms. This study suggests that important developmental differences in postdisaster psychological responses exist across a broad spectrum of developmental stages in children. Our results further imply that these differences need to be addressed in the context of mental health interventions in the postdisaster environment.
Footnotes
Acknowledgements
We thank Janet Cross and the school psychologists in the Sutherland Shire of New South Wales and the school principals and school authorities with responsibility in this area. Professor Einfeld gave valuable advice on research design.