
Abstract
The provision of better services and care to people who suffer from mental disorders requires: (i) developments in understanding the sciences informing psychiatry; (ii) a well-trained and caring workforce who actively seek to improve their knowledge, skills and attitudes; and (iii) a social and political commitment to caring for people with mental disorders through adequate funding and changes in social attitude. All three elements are essential if we are to reduce the burden that mental illness imposes on our communities and the individuals who make up our communities. However, without a strong science and evidence base for the practice of psychiatry, it is unlikely that a motivated and welltrained workforce will exist, and it is unlikely that there will be a social and political commitment to improving the lives of people with mental disorders. Often advances in the understanding or treatment of mental disorders have been at the forefront of changing attitudes. This paper presents a personal history of the development, ideas and practices of one clinical research unit that hopes to make a contribution to the global science of psychiatry. The history of any research unit is inevitably intertwined with the personal histories of key individuals, of opportunities taken, decisions made and local politics satisfied. Thus, no two research groups will have the same histories; however, many of the issues faced by different research units will be similar.
The environment
Christchurch is the largest city (population approximately 350 000) in the South Island of New Zealand. The population is mainly of European ancestry, but the indigenous Maori people, Pacific Islanders and a growing Asian influence contribute to the city's diversity. Christchurch hosts three universities: Canterbury University, Lincoln University (initially an Agricultural College) and Otago University – which hosts the Christchurch School of Medicine and Health Sciences. Christchurch's most famous scholars include Lord Ernest Rutherford who won a Nobel Prize for his research on the structure of the atom, and the philosopher Sir Karl Popper who lectured at Canterbury University during World War II.
The Christchurch School of Medicine was established as a clinical school of the University of Otago Medical School in the early 1970s, with the first clinical medical students coming in 1973. Professor Ken Adam was appointed as the Foundation Professor of Psychological Medicine in Christchurch. He established the Crisis Team (later renamed the Psychiatric Emergency Service) and initiated research on attempted suicide [1, 2]. However, the 1970s were difficult years for psychiatry. Christchurch, like the rest of New Zealand, was desperately short of psychiatrists. The few New Zealand medical students who were interested in psychiatry usually went to Australia, England, Canada or the United States for their training, and seldom returned to practise in New Zealand.
Within the Christchurch School of Medicine, research was growing. There were particular strengths in the Department of Medicine, where professors Beaven, Espiner, Donald and Nicholls were leading research into endocrinology. In the Department of Pathology, there were particular strengths in clinical biochemistry (Professor Carrell), immunology (Professor McGiven) and cancer cytogenetics (Dr Fitzgerald). As a medical student, I was fortunate to spend three summer holidays as a research student with Professor Carrell, studying α −1-antitrypsin polymorphisms. Professor Carrell had developed the Department of Clinical Biochemistry from a service department into an active research department. Although he was disappointed when I chose psychiatry as a career, he had shown us the possibilities of developing a research culture and environment where none had previously existed.
In Mental Health Services of the 1970s, Dr Edwin Hall was making substantial progress in modernizing the old asylum, Sunnyside Hospital, and Dr John Dobson was fighting the battles to establish psychiatry as a medical discipline in the general hospitals. By the end of the 1970s (I commenced as a psychiatric registrar in December 1979), Professor Adam had returned to Canada. The shortage of psychiatrists remained a major problem, and there was no psychiatric research. Although there may have been no research, Christchurch was fortunate to have two exceptional older psychiatrists who were vital mentors to many of us who trained during the 1980s. Dr Arthur Jones, who had come from South Africa, knew about benzodiazepine dependence before the academic or pharmaceutical worlds acknowledged its existence [3]; he knew that many patients with a diagnosis of schizophrenia improved dramatically when treated with lithium; he knew many patients with recurrent major depression required lifelong maintenance antidepressants. Given that in the early 1980s there was no evidence for maintenance antidepressant treatment for recurrent depression, it is interesting to ponder on what evidence-based zealots of the 1980s would have made of his practice, especially given the later overwhelming evidence from the 1990s for maintenance antidepressant treatment. Before it was fashionable, he spent considerable time helping family members survive severe mental illness in relatives. In the late 1980s he introduced clozapine to Christchurch psychiatry before the major American publications heralded its benefits in refractory schizophrenia. The other key mentor was Dr Jim Walshe, a former English teacher and general practitioner. In his role in liaison psychiatry, he established psychiatry's credibility in the eyes of medical colleagues. He understood the intricacies of human behaviour, including normal and abnormal illness behaviour [4, 5]. He appreciated the varieties of presentations of depressive disorders, and was well versed in their psychological and pharmacological management. Both men were highly respected by patients and colleagues; both were excellent clinicians, widely read, observant, inquiring and sceptical; and both were supportive of research initiatives.
The research instinct
Research does not happen because a committee thinks it would be a good idea. Research happens because individuals have a passion to enquire about and understand the world in which we live. During school days my first passion was cricket, but the second was chemistry. In high school I daydreamed about the chemistry of brain function; little did I realize how much progress would be made in my lifetime. Thus, I went to university with a view to studying either chemistry (the research wish) or chemical engineering (the pragmatic self). However, during my second year at university came a decision to study medicine. I thus changed from completing a chemistry degree to a biochemistry degree. In biochemistry I was inspired by Dr Darryle Reanney to explore the intricacies of molecular biology, and even after I finished my biochemistry degree we continued to have many discussions about evolutionary biology, molecular evolution, the origins of life and the philosophy of life. It is thus a source of pleasure to see growing attempts to place psychiatry within the realm of evolutionary biology [6, 7].
Unlike most fellow medical students whose motivations to study medicine were usually more altruistic, I saw a medical degree as a pathway to research. Perhaps these motivations plus the stimulating years in biochemistry contributed to the conviction that much of the preclinical medical curriculum was boring, especially anatomy, where some lecturers had no understanding of modern cell biology. However, despite my motives for undertaking research, I discovered great enjoyment in listening to patients. The decision to do psychiatry crystallized one morning for me as a fifth year medical student, after I had spent over two hours listening to the life story of a man with severe rheumatoid arthritis. Combine enjoyment of listening to patients with interests from molecular biology, evolution, neurochemistry and philosophy, and then psychiatry had no competitors as a career option.
Research is an endless quest for understanding or, in the words of Karl Popper [8], ‘The wrong view of science betrays itself in the craving to be right; for it is not his possession of knowledge, of irrefutable truth, that makes the man of science, but his persistent and recklessly critical quest for the truth’. For progress to be made, it is important that conjecture (hypothesis) and refutation are in a dynamic balance. In psychiatry's intellectual history, there have been times and places where hypotheses without attempts at refutation have been uncritically and gullibly accepted (and often to the detriment of patient care). Similarly, there have been times and places when hypothesis was absent and excessive refutation led to pessimism, nihilism and despair.
The beginnings
In the early 1980s, during my first years as a psychiatric registrar, and with encouragement from doctors Jones and Walshe, it was feasible to undertake some ‘low cost’ research in liaison psychiatry [5] and on bipolar affective disorder [9, 10]. Also, during those first three years an interest in affective disorders crystallized; a research mentor was found in Professor Donald (endocrinology) and a first research grant was submitted to the Canterbury Medical Research Foundation to study neuroendocrine dysfunction in depression. During 1983, as a fourth-year psychiatric registrar, I worked in a general hospital outpatient department and saw many outpatients with depression, a few of whom were recruited into our neuroendocrine studies [11].
This experience contributed to my view that for many clinical research studies a separate clinical research service is required. First, most outpatients seen were not eligible for the study, but still required assessment and treatment. Second, other staff, while generally supportive, seldom gave it a quite high enough priority in their busy clinical days to ‘remember’ to assist with recruitment or help in other ways. Third, colleagues sometimes think that a depressed patient with five comorbid medical disorders and refractory to a cocktail of medications would be an ‘interesting’ research subject, even though the research protocol excludes them for a variety of reasons.
A lasting memory from these early studies, in which we gave methylphenidate to both control subjects and depressed patients, were the marked individual differences in response. Later, I became aware that Eysenck's initial biological model of personality was based on individual differences in response to stimulant and sedative drugs. However, seeing these differences strongly influenced my clinical belief that, when patients report unusual effects from drugs, they require close evaluation. These observed individual differences perhaps also influenced directions for later research into the nature of individual differences (i.e. personality).
Another lasting benefit of that first neuroendocrine research project was that the grant employed a psychiatric nurse, Robyn Abbott. She has continued to be a core member of a growing clinical research group over the past 18 years. She continues to affirm, and remind others, that first we are providing clinical care for patients and only second are we undertaking clinical research.
In the fifth and final year of psychiatric training I moved to a busy acute inpatient ward in the psychiatric hospital (Sunnyside). This decreased the feasibility of constantly finding new depressed outpatients, and so research became focused on using patients with rapidcycling bipolar disorder as their own controls and for assessing neuroendocrine changes with mood changes [12]. This clinical position continued after my completion of the college exam process and also when I was initially appointed to the university department as a lecturer.
An epidemiologic interlude
During 1984, Dr Mark Oakley-Browne, a psychiatric registrar who had started his training two years after me, approached me about the feasibility of his also being involved with research on depression. We contemplated a treatment trial with both antidepressant medication and psychotherapy, but realized we did not have the resources for such a study. Instead we started thinking about risk factors for depression. We contacted Professor Andrew Hornblow (now Dean), a clinical psychologist by training, but then Head of the Department of Public Health and General Practice. Very soon a team of five investigators, including Dr Elisabeth Wells (biostatistician) and John Bushnell (clinical psychologist), were engaged in planning the Christchurch Psychiatric Epidemiology Study (CPES) [13].
While the statistics associated with epidemiology can appear overwhelming the principles of epidemiology, involving cases, risk factors and populations, are relatively straightforward. However, an epidemiologic perspective on mental illness is extremely helpful. Indeed, many clinical studies and trials could benefit if investigators were mindful of epidemiological principles. For instance, the pharmaceutical industry's desire to exclude patients with comorbid disorders from clinical trials is but one example where a little epidemiologic knowledge would be beneficial.
One outcome of undertaking the CPES was that we then became one of the sites in the Cross-National Collaborative Group under the leadership of Dr Myrna Weissman [14]. Another lasting benefit of the epidemiologic study was that two of the interviewers employed stayed with the department. Alison Pickering continued as a research interviewer across a range of studies, and as a trainer of other interviewers, up until her untimely death. Isobel Stevens was not only an interviewer with the CPES, but also became involved in data checking, cleaning and management. Isobel has continued to develop these roles and over the years has been invaluable as a study coordinator and data manager. Any large clinical or epidemiologic study requires a coordinator and data manager; a forceful lesson for researchers is never leave coordination to busy clinical staff if protocols are to be closely followed and data correctly entered.
Reflection
At the end of 1986 the position of Chair of Psychiatry in the Christchurch school of medicine was advertised. As the previous incumbent (from overseas) had not fulfilled expectations and the department still had only a minimalist research history, the appointments committee decided to appoint a young local with potential, rather than again import an applicant with a longer track record. Given the state of research in the department at that time, it was believed that things could only get better.
It was strongly suggested to me that I should take three months’ research and study leave and reflect upon future directions (indeed, it was a question mark raised about my appointment that I had not spent time ‘overseas’). With my wife and two young daughters we went to Cambridge (England) for three months in 1987 and were kindly hosted by Professor Paykel (an ex-New Zealander). I used the time to write a review on predictors of antidepressant response [15], prepare a grant application for the Health Research Council, reflect on Kendell's writings on clinical validity [16], re-read some of the writings of van Praag [17, 18] and digest Cloninger's developing psychobiological model of personality [19–21].
A first clinical research unit
The first wish in thinking about a clinical research unit (CRU) was to develop this on an inpatient basis. However, health funding and local politics deemed that this was not to be, and instead we commenced an outpatient CRU, based in the psychiatric hospital. In retrospect this has been to our advantage, as inpatient research units have always been expensive and demand constant justification. Another issue was the name: should it be called an affective disorders unit or a clinical research unit? The decision in favour of CRU was that it potentially allowed for more flexibility in the nature of the studies undertaken, and it also signalled that we were not establishing a tertiary referral service for patients with treatment resistant affective disorders. Given our interest in predictors of treatment response, we needed some patients who improved and some that inevitably did not. It is interesting to reflect on why it has been so difficult to identify predictors of antidepressant response. Part of the difficulty relates to the complexity of the apparently simple question. In a hypothetical antidepressant trial (see Fig. 1) of a noradrenergic antidepressant (NA – AD), a serotonergic antidepressant (5HT – AD) and placebo (PL) it is possible to obtain a 20% response to placebo and a 60% response to both active antidepressants.
A simplified diagramatic presentation of responders to placebo, a noradrenergic (NA-AD) antidepressant and a serotonergic (5HT-AD) antidepressant in a hypothetical depression treatment study.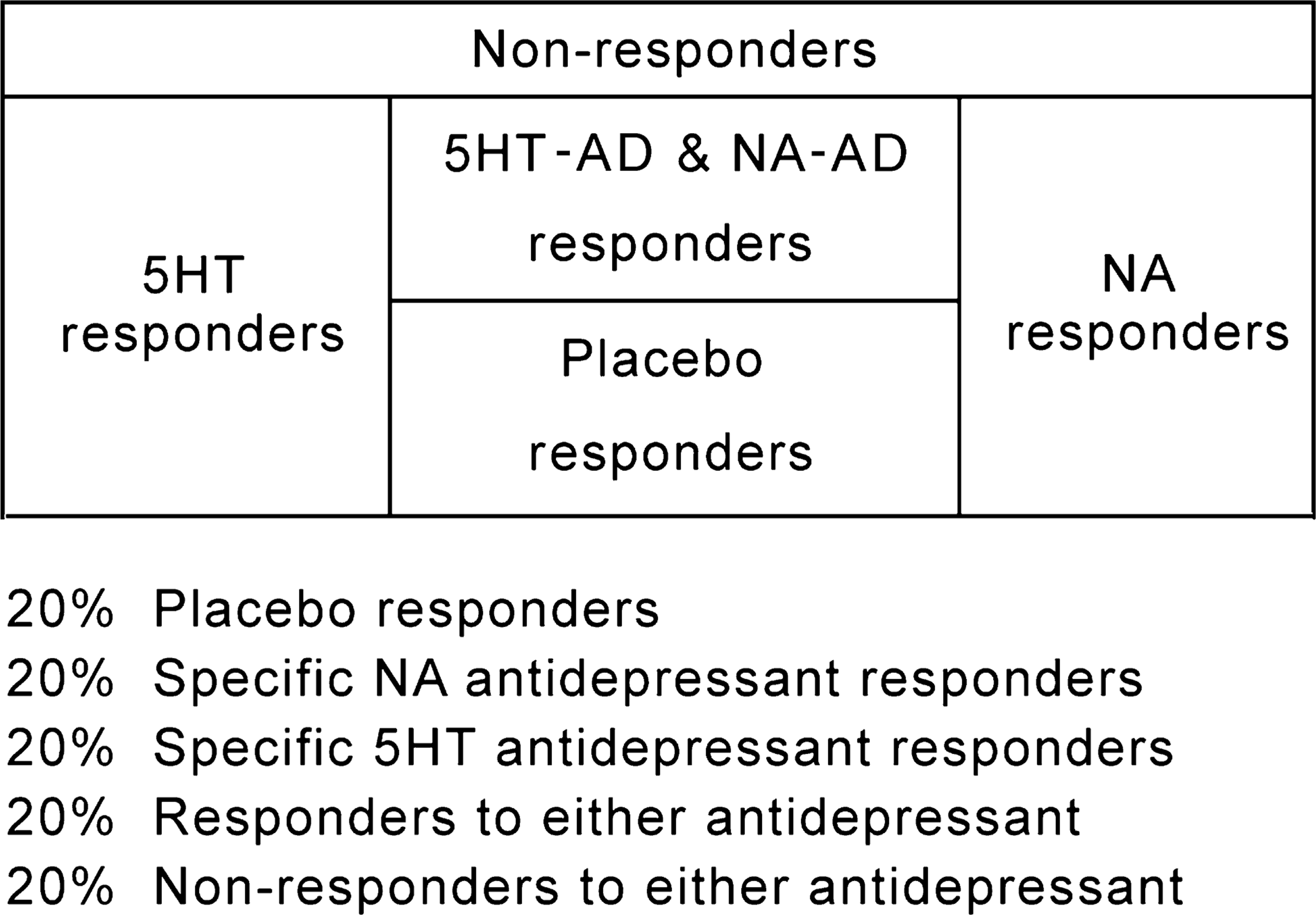
However, within the 60% of responders to one antidepressant, one-third were probably placebo responders, one-third would have responded to any antidepressant and only for one-third did it really matter which drug was administered. Similarly, of the 40% who were nonresponders, half may respond to a different antidepressant, but half may respond to no antidepressant drug. Thus, in a comparison of responders to a serotonergic and noradrenergic antidepressant, two-thirds of each sample will have similar characteristics, and will minimize differences between the responder groups.
The first treatment study examined predictors of response to clomipramine and desipramine in depressed patients [22]. At this time, we had a vacancy in the department and so I approached Dr Roger Mulder who at that time was in his fifth year of the psychiatric registrar training programme. Dr Mulder's interests included the history of psychiatry [23], philosophy [24] and personality [25]. He had not planned on an academic career, but being well read and appropriately sceptical, he had the important ingredients. Thus, with Roger Mulder, Mark Oakley-Browne, Isobel Stevens and Robyn Abbott we assessed and treated the depressed patients, and met regularly to assess interrater reliability with the Structured Clinical Interview for DSM-IIIR (SCID) and depression rating scales.
Relocation
In the late 1980s there was considerable discussion about the organization of Mental Health Services in Christchurch. While the majority of local psychiatrists, including myself, favoured the development of a predominantly ‘specialist’ approach to delivery of mental health services, managers decided that a ‘generalist’ sector-based model should be adopted. I thus moved my clinical work from the psychiatric hospital to the Princess Margaret Hospital (a general hospital) and undertook clinical duties in liaison psychiatry, treating patients in the clinical research unit, and later with eating disorders. At the same time Dr Mark Oakley-Browne developed a specialist anxiety disorders service. With these moves, the CRU moved too. We also then had registrars on rotation through the CRU, which was especially useful in a short-term antidepressant trial. At later times this lapsed as, with long-term treatment trials in depression and with psychotherapy trials, a 6-month rotation is too short a period of time for psychiatric registrars to make a useful contribution. Hopefully, with the College moving the exam earlier, and with a 2-year advanced training period, involvement of registrars in research on rotation will again be more feasible.
Despite my misgivings about the reorganization of local mental health services, the mental health division did fund a clinical psychologist (Frances Carter), as well as a psychiatric nurse (Robyn Abbott) and some psychiatrist time into the developing CRU.
An offspring
A psychiatric registrar contemporaneous with Mark Oakley-Browne was Dr Doug Sellman. Doug Sellman was interested in addictions rather than mood disorders. However, we adapted the clinical, personality and neuroendocrine assessment protocol we were using in our antidepressant trial, and applied it to the study of relapse in men undergoing treatment in an abstinence-focused alcohol treatment programme [26]. Subsequently, Dr Sellman undertook a randomized treatment trial in alcohol dependence [27], and was successful in competing to establish a national centre for treatment development (NCTD) in alcohol, drugs and addiction funded by the Alcoholic Liquor Advisory Council (ALAC).
Contacts
With our growing interest in personality, we established personal contact with Dr Cloninger in St Louis. This led in the first instance to our becoming involved in a large American study on the genetics of alcoholism (and personality). We thus recruited families with two or more members suffering from alcohol dependence, interviewed them with the Diagnostic Interview for Genetic Studies (DIGS) and collected DNA. This was the beginning of a 10-year ongoing collaboration.
An American influence
In the early 1990s Dr Cindy Bulik was appointed as a lecturer in Clinical Psychology at the University of Canterbury. Accompanying her from Pittsburgh was her husband Dr Patrick Sullivan who was partway through his psychiatric residency training. Dr Sullivan thus joined our psychiatric registrar training scheme, then became Health Research Council training fellow and subsequently a senior lecturer in the department. Dr Sullivan made many contributions over the years in Christchurch to both depression and eating disorder studies. Indeed, his progress was noted in the USA, and Dr Ken Kendler (Virginia) offered Dr Sullivan a research position with him that he could not refuse, and that we could not match.
Dr Bulik was interested in eating disorders and joined forces with Frances Carter, Dr Sullivan and me. We received funding to undertake a bulimia treatment study in which we treated all women with cognitive therapy and then randomized them to exposure treatment or relaxation as a control group [28]. Although Dr Bulik was in the Psychology Department at a different university, the CRU hosted the study and we have continued the 5-year follow up of women treated even after Drs Bulik and Sullivan returned to the USA. Dr Bulik felt more at home in a ‘medical’ CRU than in her own department; indeed the Canterbury University Department of Psychology is not alone in holding ambivalent views about the proper setting for Clinical Psychology.
Both Dr Bulik and Dr Sullivan made many useful contributions to the development of the CRU. Pittsburgh, where they came from, is clearly one of the world's leaders in clinical research studies, especially in the area of affective disorders. Usually publications do not give the full picture of how clinical studies are completed. The mechanics that underlie the successful running of clinical studies are complex, and this is not necessarily gleaned from the reports of the studies themselves. Also, in any study a multitude of little (but sometimes important) decisions are made along the way, which are incorporated but not always articulated. Dr Bulik and Dr Sullivan also made major contributions to our expertise in both cognitive therapy and interpersonal psychotherapy. Indeed, Dr Sullivan trained a psychiatric registrar, Dr Sue Luty, who is now the New Zealand representative on the committee of the International Association for Interpersonal Psychotherapy.
Trans-Tasman difference of opinion
Within Australasia, Professor Gordon Parker and the Mood Disorders Unit are the most productive research group in the area of affective disorders. From one of my early papers in psychiatry [29], published when Professor Parker was the editor of the Australian and New Zealand Journal of Psychiarty, he has been very supportive of our research. Professor Parker's Parental Bonding Instrument paper [30] is the most cited paper of the last 50 years from Australasian psychiatric research, and his CORE measure for the assessment of melancholia [31] is another more recent important contribution to affective disorders research. Despite our respect for his work, his ideas on the subtyping of depression [32] have never matched our clinical experience, and seldom our data. Most of our depressed patients have some melancholic features and some have bipolar spectrum disorders. We agree with Parker that DSM-III and IV have not solved the problem of classification in affective disorders, and consider that the ‘American’ devotion to DSM-III and IV has impeded research into better classification systems for affective disorders. We consider, though, that ideas such as those of van Praag are likely to be more fruitful [33, 34]. In a classification system as envisaged by van Praag, depression will be seen as a broad and heterogeneous disorder with fuzzy boundaries. Within this broad category of depression, we will need to map specific functional psychopathology to its underlying neurobiology. Thus, we do not expect there will be a distinct neurobiology for a subtype such as melancholia. We think, however, there may be a distinct neurobiology which underlies non-interactiveness and retardation, a distinct neurobiology of proneness to psychotic symptoms in depression, a distinct neurobiology of anhedonia, suicidality, sleep disturbance, appetite disturbance, etc. After the functional psychopathological symptoms and their underlying neurobiological basis have been identified, there will be the challenge to integrate these systems and understand their interactions and their clinical implications.
Another challenge in piecing together a comprehensive psychoneurobiology of affective disorders will be to understand the interaction of brain and personality development with the functional psychopathology of the clinical syndromes. For instance: why does adolescent depression respond to selective serotonin re-uptake inhibitors (SSRIs) but not tricyclic antidepressants; why are initial insomnia and hypersomnia more common in younger depressed patients; why is depressive pseudodementia seen only in the elderly; why does agitation increase with age; and what is the basis for the marked increase in depressive disorders in females at biological puberty?
A political opportunity
In the early 1990s the then Labour Government announced 10 health goals for the country. Mental health was not included. The Minister of Health was keen for a mental health goal, but apparently ‘nothing was measurable’. This provocation led me to lobby the local Canterbury Health Board about creating a local mental health goal of suicide reduction, and applying for health goals’ money through the Health Department.
Dr Mulder and I organized a planning meeting including Professor Gavin Andrews (Sydney), Professor John Tiller (Melbourne), David Fergusson and Elizabeth Wells (Christchurch). Over two days, the Canterbury Suicide Project was planned. Later, we employed Annette Beautrais to run this study [35], although it stayed separate from other clinical research activities.
Suicide reduction as a national or local mental health goal has considerable political appeal, although whether it is the most sensible community mental health goal is debatable. What is overwhelmingly clear is that affective disorders are clearly the single largest risk factor for suicide, although this major risk factor interacts with a range of other developmental, personality, social and neurobiological factors. While it is sensible to institute a range of measures, including limiting availability of potentially lethal methods, the single approach which has most potential to reduce suicide in a population is the better recognition and treatment of affective disorders. In Christchurch, where antidepressant prescribing, especially of SSRIs, has increased dramatically from the mid-1990s, local suicide rates have reduced by about 30% over the past 5 years. Only time will tell whether this change is sustained and whether this is a national and international phenomenon, or just part of the apparently random fluctuations in suicide rates.
Bringing it together
By 1994 the department had enlarged considerably because of growth in research and in postgraduate teaching. The few offices that the department had at Christchurch Hospital were being threatened with demolition; the CRU was at the Princess Margaret Hospital; and Professor Fergusson's Christchurch Health and Development Study [36], which had moved from Paediatrics to Psychological Medicine a few years before, was in another location. Through the vision and hard work of the departmental administrator, Margo Lukes, the whole department including the clinical research unit and the Christchurch Health and Development Study, moved into a single building (Terrace House) on the Christchurch Hospital site.
Psychotherapy research
The Bulimia Treatment Study (BTS) led by Dr Cindy Bulik, in which we ‘dismantled’ the cognitive and behavioural aspects of cognitive behaviour therapy (CBT) [28], was our first psychotherapy trial. Dr Bulik then suggested a psychotherapy trial in anorexia nervosa, which many of us saw as a challenging undertaking. Although Dr Bulik returned to the USA, a residual core of Gini McIntosh, Dr Frances Carter, Dr Sue Luty, Jenny Jordan, Dr Jan McKenzie and myself, with Leslie Livingstone and later Andrea Bartram as study coordinators, ventured forward. In the Anorexia Treatment Study (ATS), women with anorexia nervosa are randomized to cognitive behaviour therapy, interpersonal psychotherapy [37] or our ‘control’ treatment of specialist supportive care (SSC). Specialist supportive care is good clinical management, with emphasis on education about anorexia, encouragement to eat regular meals and support, but the avoidance of any consistent psychological model across sessions. Recruitment for the anorexia treatment study has been a real challenge, as in most other anorexia clinical trials, but recruitment has finished and results will be available in 2002.
With the experience of the BTS and the ATS underway, and with growing expertise in both cognitive behavioural and interpersonal psychotherapy, the next obvious trial to undertake was of CBT and interpersonal psychotherapy (IPT) in depression. This was funded through the Health Research Council again. Consistent with our interest in understanding which treatment works for which depressed patient, the key research hypotheses are that CBT and IPT will be of comparable efficacy, but patients with avoidant personality disorder and/or high harm avoidance will do better with a cognitive approach, while those with high reward dependence will do better with an interpersonal approach.
Adding molecular genetics
Given our interest in understanding why antidepressant medications work for some patients but not others, it was obvious that we should measure genes that influence antidepressant metabolism. Dr Patrick Sullivan approached a molecular biologist, Dr Martin Kennedy, in the Christchurch Department of Pathology for assistance, and we started collecting DNA in our depressed patients. We soon moved to include looking at genetic polymorphisms for personality traits [38] and other features of depression.
We have more recently received funding to undertake a molecular genetic family study of depression and personality. Another grant under the leadership of Dr Kennedy is to examine how antidepressant drugs alter gene expression in neuronal cells in culture.
In Dunedin, Professor Sarah Romans, Professor Trevor Silverstone, Dr Anne Walshe from Psychological Medicine and Professor Robin Olds from Pathology initiated a study on the molecular genetics of bipolar affective disorder. We became involved as a second site, and between Dunedin and Christchurch over 200 probands with bipolar disorder, as well as over 400 relatives, have been interviewed and DNA collected.
Recently, we held a psychiatric molecular genetics research day, and between the depression and bipolar studies we have more than 10 interesting associations between genetic polymorphisms and clinical phenomena. None involve major genes relevant to the aetiology of bipolar disorder or depression, but the findings reflect our interest in the dissection of psychopathology or antidepressant response. For instance, polymorphisms of the dopamine β hydroxylase gene, which converts dopamine to norepinephrine, may address the issue as to why some depressed patients become paranoid when depressed while others do not; and we have found a polymorphism of p-glycoprotein which may explain why some patients treated with tricyclic antidepressants develop postural hypotension.
Other affective disorder studies
Bipolar disorder remains one of the most fascinating illnesses in all of medicine. We are currently looking at interhemispheric switching; a possible trait marker for bipolar disorder [39], in relationship to bipolar two and bipolar spectrum disorders. Recently we have received funding from the American Stanley Foundation to undertake a study on the problem of weight gain in bipolar patients on valproate. This study involves Dr Jane Elmslie, a dietician, and Dr Richard Porter, a new senior lecturer in the department. Dr Porter has also obtained funding from the Canterbury Medical Research Foundation to look at the paradigm of tryptophan depletion in patients who have recovered from a depressive episode.
Associate Professor Roger Mulder has also developed studies in liaison psychiatry. In conjunction with local gastroenterologists he has shown that interferon, given for hepatitis C, does not produce depressive symptoms, or at most only in those with histories of depression [40]. He and Janet Carter are also involved with the Department of Paediatrics, looking at the prevalence of depression in parents of low birth weight infants.
Philosophy of care and research
The major current sources of funding for the CRU are the Health Research Council of New Zealand via a programme grant, the Christchurch School of Medicine and Health Sciences of the University of Otago through academic and general salary support and building space, and the Mental Health Division of Canterbury District Health through clinical and research staff salaries. While all of the key stakeholders require research outputs, the health service also expects that patients are assessed and treated as an integral part of the deal. However, this need to assess and treat patients has been entirely consistent with our research interests in questions such as which treatments work for which patients.
Guidelines for clinical research insist that the welfare of patients involved in studies should be foremost in the minds of investigators, and that the wellbeing of patients overrides research questions. It is pleasing to see that there are more and more questions being asked about the use of placebos in affective disorder research [41–43]. While placebos will clearly have some role (e.g. in monotherapy vs combination therapy studies) in the future, placebo only in acute treatment studies of disorders where there is good evidence that treatment works is perhaps ethically dubious. Clinically and scientifically there are also issues; in placebo controlled studies, severely ill or suicidal patients are often excluded, which may then limit generalisability of any findings from the studies. Indeed, in the depression treatment study reported in this issue of this journal [44], my colleagues and I were able to include depressed patients of all degrees of severity and suicidality (consistent with outpatient care), as there was no placebo arm in the treatment options. If there had been a placebo option, some patients could not have been included. Perhaps it was easier for us, in that our central research question was understanding which antidepressant works for which patient, than if our key question was that of efficacy.
Another research design that is appropriately being more often challenged is the double blind [45, 46]. The purpose of making studies double blind is to minimize bias. Clearly, if investigators believe that one treatment is better than the other, and these same investigators are using one clinician-based assessment to judge outcome, then bias will not be minimized. However, the use of raters who are blind to treatment allocation (as occurs in our psychotherapy studies, where the double blind is clearly impossible), or the use of multiple measures (e.g. both clinician-rated and patient-rated), by multiple observers at multiple points in time, then bias can be minimized. Indeed single clinician ratings of outcome can be tested for the presence of bias.
There are other situations in which it is also feasible to examine clinician ratings such as in the assessment of axis II personality disorders. Perhaps if accreditation bodies are serious about clinical competence, such research-derived assessments of individual clinicians could be undertaken. However, this may be too threatening for many clinicians, although in research studies evaluation of interrater reliability and of clinician agreement with self-reports are commonly undertaken without individual clinicians feeling especially threatened.
While the need for placebo and the double blind can be challenged, the need for randomization (without bias) is likely to remain of paramount importance.
Recruitment of patients for clinical research studies is fundamental to success, but can be a major stumbling block for many clinical studies. Expecting referrals from a wide range of general practitioners, even if extensive effort is put into education and encouragement, is to court disappointment. Similarly, over a wide range of psychiatric colleagues, the flow of referrals is likely to be meagre. Targeting selected individual clinicians or services is generally more effective; but a research unit must then provide a friendly and rapidly accessible service, and if patients return to referrers they must report on a high quality of care received. We have also taken the view that if patients are referred who turn out to be inappropriate, then we either treat them anyway or ensure and facilitate appropriate referral to another service. For instance, we have had some patients referred for treatment of their depressions, and while we accept patients with bipolar II depression into our treatment studies, we have not included patients with bipolar I depression, as we consider they need a mood stabilizer. Often in these situations, we have commenced them on a mood stabilizer, monitored initial response to treatment, and when they are stable referred them to an appropriate ongoing treatment service. The rationale for this approach is primarily that we think it is in the best interest of the patient, but secondly, it maintains good relationships with referring clinicians.
With our depression studies we have not advertised for patients, as there are doubts about the comparability of referred and advertised-for depressed patients in treatment studies. However, for both our bulimia and anorexia treatment studies we have advertised. In the case of the bulimia treatment study, we were a little surprised by the extent and severity not only of bulimic symptoms, but also of their comorbid axis I and axis II psychopathology. One interesting observation was that a considerable percentage of women with bulimia nervosa refused permission for us to contact or write to their general practitioners, even in situations where they held their general practitioners in high regard. That they answered advertisements for research treatment (by female-only therapists, although some saw male psychiatrists for assessment), but refused that their general practitioners be advised, perhaps reflects both the great distress and the high level of guilt and shame suffered by women with bulimia. Recruitment for our anorexia study has been a challenge, but this appears to be an international phenomenon. As well it probably reflects both the low prevalence of anorexia nervosa, and the denial by many sufferers of anorexia (but not their families and friends who would contact us about referral) that they need treatment.
Conclusion
Issues for clinical research
While many governments, including that of New Zealand, ostensibly encourage evidence-based health care, many policies and practices conspire against the ongoing acquisition of new evidence. In New Zealand, spending on health research is very low, and an increasing number of New Zealand researchers are leaving the country because of an inability to obtain funding. Not only is government spending on health research low, but also New Zealand has little tradition of philanthropy that supports a lot of the research in other countries. Furthermore, the government does not explicitly recognize that teaching hospitals are more expensive than non-teaching hospitals to run, because of their commitments to teaching and research.
Similarly, the New Zealand universities have been squeezed over the past decade, and for medical education the inflation-adjusted income per medical student has consistently declined over each of the last 15 years. This has contributed to a situation where salaries for university clinical staff are considerably less than for hospital clinical staff. In some specialties of medicine this has already created major recruitment and retention issues, which threatens the future of academic medicine in New Zealand.
An earlier government also created Pharmac as a method of controlling expenditure on pharmaceuticals in New Zealand. The approach taken by Pharmac over its years in existence has led predictably to the withdrawal of some pharmaceutical companies from New Zealand, and in many instances has markedly decreased the availability of money for clinical research in this country. In addition to the adverse effects of Pharmac on medical research activities in New Zealand, it is probable that their niggardly approach has considerably compromised the treatment that New Zealanders with mental disorders receive. Finally, the non-availability of an increasing range of modern psychotropic drugs probably adversely affects the ability of New Zealand to recruit and retain psychiatrists from other countries where there is better access to the modern pharmacological options.
Over the past decade where the issues of accountability have increased, there are increasing pressures on academic clinical staff. Each individual must juggle the competing demands on their time for clinical work and maintaining clinical competencies, teaching and producing evidence of competence in teaching, research outputs despite greater difficulties in attracting research money, as well as administration of and service to the institutions and communities in which we work and live. No individual can do full justice on all fronts, and there can always be a sense of not doing all things as well as would be desired. For full-time research staff there are fewer conflicts over the use of time, but this is usually replaced by the uncertainty of future funding. Research will prosper only if research is at the top of the priority list, as all other demands on time may be both more immediate and bring more immediate gratification. Research requires an optimistic expectation that the future can be better, an ability to accept that change takes time, an ability to ignore most of the threats to time for research, and an ability to accept delayed gratification.
For myself, a research-focused career in psychiatry has been a pleasure and a privilege, with remarkably few regrets. For future generations of students who graduate with extensive student loans, who early in their careers would have to accept lower incomes to undertake research, in a political climate that espouses the cause of sound knowledge and good evidence, but which through policies and practices impedes clinical research and the development of new knowledge and of new evidence, it is difficult to recommend a career in research. However, some individuals will be instinctively inquisitive, challenging, and not accepting of current orthodoxies. Hurdles to research have always existed, and individual determination has usually overcome political and institutional impediments. There remains intense satisfaction in making a small contribution to knowledge in a belief that this may ultimately benefit the health of others.
Footnotes
Acknowledgements
Research in the CRU is funded by the Health Research Council of New Zealand, the Christchurch School of Medicine and Health Sciences of the University of Otago, and the Mental Health Division of the Canterbury District Health Board. I thank the many patients who have taught me so much, and who have agreed to participate in our research studies. I thank the many staff who have contributed in a multitude of ways. I especially thank the decade-old cohort of Isobel Stevens (for data management and study coordination), Robyn Abbott (for patient care and sample collection), and my colleague and coinvestigator Associate Professor Roger Mulder.