
Abstract
Objective:
There are mounting calls for bipolar disorder to be managed in primary care, yet the exact prevalence remains unclear. We conducted a meta-analysis to investigate the prevalence of bipolar disorder in general primary care attendees without other comorbid psychiatric diagnosis.
Method:
We systematically searched major electronic databases from inception till 03/2015. Articles were included that reported the prevalence of bipolar disorder determined in line with structured clinical assessment in primary care settings. Two independent authors conducted searches, completed methodological appraisal and extracted data. A random effects meta-analysis and meta-regression were performed.
Results:
Sixteen studies were included accounting for 425,691 participants (mean age = 41.1 years [standard deviation = 7.2 years] 33.3% males). Overall, the global prevalence of bipolar disorder was 1.9% (95% confidence interval = [0.6, 5.4]). The prevalence of bipolar disorder in studies recording a current diagnosis was 3.7% (95% confidence interval = [1.9, 6.0]) and 0.7% (95% confidence interval = [0.2, 1.5]) in studies considering a 12-month period. A diagnosis of bipolar disorder appeared higher in North America (3.7%, 95% confidence interval = [0.9, 8.1]) compared to Europe (0.8%, 95% confidence interval = [0.3, 1.5]). Meta-regression suggests that a more recent publication date (co-efficient = 0.089, 95% confidence interval = [0.0173, 0.1654], z = 2.19, p = 0.01, R2 = 0.21) and younger age of participants (co-efficient −0.0851, 95% confidence interval = [−0.1696, 0.005], z = −1.97, p = 0.04, R2 = 0.24) moderated a higher prevalence of bipolar disorder.
Conclusion:
The global prevalence of bipolar disorder in primary care is 1.9%, with potentially higher prevalence rates in North America compared to Europe. A more recent study publication date is a significant predictor of higher prevalence of bipolar disorder. Potential reasons/drivers of this are considered within the text.
Introduction
Bipolar disorder (BD) is a leading global cause of disability and burden (Vos et al., 2012; Whiteford, 2013). Due to its chronic and fluctuating nature, BD is typically a condition that affects an individual’s quality of life and functioning and necessitates treatment throughout the course of life (Geddes and Miklowitz, 2013). The financial costs associated with BD are profound, for instance, US direct and indirect healthcare expenditure per annum is estimated to be in excess of US$30 billion and US$120 billion, respectively (Jann, 2014). In addition, people with BD have a markedly increased mortality rate (relative risk of 2.00 (95% confidence interval [CI] = [1.70, 2.34], (Walker et al., 2015)) with particularly increased rates of mortality due to physical comorbidities (Hayes et al., 2015).
Given the profound health and societal consequences associated with BD, there is a need to identify those with the condition as early as possible. A primary care setting typically represents the first chronological step for treatment-seeking subjects complaining of mood symptoms (Daigneault et al., 2015). Understanding the prevalence of BD in primary care will assist in attempts to accurately identify and develop appropriately treatment of BD in this setting (Cerimele et al., 2013a). Delays in the diagnosis of BD are associated with greatly increased costs and also worse outcomes for the individual (Jann, 2014). Primary care offers the optimal opportunity for the early recognition of BD for multiple reasons (Cerimele et al., 2014). First, people with BD are at an increased risk for a range of physical comorbidities which are typically managed in primary care, such as diabetes (Vancampfort et al., 2015), pain (Stubbs et al., 2015) and migraines (Fornaro and Stubbs, 2015). Moreover, people with unidentified BD may present with depression rather than mania (Mitchell, 2012), obsessive compulsive disorder (Amerio et al., 2014) and substance use disorders (Merikangas et al., 2008). In addition, BD is often characterized by predominant depressive polarity which may inflate the rates of recall bias and potentially increase the risk misdiagnosis and improper exposure to course-worsening antidepressant monotherapies even in the primary care setting (Manning, 2010; Regeer et al., 2015). In addition, BD could also be over-estimated over unipolar depression (Zimmerman et al., 2010).
Given the need to promptly identify people with BD, a number of screening tools have been developed. Recently, Carvalho et al. (2015) investigated the psychometric properties of the bipolar spectrum diagnostic scale (BSDS), the hypomania checklist (HCL-32) and the mood disorder questionnaire (MDQ). The authors found that while the MDQ is the optimal screening measure, the use of such tools might overinflate the true prevalence of BD. The gold standard required to make a formal diagnosis of BD is with a structured clinical assessment instead (e.g. Diagnostic and Statistical Manual of Mental Disorders [DSM]-5 or International Classification of Diseases [ICD]-10). Recently, Cerimele et al. (2014) conducted an innovative narrative systematic review and found that screening tools (including the MDQ, HCL-32 and BSDS) report higher prevalence of BD (range = 7.6–9.8%) compared to those studies relying on the gold standard structured clinical assessment (range = 0.5–4.3%). Although very helpful, the authors did not conduct a formal meta-analysis to investigate the pooled prevalence of BD in primary care, nor did they investigate subgroup analyses and factors that may account for differences in the prevalence (e.g. geographical variations in BD prevalence). Meta-analyses have the distinct advantage of pooling data from numerous studies in a logical manner to provide a more accurate effect size which is closer to the true prevalence than when individual studies are considered separately (Ioannidis, 2009). Given the burden of BD and increasing calls for this to be identified and managed in primary care settings, we set out to establish the prevalence of BD among general primary care attendees determined only through structured clinical assessment. We planned to conduct subgroup analyses to see if there were geographical variations in the prevalence of BD and where possible conduct meta-regression to consider the impact of important moderators on the pooled prevalence of BD in primary care.
Method
This systematic review was conducted in accordance with the Meta-analysis of Observational Studies in Epidemiology guidelines (Stroup et al., 2000) and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009) following a predetermined but unpublished protocol.
Inclusion and exclusion criteria
We included observational studies (prospective, retrospective or cross-sectional) that: (a) included people with a diagnosis of BD according to a structured clinical assessment using recognised criteria (e.g. DSM-IV [American Psychiatric Association, 2000] or ICD-10 [World Health Organization, 1993]) (b) were conducted in primary care settings including adults (mean age of the sample 18 years and older) without a known comorbid psychiatric diagnosis (e.g. major depressive disorder [MDD], obsessive compulsive disorder). We did not place any language restrictions upon our searches. When we encountered studies reporting data from the same sample at different time points, we used the most recent data and/or the largest data set. When necessary, we contacted study authors to confirm eligibility and/ or to acquire data. We excluded studies conducted using samples of less than 200 participants, in order to increase representativeness of the samples.
Information sources and searches
Two independent reviewers (B.S. and M.F.) searched Academic Search Premier, MEDLINE, Psychology and Behavioural Sciences Collection, PsycINFO, SPORTDiscus, CINAHL Plus and PubMed from inception until March 2015. We used the key words (‘bipolar disorder’ or ‘bipolar*’ or ‘affective disorders’ or ‘mood disorder’) and (‘primary care*’ or ‘primary care physician’ or ‘family medicine’) and (‘prevalence’ or ‘diagnosis’). In addition, the reference lists of all eligible articles and recent narrative systematic reviews on the prevalence of BD in primary care settings were consulted (Cerimele et al., 2013a, 2013b, 2014).
The search term, ‘primary care’, was relied upon, since this encompasses the most recent terminology adopted by the World Health Organization (www.euro.who.int/en/health-topics/Health-systems/primary-health-care/main-terminology).
Study selection
After the removal of duplicates, two independent reviewers screened the titles and abstracts of all potentially eligible articles. Both authors applied the eligibility criteria, and a list of full text articles was developed through consensus. The two reviewers then considered the full texts of these articles and the final list of included articles was reached through consensus.
Data extraction
Two authors (B.S. and M.F.) independently extracted data in a predetermined database. The data collected from each article included: study design, geographical location, details of bipolar participants (mean age, % of males, diagnosis method, details of medications and chronicity of illness) and details regarding diagnosis. In addition, we sought to extract data on the classification of BD (either Type-I, Type-II or Not Otherwise Specified), details regarding medication, Atypical features, Seasonal patterns, Mixed feature, Rapid cyclicity, Previous suicidal attempts and Substance use and other course specifiers whenever available for screening.
Methodological quality assessment
Two authors (B.S. and D.V.) completed methodological quality assessment of included articles using the Newcastle Ottawa Scale (NOS) (Deeks et al., 2003). The NOS is utilized to assess the methodological quality of non-randomized trials and has acceptable validity and reliability (Deeks et al., 2003). The assessment tool focuses on three main methodological features: (a) the selection of the groups, (b) the comparability of the groups and (c) the ascertainment of the outcome of interest. Studies were given a NOS score ranging from 0–9, with a score of 5 or greater indicative of satisfactory methodological quality.
Meta-analysis
We pooled individual study data using DerSimonian-Laird proportion method (DerSimonian and Laird, 1988) with StatsDirect® and Comprehensive Meta-Analysis® software (version 3). Due to anticipated heterogeneity, a random effects meta-analysis was employed. If there were three or more studies with relevant data, we planned to calculate subgroup analyses of the prevalence of BD according to geographical region and duration of BD diagnosis. We also anticipated on conducting separate pooled prevalence of BD according to gender and also classification of BD itself. We assessed publication bias with the visual inspection of a funnel plot (Higgins et al., 2011) and the Begg (Begg and Mazumdar, 1994) and Egger (Egger et al., 1997) tests. Heterogeneity was assessed using Cochran Q statistic (Higgins et al., 2011). Finally, we conducted several meta-regression analyses (if N⩾3) to investigate potential moderators (age, percentage males and date study published) with Comprehensive Meta-Analysis® (version 3).
Results
Search results and study selection
The initial search identified 2215 publications; 18 additional results were identified through other sources, leading to a grand total of 2233 identified studies. After removal of duplicates, 321 abstracts and titles were screened (Figure 1). At the full-text review stage, 98 articles were considered and 82 articles were excluded with reasons (see Figure 1). Thus, 16 articles met the eligibility criteria and were included in the review (Aillon et al., 2014; Ansseau et al., 2004; Carvalho et al., 2014; Gaynes et al., 2010; Ghuloum et al., 2011; Kroon et al., 2013; Liu et al., 2004; Olfson et al., 1997; Philbrick et al., 1996; Serrano-Blanco, 2010; Sorvaniemi and Salokangas, 2005; Spitzer et al., 1994; Szádóczky et al., 1997, 2004; Vermani et al., 2011; Vöhringer et al., 2013). Details regarding the search results including reasons for exclusion of articles are summarised in Figure 1.
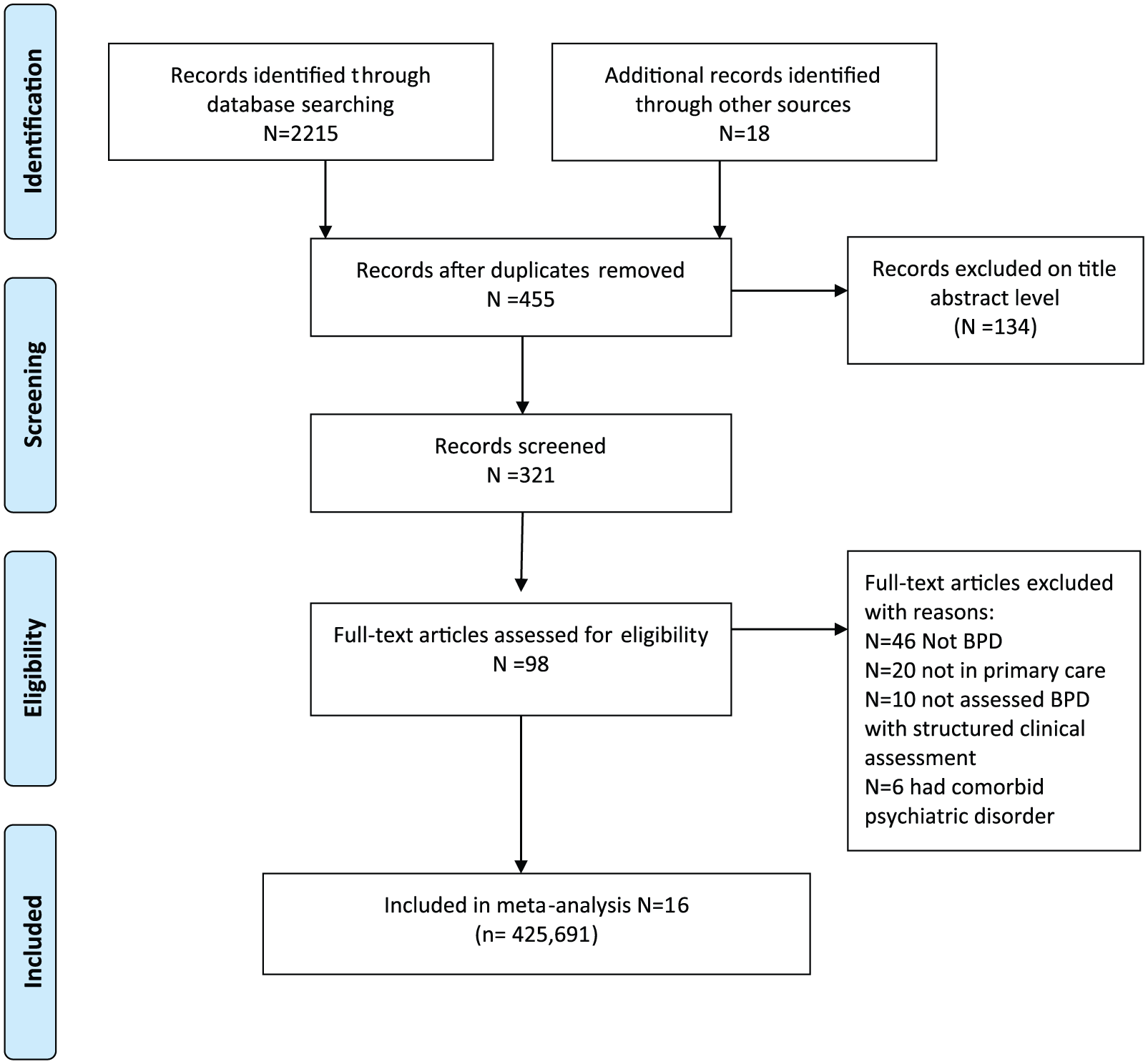
PRISMA 2009 flow diagram for search strategy.
Study and participant characteristics
Across the 16 included studies, 425,691 primary care attendees were represented. The mean age of participants across the studies was 41.1 years (standard deviation [SD] = 7.2 years) and the percentage of males was 33.3%. Six studies were conducted in Europe (Ansseau et al., 2004; Kroon et al., 2013; Serrano-Blanco, 2010; Sorvaniemi and Salokangas, 2005; Szádóczky et al., 1997, 2004) and five were conducted in North America (Gaynes et al., 2010; Olfson et al., 1997; Philbrick et al., 1996; Spitzer et al., 1994; Vermani et al., 2011) The remaining studies included in our analysis were conducted in Taiwan (Liu et al., 2004; Vöhringer et al., 2013), Brazil (Carvalho et al., 2014), Kenya (Aillon et al., 2014) and Qatar (Ghuloum et al., 2011). There was some variation in the time over which BD diagnosis was considered: three studies considered 12-month prevalence (Serrano-Blanco, 2010; Sorvaniemi and Salokangas, 2005; Szádóczky et al., 2004) and eight considered current BD (Aillon et al., 2014; Ansseau et al., 2004; Carvalho et al., 2014; Ghuloum et al., 2011; Liu et al., 2004; Philbrick et al., 1996; Szádóczky et al., 1997; Vermani et al., 2011). A summary of the included studies is included in Table 1.
Summary of included studies.
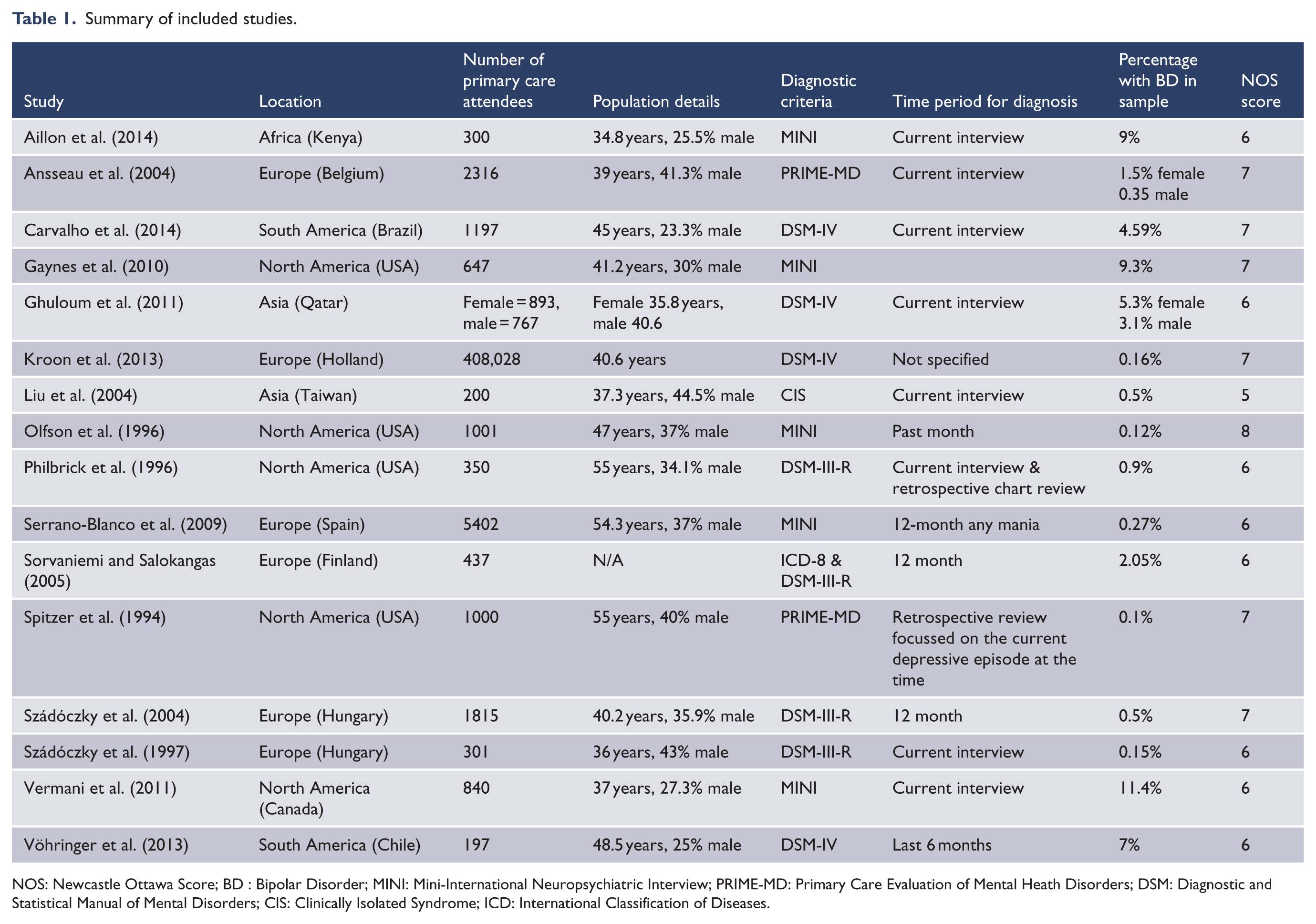
NOS: Newcastle Ottawa Score; BD : Bipolar Disorder; MINI: Mini-International Neuropsychiatric Interview; PRIME-MD: Primary Care Evaluation of Mental Heath Disorders; DSM: Diagnostic and Statistical Manual of Mental Disorders; CIS: Clinically Isolated Syndrome; ICD: International Classification of Diseases.
Methodological quality
The NOS summary score for each article is presented in Table 1. All of the articles were of acceptable methodological quality with an average NOS score 6.0 (range = 5–8).
Meta-analysis of the prevalence of bipolar disorder
The pooled prevalence of BD among 425,691 primary care attendees from 16 unique studies was 1.9% (95% CI = [0.6, 5.4], Q = 1,119, [df = 16], p < 0.001) (Figure 2). The funnel plot was rather asymmetrical (Figure 3) and both the Begg-Mazumdar (Kendall’s tau = 0.39, p = 0.027) and Egger bias test (= 3.988, p < 0.008) indicated some evidence of publication bias. Given the observed publication bias, the pooled prevalence of BD was recalculated using Duval and Tweedie’s trim and fill method establishing a pooled prevalence of 1.9% (95% CI = [0.64, 5.3]). There was insufficient data to conduct subgroup analysis to compare the prevalence of BD classification groups or the prevalence of BD according to gender.
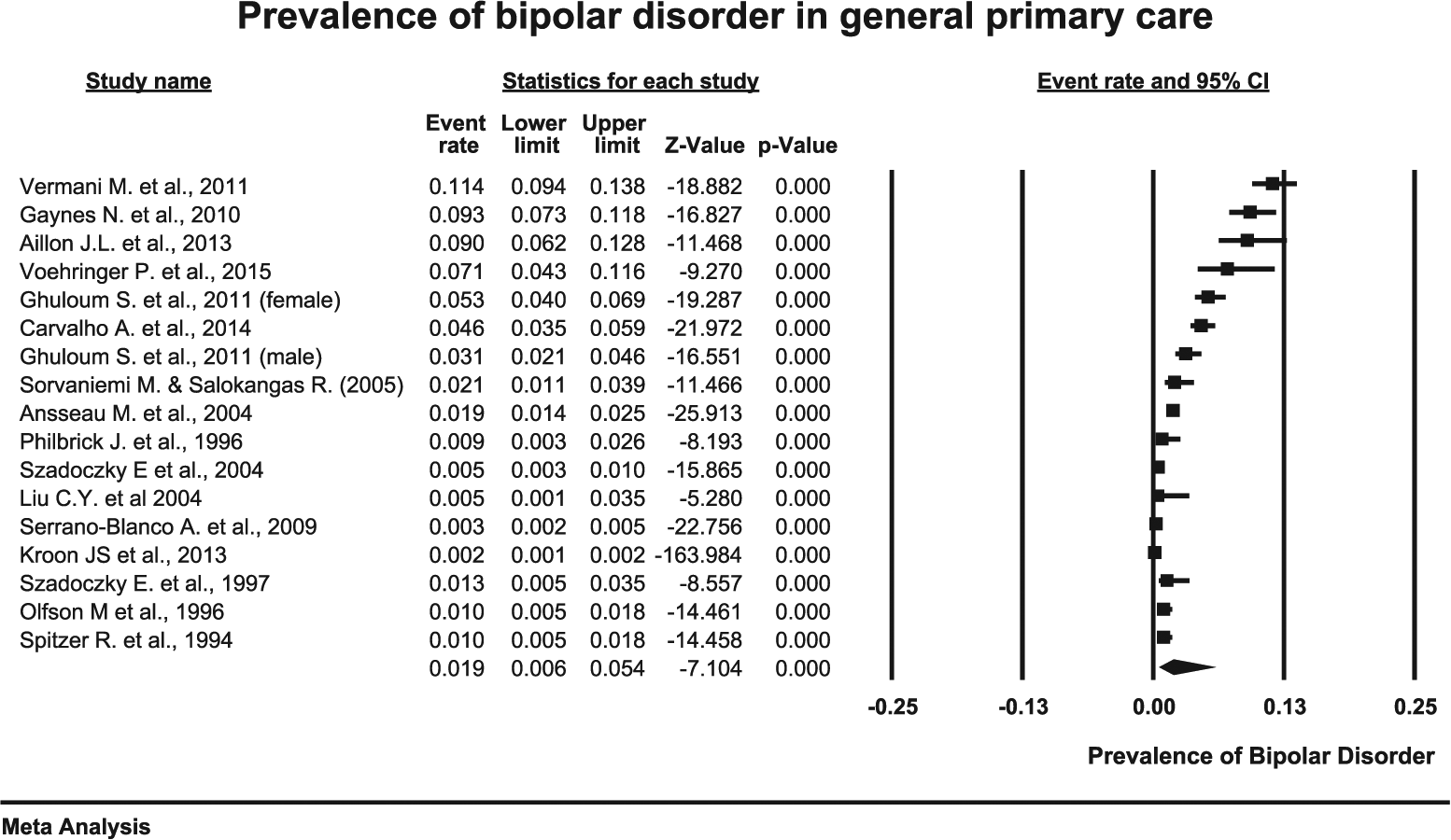
Pooled prevalence of BD in primary care settings among 425,691 attendees.
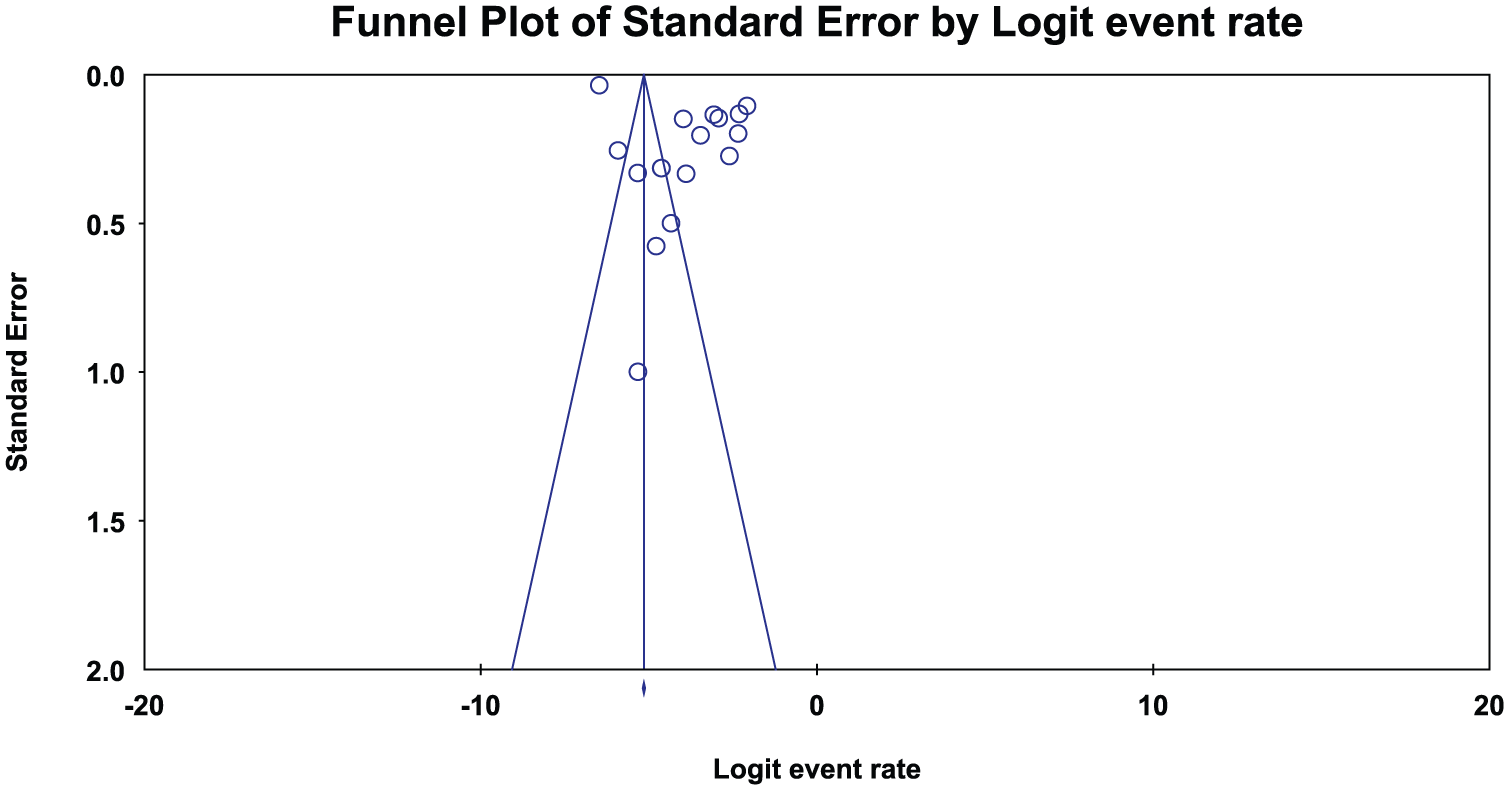
Funnel plot for main analysis.
Meta-regression investigating moderators of the prevalence of bipolar disorder
In order to investigate if the prevalence of BD has changed over time, we conducted a meta-regression analysis using the date of study publication across all 16 studies. The meta-regression analysis established that a more recent study publication year was a significant predictor of a higher prevalence of BD (co-efficient = 0.089, 95% CI = [0.0173, 0.1654], z = 2.19, p = 0.01, R2 = 0.21). There was sufficient data from 15 studies to investigate the influence of mean age on the prevalence of BD. This established that increasing age is associated with a lower prevalence of BD (co-efficient = −0.0851, 95% CI = [−0.1696, 0.005], z = −1.97, p = 0.04, R2 = 0.24). A meta-regression analysis using data from 14 estimates established that the percentage of males in the sample was not related to the prevalence of BD (co-efficient = 0.0357, 95% CI= [−0.0623, 0.1337], z = 0.71, p = 0.45).
Regional prevalence of bipolar disorder
The pooled prevalence of BD among 418,299 primary care attendees was 0.8% (95% CI = [0.3, 1.5], Q = 273, p < 0.01) in six European studies. There was no evidence of publication bias (Begg-Mazumdar: Kendall’s tau = 0.46, p = 0.27). The pooled prevalence of BD in five studies conducted in North America was 3.7% (95% CI = [0.9, 8.1], Q = 191, p < 0.01, Begg-Mazumdar: Kendall’s tau = 0.8, p = 0.08) which was higher than in Europe (z = −59.3, p < 0.01).
Prevalence of bipolar disorder across different time periods
It was possible to pool data from eight studies to establish the pooled current prevalence of BD (Aillon et al., 2014; Ansseau et al., 2004; Carvalho et al., 2014; Ghuloum et al., 2011; Liu et al., 2004; Philbrick et al., 1996; Szádóczky et al., 1997; Vermani et al., 2011). Using these studies, the prevalence of current BD was 3.7% (95% CI = [1.9, 6.0], Q = 157, p < 0.01). The Begg-Mazumdar test did not indicate publication bias (Kendall’s tau = 0.34, p = 0.16) although the Egger test did (= 5.09, p = 0.003). The pooled prevalence of BD over 12 months across three studies was 0.7% (95% CI = [0.2, 1.5], Q = 15, p < 0.01).
Discussion
General findings
Data from the current meta-analysis among 425,691 primary care attendees suggest that the global prevalence of BD is 1.9% (95% CI = [0.64, 5.3] adjusted for publication bias). It appears that when considering a current diagnosis of BD, the actual prevalence is 3.7% (95% CI = [1.9, 6.0]), which is larger than studies considering BD over a 12-month period (0.7%, 95% CI = [0.2, 1.5]). In this regard, it is possible that recall bias by the patients could have influenced the 12-month period studies. This is a pertinent issue since BD patients are prone to a better acknowledgment of previous depressive episodes, rather than previous manic episodes, especially when they experience a current major depressive episode (Karam et al., 2014).
Moreover, the prevalence of BD appears to be higher in studies conducted in North America (3.7%, 95% CI = [0.6, 8.9]) compared to European studies (0.8%, 95% CI = [0.3, 1.5]). While this is in corroboration with previous large, intercontinental cross-sectional study in the general population (Merikangas et al., 2011), to the best of our knowledge, the current work represents the first meta-analytic synthesis in primary care attendees. While a conclusive explanation about this clinically relevant finding is beyond the scope of the present report, we submit that a number of different explanations could be postulated for the higher rates of BD in North America compared to Europe. Specifically, it has been proposed that there is an overall prompter recognition of BD rates even in the primary care setting for the United States vs other countries, essentially based on the claim of a better awareness in the United States about BD by the general population, that may ultimately account for higher rates of specific-treatment seeking patients already occurring at the primary care setting (Fornaro et al., 2009). This may also be perceived as a time-lead bias. Moreover, awareness of disease dovetails closely with stigma in an inverse proportion (Fornaro et al., 2009) with no exception of BD (Levy et al., 2015). That may mean fewer people may be willing to talk about or get treatment for symptoms (Clement et al., 2015), which can lead to lower perceived rates of BD. One possible reason therefore could be that North America has lower levels of stigma associated with BD compared with European countries. However, it was not possible to test this hypothesis within the current data set. In addition, we cannot exclude the chance of ‘sponsor bias’ with respect to the rating tools aimed at increasing the detection of sub-threshold bipolarity in previously diagnosed MDD cases, especially when such rating tools might be directly or indirectly endorsed by the brand at sponsored workshops or education meetings. However, it is not possible to investigate this factor within the current data set.
Of particular interest are the findings within the meta-regression that studies published more recently predicted a higher prevalence of BD (co-efficient = 089, 95% CI = [0.0173, 0.1654], z = 2.19, p = 0.01, R2 = 0.21). While the shift from the DSM-III to DSM-IV criteria could have contributed to this result, an alternative interpretation is that within recent years, clinicians have started to pay greater attention to BD beyond the mere diagnostic guidelines, even in the primary care setting. Once again, this should be particularly true for the North American setting compared to other areas of the world, and for the proportional increase of BD awareness seen in Western Europe vs developing countries, due to common misdiagnoses leading to the under-appreciation of mood disorders in more ‘diagnostically conservative’ regions (Selten and Hoek, 2008). Within the meta-regression analysis, we also established that a higher mean age predicted a lower prevalence of BD (co-efficient = −0.0851, 95% CI = [−0.1696, 0.005], z = −1.97, p = 0.04, R2 = 0.24). The exact reasons for this are unclear but it could possibly resemble the unparalleled increase in BD reported in paediatric populations (Moreno et al., 2007). A more critical view of the higher rates of BD in North America and in those studies published more recently could be attributed to over-diagnosis (Ghouse et al., 2013). However, it is not possible to definitively decipher the possible reasons behind the increasing rates of BD seen in recent studies and in North America. Clarification and understanding the potential reasons and drivers for the elevated prevalence of BD in younger participants, in studies conducted more recently and in those in North America is worthy of future investigation.
Finally, the results of current meta-analysis demonstrate that the prevalence of BD appears to be approximately twice as common as the levels reported in the National Comorbidity Survey Replication studies in the general population (Merikangas et al., 2008). This finding adds weight to the notion that higher numbers of people with BD present to primary care settings and may therefore be an optimal place to identify and manage this group. The current meta-analysis builds upon the previous narrative review by Cerimele et al. (2014) in several ways. First, this study provides the first pooled global prevalence estimate of BD at 1.9%. Second, the current meta-analysis demonstrated there are geographical variations in the prevalence of BD between Europe and North America, which were not established previously. Third, we were able to investigate moderators that may account for the variations in the prevalence of BD.
Limitations
Although this meta-analysis provides novel results, there are a number of limitations which are broadly reflections on the quality within the primary studies. First, there was some heterogeneity encountered within the study design and participants. E.g. most of the original observational studies were over-represented by female participants, which is nonetheless an expected occurrence among those patients seeking primary care attention for ‘depression’ (Maier et al., 1999). Similarly, we did not include any study of BD patients with psychiatric comorbidities, despite the notion that comorbidity is very common in BD (Leinonen and Kampman, 2009). Nonetheless, from a methodological standpoint, this attempted to increase homogeneity, but might have inadvertently reduced the representativeness of our results.
Second, there was no clarity or consensus concerning how the point prevalence of BD was determined by the various relevant studies included in our meta-analysis. We attempted to investigate this by conducting subgroup analyses wherever possible and also conducted meta-regressions in an attempt to better understand this. Third, there was inadequate data to investigate the prevalence of BD according to gender and/or classification of BD, thus precluding subgroup meta-analysis on these important factors. Future research should stratify the results to enable a better understanding of these important relationships. Finally, we encountered some publication bias. We attempted to investigate this by employing the Duval and Tweedie’s trim and fill adjusted prevalence rates separately. Nevertheless, allowing for these caveats, our meta-analysis provides the most systematic quantitative analysis of the prevalence and predictors of the global prevalence of BD in general primary care attendees.
Future research
Future research should seek to understand the reasons for the potential increasing prevalence of BD in recent years, particularly among younger people and in studies conducted in North America. There is a need for randomized control trials to understand if the early identification and management of BD in primary care settings improves the clinical outcomes of people with BD. Future research could address the optimal treatment for primary care patients with BD, and address which patients can be effectively treated in primary care. Moreover, given the concerns regarding the false positive and poor case finding nature of the MDQ, HCL-32 and BSDS, there is a need to develop better strategies to correctly identify those with and without BD in primary care, while not burdening the administering primary care clinician. Greater research focus on integrated, concurrent treatment for BD and chronic physical diseases is also required, given the high levels of physical comorbidities in this group.
Conclusion
Approximately 1.9% of general primary care attendees have BD according to a structured clinical assessment. It appears BD diagnoses are elevated in North America compared to Europe. Finally, the results of the meta-regression suggest that BD diagnoses are becoming more common in primary care in recent years, particularly among younger adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: DV is funded by the Research Foundation – Flanders (FWO-Vlaanderen).